Helicobacter pylori
and anemia: a community-based
cross-sectional study among adults
in Southern Brazil
Helicobacter pylori
e anemia: um estudo
transversal de base populacional entre
adultos no Sul do Brasil
1 Programa de Pós-graduação em Epidemiologia, Universidade Federal de Pelotas, Pelotas, Brasil. 2 Facultad de Farmacia y Bioquímica, Universidad de Buenos Aires, Buenos Aires, Argentina.
Correspondence G. C. Minten
Programa de Pós-graduação em Epidemiologia, Universidade Federal de Pelotas.
Rua Marechal Deodoro 1160, 3o piso, C.P. 464, Pelotas, RS 96020-220, Brasil. [email protected]
Iná S. Santos 1
Gicele Costa Minten 1
Neiva C. J. Valle 1
Giovana Costa Tuerlinckx 1
José Boccio 2
Domingo Andrés Barrado 2
Alessandra Banaszeski da Silva 1
Guilherme Augusto Reissig Pereira 1
Abstract
To investigate the association between Helico-bacter pylori and anemia, a community-based cross-sectional study was conducted among 18-45 year old users of the 31 primary health care units in Pelotas, Southern Brazil. Interviews us-ing a structured questionnaire were carried out in waiting rooms during two work shifts. Anemia (hemoglobin < 11g/dL among pregnant women, < 12g/dL among women and < 13g/dL among men) was diagnosed from capillary blood (HemoCue) and H. pylori by means of a 13C-UBT.
Information on socio-demographic, behavioral and biological characteristics was collected. Lo-gistic and linear regression analyses were car-ried out, taking into account aggregated primary health care units. A total of 1,117 respondents ful-filled the inclusion criteria (losses/refusals: 8.1%). Prevalence of anemia was 20.6% (18.2-23.2%) and of H. pylori, 70.7% (68.0-73.6%). After allowing for age, sex and skin color the odds ratio for ane-mia among those who were diagnosed H. pylori
positive was 0.94 (0.70-1.27). After allowing for sex, skin color, family monthly income, age, and smoking, the reduction in hemoglobin among
H. pylori positive respondents was 0.07g/dL (-0.24-0.11; p = 0.4). There is no association be-tween H. pylori and anemia among adults attend-ing primary health care units in Southern Brazil.
Helicobacter pylori; Anemia; Adult
Background
Identification of the effect of Helicobacter pylori
on the digestive system has given rise to studies of the risk factor of this infectionfor extra-gastric diseases. It has been proposed that H. pylori may be responsible for iron deficiency, among other risks. The factors that lend biological plausibility to this association include the deficiency in iron absorption by H. pylori-colonized gastric cells,
competition for iron between gastric cells and H. pylori, and bleeding through peptic ulcers and other gastric lesions associated with H. pylori1,2.
Anemia is a major public health problem in developing countries. The main causes of ane-mia include: dietary iron deficiency; infectious diseases such as malaria, hookworm infections and schistosomiasis; deficiencies of other key mi-cronutrients including folate, vitamin B12 and vi-tamin A; and inherited conditions that affect red blood cells, such as thalassaemia. Nonetheless, about half of all cases of anemia can be attributed to iron deficiency 3. Accordingly, if an association between H. pylori and anemia is demonstrated, eradication of this bacterium could become an important public health strategy for controlling anemia in developing countries.
Methods
This was a community-based cross-sectional study carried out in all 31 primary health care fa-cilities within the Unified National Health System (SUS) in the urban area of the municipality of Pelotas between August 2006 and February 2007. The study included adults aged 18 to 45 who were present in waiting rooms for consultations for any reason, and also the accompanying persons, provided that they too were users of the city’s pri-mary health care facilities.
Two pairs of interviewers received prior train-ing to apply standardized pre-coded question-naires, take anthropometric measurements and carry out two tests on the interviewees: HemoCue (HemoCue Corp., Ängelholm, Sweden) and 13 C-Urea Breath Test (13C-UBT; Fischer Analysen In-strumente GmbH, Leipzig, Germany). The proce-dures were implemented during two work shifts of each primary health care unit (two mornings on two consecutive days).
