w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Profile
of
ostomy
patients
residing
in
Pouso
Alegre
city
Geraldo
Magela
Salomé
∗,
Maiume
Roana
Ferreira
Carvalho,
Marcelo
Renato
Massahud
Junior,
Bruno
Mendes
UniversidadedoValedoSapucaí(UNIVÁS),PousoAlegre,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received6January2015 Accepted20February2015 Availableonline8April2015
Keywords: Stoma Colostomy Nursingcare
a
b
s
t
r
a
c
t
TheobjectivewastocharacterizetheclienteleofostomypatientslivinginPousoAlegre, MinasGerais,Brazil.Amongthecausesthatledpatientstoacquireanostomy,themost prevalentwasneoplasia;thetypeofostomywasapermanentcolostomy.Mostpeoplewere nottoldthattheywouldbesubmittedtothestoma.Inaddition,individualswerenotsubject tostomademarcation,andirrigationwasnotperformed.Regardingthetypeofcomplication, 34(48.60%)haddermatitis;14(20%),retraction;and13(18.60%),prolapse.Withrespectto stomadiameter,34(48.60%)had20–40mmand23(32.90%),40–60mm.Withthisstudy,we becameawareoftheprofileofostomizedpatientstreated atthemunicipalityofPouso Alegre/MG;itisexpectedthat,withthesedata,theimprovementofcaretothispopulation canbesubsidized.Wesuggestthatnursingprofessionalsthinkofhealthactionstrategies withrespecttoguidanceonstomamanufactureandtomeasuresaimingfortheprevention ofpossiblecomplications,promotingwaystohelpthesepatientstomakedecisionsandto verbalizefeelings,sothattheyfeelsupportedincopingwithchangesintheirbodyimage, forthesakeofsurvival.
©2015SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All rightsreserved.
Perfil
dos
pacientes
estomizados
residentes
no
município
de
Pouso
Alegre
Palavras-chave: Estoma Colostomia
Cuidadodeenfermagem
r
e
s
u
m
o
OobjetivofoicaracterizaraclienteladeestomizadosresidentesemPousoAlegre,Minas Gerais.maioriadascausasquelevaramospacientesaadquirirostomiafoineoplasia;otipo deostomiaeracolostomiaemdefinitivo.Amaioriadosindivíduosnãoforamcomunicados dequeseriamsubmetidosaoestoma.Alémdisso,osindivíduosnãoforamsubmetidosà demarcac¸ãodoestomaenãofoirealizadairrigac¸ão.Comrelac¸ãoaotipodecomplicac¸ão, 34(48,60%)apresentaramdermatite;14(20%),retrac¸ãoe13(18,60%),prolapso.Comrelac¸ão aodiâmetrodoestoma,34(48,60%)mensuravam20a40mme23(32,90%),40a60mm.Este estudopossibilitouconheceroperfildospacientesostomizadosatendidosdomunicípio
∗ Correspondingauthor.
E-mail:[email protected](G.M.Salomé).
http://dx.doi.org/10.1016/j.jcol.2015.02.002
dePousoAlegre/MGeespera-seque,comessesdados,sepossasubsidiaramelhoriada assistênciaaessaclientela.Sugere-seaquiaosenfermeirospensaremestratégiasdeac¸ões desaúdecomrelac¸ãoàsorientac¸õessobreaconfecc¸ãodoestoma,medidasdeprevenc¸ão depossíveiscomplicac¸ões,promovendomeiosparaauxiliaressespacientesatomarem decisões,verbalizaremsentimentos,demodoquesesintamapoiadosnoenfretamentodas mudanc¸asdasuaimagemcorporalemproldasobrevivência.
©2015SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda. Todososdireitosreservados.
