REVISTA
BRASILEIRA
DE
REUMATOLOGIA
www . r e u m a t o l o g i a . c o m . b r
Brief
communication
The
dermatoscopy
in
the
skin
pathergy
testing:
case
series
in
patients
with
suspected
Behc¸et’s
Disease
Maria
Antonieta
Rios
Scherrer
a,
Lúcia
Porto
Fonseca
de
Castro
b,
Vanessa
Barreto
Rocha
a,∗,
Leonardo
Pacheco
aaAmbulatóriodeDermatologia,HospitaldasClínicas,UniversidadeFederaldeMinasGerais,BeloHorizonte,MG,Brazil bDepartamentodeAnatomiaPatológicaeMedicinaLegal,UniversidadeFederaldeMinasGerais,BeloHorizonte,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received9November2013 Accepted12June2014
Keywords:
Behc¸etdisease
Diagnostictechniquesand procedures
Vasculitis
a
b
s
t
r
a
c
t
Behc¸et’sdiseaseisamultisystemicdiseaseconsistingofavaryingcombinationofocular, mucocutaneous,neurologic,cardiovascular,gastrointestinalandothermanifestations.Its diagnosisisbasedonclinicalcriteria,inwhichapositivepathergytestscores1.Acaseseries with26suspectedpatientsispresented,andtheskinpathergytestwasperformedin23. Theresultswerereadin48hours,andtheywereconsiderednegativewhenwithoutpapule, andpositivewithapapuleor pustule.Positiveresultsweredividedbypapulesize,and dermatoscopywasdonetomeasureandobserveitsclinicalaspects.Afterthereadings,a biopsywasperformed,withannotationofhistopathologicalaspects.Thetestwasnegative in2(8.7%)andpositivein21(91.3%)patients.Theresultsandtheliteraturerevieware presented.
©2014ElsevierEditoraLtda.Allrightsreserved.
Dermatoscopia
no
teste
cutâneo
da
patergia:
série
de
casos
de
pacientes
com
suspeita
de
Doenc¸a
de
Behc¸et
Palavras-chave:
Doenc¸adeBehc¸et Técnicaseprocedimentos diagnósticos
Vasculite
r
e
s
u
m
o
Adoenc¸adeBehc¸etéumadoenc¸amultissistêmicaqueconsistedediferentescombinac¸ões de manifestac¸ões oculares, mucocutâneas, neurológicas, cardiovasculares, gastrintesti-naiseoutras. Seudiagnóstico sefundamentaem critérios clínicos,em queoteste da patergiapositivorecebeumponto. Apresenta-seumasérie decasos com26pacientes suspeitos,tendootesteda patergia da pelesidorealizadoem 23 deles.Os resultados foramavaliadosem48horas,tendosidoconsideradoscomonegativosdianteda ausên-ciadepápulaepositivosnapresenc¸adepápulaoupústula.Osresultadospositivosforam divididospelo tamanhodapápula,efetuou-seumadermatoscopiaparamedire obser-varseusaspectosclínicos.Apósasleituras,foirealizadaumabiópsia,comanotac¸ãodos
DOIoforiginalarticle:http://dx.doi.org/10.1016/j.rbr.2014.06.003. ∗ Correspondingauthor.
E-mail:[email protected](V.B.Rocha).
http://dx.doi.org/10.1016/j.rbre.2014.06.005
aspectoshistopatológicos.Otestefoinegativoem2(8,7%)epositivoem21(91,3%)pacientes. Apresentam-seosresultadosearevisãodaliteratura.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Behc¸et’sdisease(BD)isclassifiedamongvasculitides.1Itwas firstdefinedasatriadofrecurrentaphtousstomatitis, geni-talaphtaeandrelapsinguveitisin1937byHulusiBehc¸et.It isconsideredamultisystemicdiseaseconsistingofvarying combinationofocular,mucocutaneous,neurologic, cardiovas-cular,gastrointestinalandothermanifestations.2–7
Itsdiagnosisisbasedonclinicalcriteria.TheNew Interna-tionalCriteriaforBehc¸et’sDiseaseareoneofthemostrecently reviseddiagnosticcriteria.AdiagnosisofBDconsistsofasum ofthreeormorepointsaccordingtoascoresystem.Positive pathergytestscores1point(Table1).8
Pathergyisa hyperreactivity oftheskin afteraneedle trauma. It was first described in 1937 and it is consid-eredpathognomonic,althoughit can beseeninpyoderma gangrenosum,erythemaelevatumdiutinumandother neu-trophilicdermatoses,includingSweetsyndromeandtheblind loopsyndrome.9Itisreportedthatabout8%ofinflammatory boweldiseasepatientsshowthisphenomenon.10
Inspiteofitshighspecificity,theskinpathergyresponse hasvariablesensitivityandinconstantreproducibility,which limititsuse.Regardlessofthis,itisusedinmanysetsof clas-sification/diagnosiscriteria.1,9,11,12
Methods
Acaseseriesstudywasdonewithtwenty-sixsuspectedBD patients(23womenandthreemen)referredtoaprivateclinic tobetestedforpathergyphenomenon.