Those who fulfilled the eligibility criteria and agreed to participate were required to complete a structured questionnaire on demographic (age, sex and skin color), socio-economic (fam-ily monthly income, marital status and school-ing) and behavioral characteristics (smoking and consumption of alcoholic drinks, greens/raw vegetables, beans, eggs/yolks, meat and viscera). Current or previous medical diagnoses of ane-mia and hemorrhoids, and report of blood in fe-ces were also investigated. In the case of female respondents, additional questions were asked regarding reproductive and menstrual charac-teristics (number of previous pregnancies, age at menarche, duration of menstrual flow, and cur-rent contraceptive method).
An aluminum anthropometer of 1cm accu-racy and a UNICEF (United Nations Children Fund) dry balance of 100g accuracy and 150kg capacity were used for anthropometric measure-ments. The body mass index (BMI) was calcu-lated as the person’s weight (in kg) divided by the square of their height (in meters). Quality control to check reliability of some of the questions was done by means of applying a reduced question-naire by telephone to approximately 10% of the interviewees, selected randomly. The kappa sta-tistic of agreement with a previous diagnosis of anemia was 0.80.
Anemia was assessed by measuring the he-moglobin in capillary blood by means of a por-table hemoglobin meter (HemoCue): < 11g/dL in pregnant women; < 12g/dL in non-pregnant women; and < 13g/dL in men 3.
Because fasting for at least six hours was re-quired, the 13C-UBT was performed in the morn-ing of the day followmorn-ing the interview. Individuals with Del 13 PDB variation between air samples before and after dosing that was greater than 3.5 per mil were defined as H. pylori-positive 4.
For sample size calculation, the following pa-rameters were set: alpha 0.05, power 80%, ratio of exposed to non-exposed of 3:1, relative risk ≥ 2.0 and anemia prevalence among non-exposed of 10%. In accordance with these parameters, and adding 15% for losses and refusals and 30% for controlling for confounding, a sample size of 909 individuals was needed.
All the analyses took into account the cluster-ing of the data in primary health care facilities. Multivariable analyses included variables associ-ated with anemia and the presence of H. pylori
with p-values < 0.20. Crude and adjusted odds ratios (OR) were obtained with their respective 95% confidence intervals (95%CI) by means of logistic regression. Hemoglobin was also ana-lyzed as a continuous variable through linear re-gression. The analyses were performed using the Stata 9.0 software (Stata Corp., College Station, United States).
The study was approved by the Research Eth-ics Committee at the School of Medicine of the Federal University of Pelotas and by the Munici-pal Department of Health and Social Wellbeing of Pelotas. Before enrollment, the participants signed an informed consent form. The results from the tests were forwarded to respective doc-tors to consider necessary treatment.
Results
A total of 1,554 adults attended the 31 primary health care units during the two work shifts of the fieldwork. Of these, 432 were ruled out for not meeting the age criterion and five on account of physical and/or mental disabilities. There were 91 losses and refusals, corresponding to an over-all no-response rate of 8.1%.
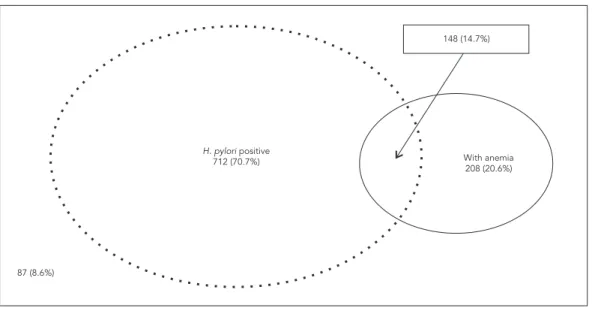
The HemoCue test was administered to 1,007 individuals. Prevalence of anemia was 20.6% (95%CI: 18.2-23.2%). Among the 1,001 partici-pants who underwent the 13C-UBT, the preva-lence of H. pylori colonization was 70.7% (95%CI: 68.0-73.6%). As shown in Figure 1, 14.7% of the individuals presented both H. pylori infection and anemia.
twice as high (p < 0.001). There were no statis-tically significant differences in anemia preva-lence in relation to the other socio-demographic variables. Among all the consumption variables, anemia was only associated with consumption of black beans (p = 0.04), with the prevalence be-ing higher among individuals who reported daily consumption.