Introduction
Anostomizedpersonisanindividualwhoissubjectedtoan operationwhichresults inthe productionofastoma. The termostomyorstomacomesfromtheGreekword“stoma” andmeansanopeningofanewmouthsurgicallyconstructed, aimingexternalizinganyexistinghollowviscerainthebody. Itisthereforeanartificialcommunicationbetweenorgansor viscera towardthe external environment. Withan ostomy, we seek the accomplishment of drainage, elimination, or nutrition.Thisstomacan stillbetemporaryor permanent, dependingon the cause andpurpose forwhichthe device wassurgicallyconstructed.Anintestinalstomaisindicated whensomebowelsegmentpresentsdysfunction,obstruction orinjury.Thestomaisnamedafterthebowelsegment,and maybeanileostomy,colostomyorcecostomy.1,2
Thecare of people with an intestinal stomashould be donethroughhumanizedcareandevaluationoftheirclinical conditions,throughphysicalexaminationandamedical his-tory,withappreciationofthepatient’sverbalandnonverbal reports.Thus,itisnecessarytosystematizethecaretothese ostomized individuals. This kind of care enables promot-ingpatientrehabilitationandminimizinghis/hersuffering, especiallybyencouraging self-care.Thus,it isnecessary to systematizeassistancetotheseostomizedindividuals.This assistanceenablespromotingpatientrehabilitationand min-imizinghis/hersuffering,especiallybyencouragingself-care. Thisstrategydoesnotallowthatbeliefsandtaboosbecome threatstotheirphysical, socialandpsychologicalintegrity. Thiscarealsoaimstosuppressthefearofperforming self-care.3–7
Whenaostomizedpatientreceivesinadequatecare,this maycausevariouscomplications,especiallyinthestomaand peristomalskin,e.g.,skinlesionsatvariouslevels,herniation, infection,stenosis,prolapse,andretraction,amongothers.6–8
Usually, complications withthe stomaare related to non-compliancewithimportanttechnicalprocedures,namely:a previousdemarcationofthesiteintheabdominalareawhere thestomawillbeexternalized,thesurgicaltechniqueforthe preparationoftheintestinallooptobeexternalized,early mat-uration,andtheuseofacollectordevicesuitableforthetype ofstomaselected.9
Complicationsrelatedtothestomaandthedifficultyofthe patienttoperformself-carearethemainfactorsinvolvedin his/herrehabilitation;thenursingcareshouldbehaveitsstart attheverytimeofdiagnosisandindicationofsurgery, seek-ingtominimizesufferingandgetabetteradaptationofthe patient.Thus,theemphasisonself-carehasbeendescribed
asanalternativetoenablethepatienttoactivelyparticipate inhis/herowncare,stimulatingtheresponsibilityforthe con-tinuityofcareafterthedischarge,whichwillcontributetothe rehabilitationprocess,minimizingoravoidingthe complica-tionsdescribedabove.10
Giventhefewpublishedstudiesonpatientsseenandthe knowledgegapontherealneedsoftheseostomizedpeople, weset ourselvestodevelopthisstudy.Webelievethatour resultsmayprovidesupportforcaresystematizationandfor thedevelopmentofcareprotocolsthataimtoanearly reha-bilitationofthispopulation.Ouraimwastocharacterizethe populationofostomizedpeoplelivinginPousoAlegre,Minas Gerais,Brazil.
Method
Thisisadescriptivestudyonintestinalstomapatientsliving inPousoAlegre,MinasGerais,andregisteredinthePrograma deAtenc¸ãoàPessoaOstomizadainPousoAlegre.Datawere col-lectedbetweenDecember2012andMay2013,afterapproval bytheResearchEthicsCommitteeoftheUniversidadedoVale doSapucaí(opinionNo.23,277).Thesampleconsistedof70 participants,selectednon-probabilisticallybyconvenience.
Allostomizedpatientsagreedtoparticipateinthisstudy and signeda freeand informed consent. Participants had assuranceoffullexemptionofrisksandofanonymity.
Ourinclusioncriteriawere:thesubjectmustbean intesti-nalstomauser,andbeaware,alert,oriented,andagreeingto participateinthisstudy.Theexclusioncriteriawere:patients withurinaryorotherkindofstoma.Asemi-structured inter-viewwasconductedwiththeuseofaformcontainingopen questions.Thesequestionsweredividedinto:identification data,socio-demographicaspects,stomadescription, compli-cations,anddevicesinuse.
Dataweretabulatedandorganizedintographsandtables usingtheExcel2003program;thenadescriptiveanalysiswas performed.Thechi-squaredtestwasalsoused.The signifi-cancelevelforstatisticaltestswas5%(p≤0.05).
Results
InTable1,itwasfoundthatmostparticipantsstoodintheage
groupover60,weremale,retired,andattendingtoasupport group.Twenty-one(30%)ofourparticipantswereilliterateand 19(25.10%)couldreadandwrite.
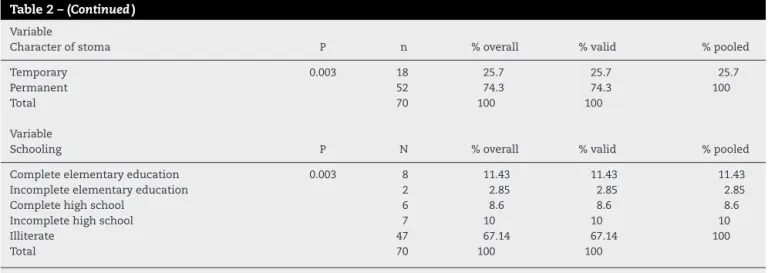
Table 2describesthat cancerwas the leadingcause for
Table1–Socio-demographiccharacteristicsofindividualswithintestinalstoma.