Outof26patients,thepathergytestwasperformedin23 patients,asthreeofthem(twomenandonewoman),which alreadyfulfilledthediagnosisofBDdidnotagreetobetested. Eightpatientsdid notpresent diseaseactivity (presence of
Table1–RevisedinternationalcriteriaforBehc¸et’s disease.
Criterion Score
(point)
Oralaphtosis 1
Skinmanifestations(erythema nodosum-likelesions,papulopustular lesionsorpseudofoliculitis,acneiform nodules)
1
Vascularlesions(arterialandvenous thrombosis,aneurysm)
1
Pathergyphenomenon(test) 1
Genitalaphtosis 2
Ocularlesions 2
Behc¸et’sDisease,threeormorepoints.
symptoms or signs)duringthe test, contrastingto 15who did.Fivepatientswereintreatment(takinglessthan20mg ofprednisone)whenitwasperformed.
Sixneedlepricksusing21gaugedisposableneedleswere doneintradermallyatthesamepointontheskinofthe fore-arm,aftercleaningthesitewith70%ethanolswabs.Results werereadbythesameobserver48hourslater.
Theywereconsiderednegativeifwithoutpapuleandonly needlemarkorerythemaandpositiveifwithpapuleor pus-tulesurroundedbyanerythema.Dermatoscopywasdoneto measurethereactionandobserveitsclinicalaspects.
After the readings abiopsy was performedand stained withhematoxylinandeosin(HE).Insomecasesmorethan1 pointofmultiplepunctureswereperformed(twopricktests) tochoosethebiggestpapuletobiopsy.
Results
Among the patients, 23 were women and 3 men.The age rangedfrom 11to72 yearsand theaverageagewas 33.11, withstandarddeviation14.73.
Theorallesionswere presentinall patients(100%), fol-lowedbygenitallesions,observedin12(46.1%),ocularlesions in10(38,5%),skinlesionsin10(38.5%),andjointand neuro-logicalinvolvementin13 (50%)and two(7.7%),respectively
(Table2).
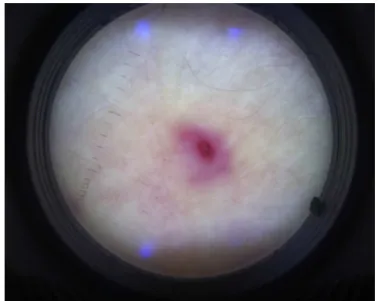
ThepathergytestwasnegativeintwoBDpatients(8.7%) and positive in 21 (91.3%). Among the positive tests, four (17.4%)werelessthan1mm,16(69.5%)werebetween1-2mm andone(4.3%)morethan2mm.Theseresultswerenot cor-relatedwiththediseaseactivityortreatment.Dermatoscopy showedneedlemarksandmilderythemainthenegativetests (2patients)anderythematouspapule/pustuleor exulcerocros-touslesionssurroundedbyerythematousand/oredematous areainthepositives(21patients)(Table3).Itwasagoodtool especiallytomeasureandexaminetheinflammatoryaspects ofthesmalllesions(lessthan2mm).Figure1showsthe der-matoscopicaspectofapathergytest.
The main histopathologic findings of the 23 biopsed patients were: perivascular inflammatory infiltration in 19
Table2–Clinicalmanifestationsin26patientswith suspectedBD.
Clinicalmanifestation Absolute
number(%)
oral 26(100)
genital 12(46)
ocular 10(38)
cutaneous 12(46)
arthritis 13(50)
T able 3 – V ar iants anal ysed in the SPT performed in 23 pa tients: size, derma toscop y , histopa thology , pr esence of tr ea tment at the moment of the test. P ather gy Histopatholo gy T reatment at the test Ne g ati v e P ositi v e -P apule size Dermatoscop y Nd mark <1mm 1-2mm >2mm P ap/pus P ap/crust Nd mark P eri v asc inf F ibrina Er ytr e xtr Interst inf Others W ith W ithout 2 4 16 1 15 6 2 19 16 13 10 43 5 18 P ap/pust, papule/pustule; P ap/crust, papule crust; Nd mark, needle mark; P eri v asc inf, peri v ascular inflammator y infiltr ation; F ibrina: de position of fibrinoid material; Er ytr e xtr , e xtr a v asation of er ythr oc ytes; Interst inf, intersticial inflammator y infiltr ation. Pr esence of neutr ophils or eosinophils, micr oa bscesses, leucoc ytoclasis, edema, necr osis,n uclear de bris, v asculitis and dama g e of v essels.