Table 2 shows the sample distribution and anemia prevalence according to current or past reported morbidity. The prevalence of anemia was associated with a history of a current or previ-ous medical diagnosis of anemia. The HemoCue test was positive for 23.4% of the individuals who reported present or past anemia versus 16.4% among those with no history of anemia (p = 0.01). The reproductive and menstrual characteristics of the female subjects are also shown in Table 2. No statistically significant association between any of the reproductive or menstrual variables and the anemia prevalence was observed.
There was no difference in anemia prevalence between the H. pylori-positive and negative indi-viduals. In both groups, the anemia prevalence was around 21% (Table 2).
Table 3 shows the results from crude and adjusted analyses of the association between H. pylori and anemia. In comparison with the H. pylori-negative individuals, taken as a reference group, the crude OR for the H. pylori-positive
was 1.02 (95%CI: 0.75-1.39). Inclusion of age, sex and skin color variables did not change this result (adjusted OR = 0.94; 95%CI: 0.70-1.27).
The effect of H. pylori colonization on the he-moglobin level was also assessed, taking the latter as a continuous variable. Crude multilevel linear regression showed that H. pylori was associated with a statistically non-significant reduction of 0.17g/dL (95%CI: -0,38-0,05; p = 0.12) in the he-moglobin level. After allowing for sex, skin color, income, age, and smoking, the reduction was even smaller: the hemoglobin level of H.
pylori-positive individuals was 0.07g/dL (95%CI: -0,24-0,11; p = 0,4) lower than that observed among the
H. pylori negative.
Discussion
In this study no association was found between
H. pylori colonization and anemia. The observed anemia prevalence (20.7%) in the present study was moderate and similar to what has been de-scribed in other locations in Brazil 5,6. The preva-lence of H. pylori colonization was high (70.7%) and consistent with the findings from a previous study carried out in the same city 7. No associa-tion was observed between the colonizaassocia-tion and the presence of anemia. Before discussing the significance of this finding, the particularities Figure 1
Table 1
Anemia prevalence according to socio-demographic and behavioral variables. Pelotas, Southern Brazil, 2007.
Variable n (1,026) Anemia prevalence (%) p value
Age (years) 0.21
18-24 244 61 (25.0)
25-29 180 36 (20.0)
30-34 190 40 (21.1)
35-39 179 26 (14.5)
40-45 214 45 (21.0)
Sex 0.12
Male 161 25 (15.9)
Female 865 183 (21.5)
Skin color < 0.001
White 749 124 (16.6)
Black/Mixed 258 84 (32.6)
Income (as a multiple of the minimum wage) 0.94
≤ 1.0 208 43 (20.7)
1.01-2.0 400 81 (20.3)
2.01-3.0 195 43 (22.1)
> 3.0 203 41 (20.2)
Education level (number of years) 0.78
0-4 213 42 (19.7)
5-8 460 102 (22.2)
≥ 9 334 64 (19.2)
Alcohol consumption 0.89
No 829 172 (20.7)
Yes 178 36 (20.2)
Smoking 0.34
No 471 108 (22.9)
Former smoker 209 40 (19.1)
Yes 327 60 (18.3)
Chicken/beef consumption (days/week) 0.93
< 1 28 7 (25.0)
1-3 229 47 (20.5)
4-6 103 17 (17.5)
7 647 137 (21.2)
Chicken/cow liver consumption (days/week) 0.29
< 1 808 161 (19.9)
≥ 1 199 47 (23.6)
Egg/yolk consumption (days/week) 0.95
0 461 95 (20.6)
1-3 461 95 (20.6)
≥ 4 85 18 (21.2)
Black bean consumption (days/week) 0.04
< 3 225 36 (16.0)
4-6 110 19 (17.3)
7 672 153 (22.8)
Green leaf vegetable consumption (days/week) 0.97
< 1 256 58 (22.7)
1-3 464 88 (19.0)
4-6 78 16 (20.5)
Table 2
Anemia prevalence according to biological variables. Pelotas, Southern Brazil, 2007.
