Rev. LatinoAm. Enfermagem vol.24
Texto
Imagem
Documentos relacionados
Nesse momento, defendemos as seguintes hipóteses: compreendemos que a EA é um tema de real importância na construção de conhecimentos e na formação de cidadãos conscientes,
Nota-se que o emprego das tecnologias de informação e comunicação na disciplina de química torna a abordagem de vários conteúdos antes considerados complexos e difíceis pelos
Factors associated with use of community mental health services by schizophrenia patients using multilevel analysis.. BMC Health
We identified high prevalence of MS in adult and elderly population in Brazil, being associated with sociodemographic variables (age, schooling, conjugal status and housing region),
Abstract Objectives: Evaluate the prevalence of self-reported hypertension in adults aged 20 to 59 years as well as identify associated factors, the use of health services
ABSTRACT: Objective: To estimate the prevalence and check the factors associated with access to prescribed medicine by the Brazilian adult population; and to describe the
Lifetime use of illicit drugs is associated with current and lifetime consumption of tobacco and alcoholic beverages and is reported to be 7.84 times more common among students
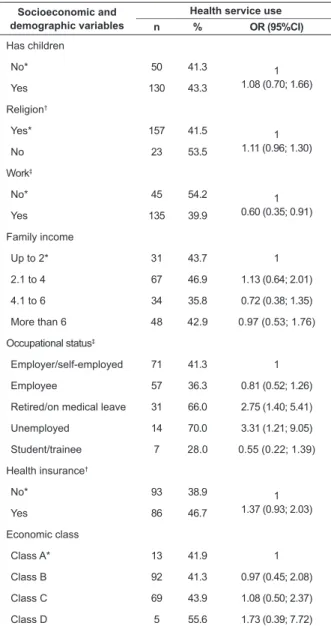
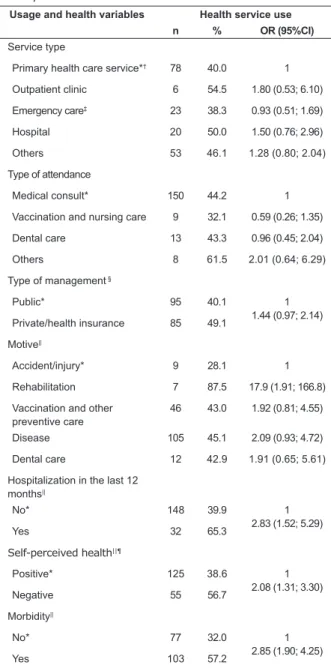
Prevalence of drug use, by gender, according to behavioral variables related to health and use of health services in the adult population (20 years or older) of Campinas in