Figure1–Thedermatoscopicaspectofapathergytest.
(82.6%),depositionoffibrinoidmaterialin16(69.5%), extrava-sationoferytrocytesin13(56.5%),intersticialinflammatory infiltration in 10 (43.5%). Other detected alterations were: presenceofneutrophilsoreosinophils,micorabscesses, leu-cocytoclasis,edema,necrosis,nucleardebris,vasculitis and damageofvesselwalls(Table3).
After testing, the final diagnosis was: 20 patients (77%) fulfilled theInternational StudyGroup(ISG) criteriaforthe diagnosisofBD(Table1),and6(23%),whodidnot,were clas-sifiedashavingsuspectedBD.
Discussion
PositivepathergyisamongstthecriteriaforadiagnosisofBD. Therefore,thestudyofthisphenomenonisimportantnotonly tomakethediagnosisbutalsotounderstandthedisease.
thesetsofcriteriashowalossofaccuracy,demonstratingthat thisparameterisnecessarytoimprovethepowerofexisting classification/diagnosiscriteria.12
Themechanismsunderlyingpathergyareunknown.The skininjurycausedbytheneedle prickinthepatient’s skin apparentlytriggersacutaneousinflammatoryresponsewhich ismoreprominentand extensivethan thatseeninnormal skin.Itissuggestedthatanincreasedandaberrantreleaseof cytokinesfromkeratinocytesorothercellsintheepidermisor dermisresultsinaperivascularinfiltrationobservedonskin biopsy.8
Pathergyphenomenon was detectedmorefrequently in HLA-B51patientsespeciallyinsomecountries.1,8
Theforearmisthemostfrequentlypositivesiteanditis oftenchosentoperformthetest.6,8,9,12
Studies have demonstrated that the use of a blunt, re-usable,sterilizedneedleincreasesthefrequencyand inten-sityofSPT.Theintroductionofdisposableneedlescausedits decrease.Pathergyisfurtherrelatedtothediameterofthe needle.A20-gaugedisposableneedlegaveapositiveSPTin 62.5%buttheresultfellto35.8%when26-gaugeneedleswere used.Otherauthorsrecommendthetestwitha25or21-gauge needleinsertedintradermally,perpendicularordiagonallyto theskin.1,6,8,9,12–14
Therefore,theintensityofthereactionwasmore promi-nent with thicker needles (20-gauge). The intracutaneous physiologicalinjections,amethodusedbysomeinvestigators, wastheleastsensitive.8
There isno consensusabout the number ofthe needle pricksrequired.Somestudiesusedmultiplepricks,whichis consideredimportanttoincreasethepositiverateofaSPTand others,oneortwo.1,3,8,9,13,14
Mostinvestigators haveread 24-48hafter the test, and itisconsideredpositiveif anerythematouspapule >2mm indiameteror apustuleisobserved. Othershavereported positiveresultsin thepresenceofa papuleor pustule not mentioningitssize.Therefore,thepercentageofpositivetests differsfromonereporttoanothernotonlybecauseofethnic factorsbutalsoforthisreason.1,3,5,6,8,9,13,14
Inordertoinvestigatethereactions,theSPTresultswere dividedbasedonthesizeofthepapuleandabiopsywastaken evenifthepapulewassmallerthan2mm.
Thehigherfrequencywasfoundbetween1-2mm,andthe testsbiggerthan2mmweredetectedinalowfrequency(4.3%). Ontheotherhand,thehistologicexamsshowedprominent aspectsevenwhenthesizesweresmallerthan1mmandfor thatreasonalltheresultswiththepresenceofapapulewere consideredpositive.InastudyreportedinBrazil,91.6%of24 patientshadSPTnegative,butthehistopathologyonthesite ofthepathergytestshowedinflammatoryaspectsin83.3%of them.13
Althoughsomeauthorsdonotrecommendthebiopsyof the SPT, we performed the histopathologic exam because, accordingtoourresults,itconfirmedtheinflammatory pro-cessshowingimportantfindingstocomplementthetest.8,13
The pathergy phenomenon is not constant during the course of the disease. The degree of positivity may occa-sionallycorrelate with disease activity.1,2,12 Reportsdo not confirmtherelationbetweenpathergyandclinic manifesta-tions,beingnecessarylongitudinalstudiestoestablishit.2,12
There are apparent controversiesabout the histopatho-logicfindingsoftheSPT,sinceitsmethodologyisvariableand evaluatedafterdifferenttimeperiods.Inadditiontothis,a studycomparedhistopathologicandclinicalevaluationsand concluded that histopathologic investigation was no more sensitivethanclinicalobservation,butinthisseriesthetest wasconsideredpositiveif>2mm.2,8,13
In our series avariety of histopathologic findings were describedbut perivascularinfiltrationanddepositionof fib-rinoid material were the most frequent, confirming the literature.