Variable n (1,026) Anemia prevalence (%) p value
History of anemia 0.01
No 391 64 (16.4)
Yes (present/past) 616 144 (23.4)
History of hemorrhoids 0.64
No 893 187 (20.9)
Yes 112 21 (18.8)
History of blood in feces 0.40
No 872 185 (21.2)
Yes 135 23 (17.0)
Body mass index 0.46
≤ 24.9 545 119 (21.8)
25.0-29.9 284 55 (19.4)
≥ 30.0 177 34 (19.2)
Age at menarche (years) * 0.41
≤ 11 214 46 (21.5)
10-14 539 110 (20.4)
≥ 15 94 25 (26.6)
Number of previous pregnancies * 0.40
0 91 14 (15.4)
1-3 596 135 (22.7)
≥ 4 161 34 (21.1)
Contraceptive method * 0.06
Pill 413 85 (20.6)
IUD/Tubal ligation/Injectable hormones 171 27 (15.8)
Others 233 62 (26.6)
Mean duration of menstrual periods (days) * 0.41
1-4 519 112 (21.6)
5-7 308 70 (22.7)
≥ 8 23 1 (4.3)
Helicobacter pylori (13C-UBT) 0.90
Negative 292 60 (20.5)
Positive 709 148 (20.9)
IUD: intra-uterine device. * Women only (n = 865).
and the possible limitations of the present study need to be considered.
Firstly, this investigation was developed among the users of primary health care units and therefore the sample was not representative of the population of the city as a whole. The pri-mary health care units serve the poorest 30% of the population living in the urban zone of the city 8. However, since the objective of the study was to verify whether there was an association between H. pylori colonization and anemia, this non-representativeness does not constitute a true limitation to the study 9. Furthermore, the fact of belonging to the same socio-economic
stratum brings a high homogeneity to the sample regarding socio-economic and behavioral char-acteristics which may possibly be responsible for the lack of association observed between those variables and the occurrence of anemia.
Secondly, there was a higher prevalence of women in the sample studied. It is well known that women use health services more than men 8,10,11. As demonstrated in other investigations,
pro-portion of men in this sample than in the general population, which may have caused the anemia estimate to be less accurate for this group. On the other hand, regarding H. pylori colonization prevalence, a previous study among the general population of the same city showed no difference between men and women 7.
Thirdly, identification of anemia by means of the hemoglobin level may have impaired the capacity of detection of iron-deficiency anemia. Not all anemic individuals are iron deficient and iron deficiency may occur without anemia. Al-though hemoglobin concentration can provide information about the severity of iron deficiency, measurements of serum ferritin and transferring-receptor provide the best approach for measuring the iron status of populations. In settings where infectious diseases are common, serum ferritin is not a useful indicator because inflammation leads to a rise in serum ferritin levels as a result of the acute phase response to the disease. In general the transferring-receptor level does not rise in response to inflammation so that, when combined with serum ferritin, it is possible to distinguish between iron deficiency and inflam-mation. This methodological approach however still requires validation in population surveys 12 and in the absence of international agreement on how to assess the iron status of populations, the prevalence of iron deficiency has often been de-rived from the prevalence of anemia using mea-surements of blood hemoglobin, even though not all anemia is caused by iron deficiency.
The three largest population-based preva-lence studies conducted worldwide found con-flicting results with regard to the association be-tween H. pylori and iron deficiency. Milman et al. 13 conducted a cross-sectional population-based study among adults (30-60 years of age) selected at random from the Civil Registration System in Denmark. A total of 4,581 persons were invited to a health examination, of which 78% accepted to participate and 3,608 entered the survey. The authors found no association between anti-H.
pylori antibodies and anemia (low hemoglobin levels). However, the probability of low body iron stores (median serum ferritin) was higher among positive individuals than among the sero-negative, after controlling for confounding.
A random sample of 2,080 stored sera avail-able from a previous study conducted among Alaska Natives residing in Alaska were tested for IgG antibody to H. pylori by Parkinson et al. 14. Overall, an association was observed between
H. pylori sero-positivity and low serum ferritin levels after adjusting for age and sex (RR: 1.39; p = 0.055), whereas in the same subjects, H. py-lori detected by 13C-UBT or fecal antigen test was not 15.