Gender P N %overall %valid %pooled
Male 0.003 52 74.3 74.3 100
Female 18 25.7 25.7 25.7
Total 70 100 100
Variable
Agegroups P n %overall %valid %pooled
44–59years 0.057 17 24.3 24.3 24.3
60–67years 18 25.7 25.7 50
68–74years 16 22.9 22.9 72.9
75–85years 19 27.1 27.1 100
Total 70 100 100
Variable
Maritalstatus P N %overall %valid %pooled
Married 0.035 34 48.6 48.6 48.6
Separated 14 20 20 68.6
Widow(er) 22 31.4 31.4 100
Total 70 100 100
Variable
Occupation p N %overall %valid %pooled
Retired 0.003 50 71.4 73.5 73.5
Unemployed 4 5.7 5.9 79.4
Working 14 20 20.6 100
Total 68 97.7 100
Noresponse 2 2.9
Total 70 100
Variable Support
group/association
p N %overall %valid %pooled
Yes 0.075 38 54.3 54.3 54.3
No 32 45.7 45.7 100
Total 70 100 100
Total 70 100 100
Chi-squaredtest(p≤0.05).
permanent colostomy type. Most of the participants had
not been told that they would receive the stoma.
More-over,nostomademarcationhad beenmade,andnostoma
irrigationwasperformed.Regardingthetypeofcomplication, 34(48.60%)patientshaddermatitis;14(20%),retraction;and13 (18.60%),prolapse.Withrespecttostomadiameter,34(48.60%)
hada20–40mmstoma,and23(32.90%)a40–60mmstoma.
Discussion
Theincreaseinlifeexpectancy,theindustrializationprocess andtheeffectsofurbanizationresultedinmoreexpositionof theBrazilianpopulationtonumerousdiseases,amongwhich standoutthecancer,traumaandchronicdegenerative dis-eases.Thus,inmanycircumstancestheuseoftechnological resources,suchasimplantprostheticsandorthotics,is criti-calinordertosavelivesortoallowabetterqualityoflife.10
Technologicalprogressandtheimprovementofsurgical tech-niquescontributedstronglyfortheearlydiagnosisofdiseases inholloworgansthatrequireexternalizationtoperformtheir
functions,thereforeimprovingthequalityoflifeandthe reha-bilitativeprocess.11
Ourresultsshowedthat,ofthe70ostomizedpatients,52 (74.30%)weremale.Theseresultscoincidewithsomesimilar findingsfoundbypreviousstudies.12–16
As for marital status, the study showed that married patients prevailed, i.e. 34 (48.60%), followed by22 (31.40%) widowedand14(20.00%)separatedsubjects.Thisresult high-lightstheimportanceoffamilyinvolvement,especiallyofthe spouse,intherecoveryoftheostomizedpatient.
Itshouldbeborneinmindthatthegenderofanostomized subjectmayinfluenceitssocialadaptation.Womentendto requirelesstimeforrehabilitation,althoughdemonstrating significantdegreesofdespair,depressionandfearinthe pre-operativeperiod.On theother hand,men,especiallythose who developimpotence,takealonger timetorespond sat-isfactorily to routine activities, including presenting more pronounceddifficultiesforself-care.17
Table2–Distributionofindividualsaccordingtobowelstomacharacteristics.