Theexpressionpatternofadhesionmoleculesinpathergy reactionsuggestedadirectepidermalinjuryasthecauseofthe cutaneous inflammation. An intense antigen-independent induction phase of cutaneous inflammation might be developedbyincreasingthereleaseofcytoquinesfrom kera-tinocytes, which might later be amplified bythe effect of infiltratingactivatedmononuclearcells.
Inaddition,theimmunohistologicpictureofthepathergy reactionsuggestedacell-mediatedimmuneresponse.
Ethnicfactorsandthecross-sectionalmethodologyofthe variousstudiesperformedinseveralcountriesmayalso influ-encethereportedhistopathologicfindings.2,8,13
Sometimes,the cutaneousinflammationduetothe epi-dermal injury caused by the pricking is so light that the SPTisconsiderednegative.However,whenthereactionsare better observed byboth dermatoscopy and histopathology, and, consequently, eventhe tiny onesare considered pos-itive, as described in our report, the frequencyof positive SPTincreases. Therefore, thishigh frequencywasdetected becauseofthemethodologyappliedwhichvaluedthesizeand histopathologicfindingsofthereactions.
DespitethecontroversiesinthemethodologyoftheSPT,it isnecessarytoestablishguidelinestoperformit,sinceitisan importantkeyforthediagnosisoftheBD.
ReportsusingdermatoscopyintheSPTwerenotfound. Inconclusion,thedermatoscopyandhistopathologicstudy on the site ofthe punctures, performed48hoursafter the prickingtest,arestronglyrecommendedfortheinvestigation ofsuspectedBDpatients,sincetheycanreveal evidenceof inflammationeveninthesmalllesions.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.DavatchiF,ShahramF,Chams-DavatchiC,ShamsH,NadjiA,
AkhlaghiM,etal.Behc¸et’sdisease:fromeasttowest.Clin
Rheumatol.2010;29:823–33.
2.LeeS,BangD,LeeES,SohnS.Behc¸et’sDisease:Aguidetoits
ClinicalUnderstandingtextbookandatlas.Berlin:
Springer-Verlag;2001.
3.OzdemirM,BodurS,EnginB,BaysalI.Evaluationof
applicationofmultipleneedlepricksonthepathergy
4. VaiopoulosG,KonstantopoulouP,EvangelatosN,Kaklamanis
Ph.Thespectrumofmucocutaneousmanifestationsin
Adamantiades-Behc¸et’sdiseaseinGreece.JEurAcad
DermatolVenereol.2010;24:434–8.
5. GulU,GonulM.OralandgenitalpathergyinBehc¸et’sDisease.
Dermatology.2007;215:80–1.
6. OzdemirM,BaleviS,DenizF,MevlitogluI.Pathergyreaction
indifferentbodyareasinBehc¸et’sdisease.ClinExpDermatol.
2006;32:85–7.
7. Yalc¸indagNF,BatiogluF.Pathergy-likereactionfollowing
intravitrealtriamcinoloneacetonideinjectioninapatient
withBehc¸et’sDisease.OculImmunolInflamm.2008;16:
181–3.
8. VarolA,SeifertO,AndersonCD.Theskinpathergytest:
innatelyuseful?ArchDermatolRes.2010;302:155–68.
9. DavatchiF,Chams-DavatchiC,GodhsiZ,ShahramF,NadjiA,
HormozS,etal.DiagnosticvalueofpathergytestinBehc¸et’s
diseaseaccordingtothechangeofincidenceoverthetime.
ClinRheumatol.2011;30:1151–5.
10.HatemiH,HatemiG,CelikAF,MelikogluM,ArzuhalN,MatC,
etal.Frequencyofpathergyphenomenonandotherfeatures
ofBehc¸et’ssyndromeamongpatientswithinflammatory
boweldisease.ClinExpRheumatol.2008;26Suppl50:S91–5.
11.MenashiS,TriboutB,DosquetC,ToumelinPl,PietteJC,
WechslerB,etal.Strongassociationbetweenplasma
trombomodulinandpathergytestinBehc¸etdisease.Ann
RheumDis.2008;67:892–3.
12.DavatchiF,AbdollahibBS,DavatchiCC,ShahramF,GhodsiZ,
NadjiA,etal.Impactofthepathergytestontheperformance
ofclassification/diagnosiscriteriaforBehc¸et’sdisease.Mod
Rheumatol.2013;23:125–32.
13.ScherrerMAR,VitralN,BambirraE,OreficeF.Estudoclínicoe
histopatológicodapatergianaDoenc¸adeBehc¸et.AnnBras
Dermatol.1994;69:267–71.
14.OzdenMG,BekY,AydinF,SenturkN,CanturkT,TuranliAY.
Differentapplicationtechniquesofpathergytestingamong
dermatologists.JEurAcadDermatolVenereol.