In the United States, Cardenas et al. 16 used data from the 1999-2000 National Health and Nutrition Examination Survey (NHANES), with 7,462 individuals aged ≥ 3 years. Association be-tween sero-positivity for H. pylori and iron defi-ciency (lower serum ferritin level -13.9%; 95%CI: -19.5;-8.0%), iron deficiency anemia (OR = 2.6; 95%CI: 1.5-4.6), and other types of anemia (OR = 1.3; 95%CI: 1.0-1.7) were observed after adjusting for confounders.
The number of randomized trials carried out to test the effect of H. pylori eradication among individuals with iron deficiency anemia, with or without the use of iron salts, is still small. Most of these trials found an improvement in iron stores and correction of the anemia, but they were gen-erally conducted with small numbers of partici-pants 17,18,19. The biggest randomized trial found in the literature up to the present date was car-ried out by Gessner et al. 20 in Alaska in 2006. This involved 219 children aged 7-11 years who pre-sented iron deficiency and in whom no associa-tion was found between H. pylori eradication and improvement in ferritin levels or anemia. Table 3
Effect of Helicobacter pylori colonization over prevalence of anemia. Pelotas, Southern Brazil, 2007.
Variable OR 95%CI p value
H. pylori colonization
Crude 1.02 0.75-1.39 0.90
Adjusted * 0.94 0.70-1.27 0.69
Conclusion
This study has produced no evidence to support the hypothesis that H. pylori contributes to ane-mia among users of the SUS in Southern Brazil. This lack of association after ruling out the role of bias and confounding argues against the inclu-sion of H. pylori among the potential risk factors for iron deficiency anemia in Brazil.
Resumo
Helicobacter pylori tem sido apontado como causa de anemia. Para investigar essa associação, estudo trans-versal de base populacional foi realizado entre adultos (18-45 anos de idade), usuários das 31 unidades bási-cas de saúde (UBS), em Pelotas, Sul do Brasil. Entre-vistas com questionários estruturados foram feitas nas salas de espera, em dois turnos de trabalho. Anemia (hemoglobina < 11g/dL entre gestantes, < 12g/dL entre mulheres adultas e < 13g/dL entre homens) foi diag-nosticada em sangue capilar (HemoCue). H. pylori foi identificado por 13C-Urea Breath Test. Foram coleta-das informações sócio-demográficas, comportamen-tais e biológicas. Análise por regressão logística e line-ar, levando em conta a agregação por UBS. Dos 1.117 elegíveis, foram perdidos ou recusaram-se participar 8,1%. A prevalência de anemia foi 20,6% (18,2-23,2%) e H. pylori, 70,7% (68,0-73,6%). Após ajuste para ida-de, sexo e cor, a odds ratio para anemia entre H. pylori
positivos foi 0,94 (0,70-1,27). Na análise ajustada para sexo, cor, renda familiar, idade e tabagismo, o nível de hemoglobina foi 0,07g/dL menor (-0,24-0,11; p = 0,4) entre H. pylori positivos. Não há associação entre
H. pylori e anemia entre adultos usuários de UBS no Sul do Brasil.
Helicobacter pylori; Anemia; Adulto
Contributors
I. S. Santos conceived the study and participated in its design, coordination, analyses, and interpretation of the results, and drafted the manuscript. G. C. Minten and G. C. Tuerlinckx participated in the design of the study, planned the logistics for the data collection, and coordinated the field work. N. J. C. Valle performed the statistical analyses. J. Boccio and D. A. Barrado carried out the laboratory analyses for 13 C-UBT tests. A. B. Silva and G. A. R. Pereira participated in the coordination of the study, edited the data set and performed prelimi-nary analyses. All authors read and approved the final manuscript.
Acknowledgments
References
1. Bini EJ. Helicobacter pylori and iron deficiency ane-mia: guilty as charged? Am J Med 2001; 111:495-7. 2. DuBois S, Kearney DJ. Iron-deficiency anemia and
Helicobacter pylori infection: a review of the evi-dence. Am J Gastroenterol 2005; 100:453-9. 3. World Health Organization/United Nations
Uni-versity/United Nations Children Fund. Iron defi-ciency anaemia: assessment, prevention, and con-trol. A guide for programme managers. Geneva: World Health Organization; 2001.
4. Zubillaga M, Oliveri P, Panarello H, Buzurro M, Ad-ami J, Goldman C, et al. Stable isotope techniques for the detection of Helicobacter pylori infection in clinical practice. 13C-Urea Breath Test in different experimental conditions. Acta Physiol Pharmacol Ther Latinoam 1999; 49:101-7.
5. Batista Filho M, Rissin A. A transição nutricional no Brasil: tendências regionais e temporais. Cad Saúde Pública 2003; 19 Suppl 1:S181-91.
6. Fabian C, Olinto MTA, Dias-da-Costa JS, Bairros F, Nácul LC. Prevalência de anemia fatores associa-dos em mulheres adultas residentes em São Leo-poldo, Rio Grande do Sul, Brasil. Cad Saúde Públi-ca 2007; 23:1199-205.
7. Santos IS, Boccio J, Santos AS, Valle NC, Halal CS, Bachilli MC, et al. Prevalence of Helicobacter py-lori infection and associated factors among adults in Southern Brazil: a population-based cross-sec-tional study. BMC Public Health 2005; 5:118. 8. Dias-da-Costa JS, Facchini LA. Utilização de
servi-ços ambulatoriais em Pelotas: onde a população consulta e com que freqüência. Rev Saúde Pública 1997; 31:360-9.
9. Rothman KJ, Greenland S. Modern epidemiology. 2nd Ed. Philadelphia: Lippincott-Raven; 1998. 10. Capilheira MF, Santos IS. Fatores individuais
asso-ciados à utilização de consultas médicas por adul-tos. Rev Saúde Pública 2006; 40:436-43.
11. Mendoza-Sassi R, Béria JU. Utilización de los ser-vicios de salud: una revisión sistemática sobre los factores relacionados. Cad Saúde Pública 2001; 17:819-32.
12. Joint World Health Organization/Centers for Dis-ease Control and Prevention Technical Consulta-tion on the Assessment of Iron Status at the Popu-lation Level. Assessing the iron status of popula-tions. Geneva: World Health Organization/Centers for Disease Control and Prevention; 2004.
13. Milman N, Rosenstock S, Andersen L, Jorgensen T, Bonnevie O. Serum ferritin, hemoglobin, and
Helicobacter pylori infection: a seroepidemiologic survey comprising 2794 Danish adults. Gastroen-terology 1998; 115:268-74.
14. Parkinson AJ, Gold BD, Bulkow L, Wainwright RB, Swaminathan B, Khanna B, et al. High prevalence of Helicobacter pylori in the Alaska native popula-tion and associapopula-tion with low serum ferritin levels in young adults. Clin Diagn Lab Immunol 2000; 7:885-8.
15. Baggett HC, Parkinson AJ, Muth PT, Gold BD, Gess-ner BD. Endemic iron deficiency associated with
Helicobacter pylori among school-aged children in Alaska. Pediatrics 2006; 117:e396-404.
16. Cardenas VM, Mulla ZD, Ortiz M, Graham DY. Iron deficiency and Helicobacter pylori infection in the United States. Am J Epidemiol 2006; 163:127-34. 17. Choe YH, Kim SK, Son BK, Lee DH, Hong YC, Pai
SH. Randomized placebo-controlled trial of He-licobacter pylori eradication for iron-deficiency anemia in preadolescent children and adolescents. Helicobacter 1999; 4:135-9.
18. Ciacci C, Sabbatini F, Cavallaro R, Castiglione F, Di Bella S, Iovino P, et al. Helicobacter pylori impairs iron absorption in infected individuals. Dig Liver Dis 2004; 36:455-60.
19. Valiyaveettil AN, Hamide A, Bobby Z, Krishnan R. Effect of anti-Helicobacter pylori therapy on out-come of iron-deficiency anemia: a randomized, controlled study. Indian J Gastroenterol 2005; 24:155-7.
20. Gessner BD, Baggett HC, Muth PT, Dunaway E, Gold BD, Feng Z, et al. A controlled, household-randomized, open-label trial of the effect that treatment of Helicobacter pylori infection has on iron deficiency in children in rural Alaska. J Infect Dis 2006; 193:537-46.
Submitted on 09/Oct/2008