Variable Causeofostomy
P N %overall %valid %pooled
Diverticulitis 0.003 3 4.3 4.3 4.3
Inflammatoryboweldisease 5 7.1 7.1 11.4
Neoplasia 52 74.3 74.3 85.7
Crohn’sdisease 10 14.3 14.3 100
Total 70 100 100
Variable
Stomatype P N %overall %valid %pooled
Colostomy 0.007 54 77.1 77.1 77.1
Ileostomy 16 22.9 22.9 100
Total 70 100 100
Variable
Stomadiameter P N %overall %valid %pooled
0–20mm 0.056 10 14.3 14.3 14.3
20–40mm 34 48.6 48.6 62.9
40–60mm 23 32.9 32.9 95.7
60–80mm 3 4.3 4.3 100
Total 70 100 100
Variable
Typeofcomplication P N %overall %valid %pooled
Dermatitis 0.0023 34 48.6 48.6 48.6
Fistula 1 1.4 1.4 50
Peristomalhernia 5 7.1 7.1 57.1
Pseudo-verrucouslesion 1 1.4 1.4 58.6
Allergicreactiontodevice 1 1.4 1.4 60
Pseudo-verrucouslesion/dermatitis 1 1.4 1.4 61.4
Retraction 14 20 20 81.4
Prolapse 13 18.6 18.6 100
Total 70 100 100
Variable
Ademarcationwasperformed? P N %overall %valid %pooled
Yes 0.002 17 24.3 24.3 24.3
No 53 75.7 75.7 100
Total 70 100 100
Variable
Typeofdevice P n %overall %valid %pooled
Singlesystem 0.043 22 31.4 31.4 31.4
Two-partsystem 48 68.6 68.6 100
Total 70 100 100
Variable
Irrigationwasperformed? P n %overall %valid %pooled
Yes 0.047 26 37.1 37.1 37.1
No 44 62.9 62.9 100
Total 70 100 100
Variable
Youweretoldthatyouwouldhaveastoma? P n %overall %valid %pooled
Yes 0.049 48 68.6 68.6 68.6
No 22 31.4 31.4 100
Table2–(Continued)
Variable
Characterofstoma P n %overall %valid %pooled
Temporary 0.003 18 25.7 25.7 25.7
Permanent 52 74.3 74.3 100
Total 70 100 100
Variable
Schooling P N %overall %valid %pooled
Completeelementaryeducation 0.003 8 11.43 11.43 11.43
Incompleteelementaryeducation 2 2.85 2.85 2.85
Completehighschool 6 8.6 8.6 8.6
Incompletehighschool 7 10 10 10
Illiterate 47 67.14 67.14 100
Total 70 100 100
Chi-squaredtest(p≤0.05).
modifiedbodyimage,andfinditdifficulttoengagein extra-marital relationships after surgery, adding that only their spousesacceptphysicalcontact.Thesedataagreewithastudy thatstudiedaffectedsexualityinpatientswitharecentstoma, whenwithoutapermanentsexualpartner,becausetheyfeel insecure,ashamed,andafraidofnotbeingacceptedbythe partner.18–23Thissupportiscritical,becausewhenthepatient
is subjected to the construction of a stoma, soon restric-tionsariseabouthis/hersexuallife.Theostomizedindividual beginstoseetheostomyasananatomicalmutilation.Thus, thefamilyisnowessentialtotheimplementationofa thera-peutic,rehabilitativeandsocialreintegrationplan.
As to age group, the population over 60 years was the mostaffected.Inthisfinding,isimportanttoemphasizethat the elderly have unique biological characteristics and are morevulnerableto chronicdegenerative diseases,i.e. neo-plasms.MeirellesandFerraz13 claimthattheoccurrenceof
complicationsinthestomaismultifactorial,involvingstoma constructionand itslocationand alsothe patient’sobesity, withinfluenceoftheagefactor.Thus,whenthesefactorsare consideredtogetherwithphysiologicalchangesofaging,the resultisagreatervulnerabilityoftheelderlyintheincidence ofstomacomplications.24
Regardingthelevelofeducation,itwasnotedthatmost, i.e.47(67.14%) patients,wereilliterate. Thisfindingreveals aworryingprofile,whenthinkingintermsofcitizenshipand respectforindividualrights,becauseitisknownthatthelower the educational level, the more unfavorable is the linguis-ticcapitalofthesubjects,sothattheycanaskprofessionals abouttheirhealthproblems,thecarethatshouldbecarried outandalsoabouttheirinherentrightsascitizens.Itisworth mentioningthatthisdoesnotinterferewiththecareofthese people, because the interaction between user, service and healthprofessionalhasmanagedtoovercomethedifficulties posedbythisvariable.25
Analyzing the participants’ occupation, it was observed that“retiree”was theprofessional statusthatstood out in this study group: 50 (71.40%), followed by “actively work-ing”,14(20.00%).These findingsare inlinewithdatafrom otherstudies.1,2,6,8,11,13,15Oneofthesocialconsequencesfor
ostomizedpatientsisachangeintheirroleandsocialstatus,
bothintheirfamilyandinsociety.Aftersurgery,itiscommon fortheostomizedpatient(thatwasworking)achangefora retiredstatus.Thus,theostomizedindividualisnolongerthe family provider,thusbecoming dependentonitforhis/her care.9
In this study, the investigators reported that the exter-nalized intestinal segments were colostomies and that, as toloopexternalizationtime,theostomiesweredefinitive.In 52patients(74.30%),thecausesformakingthestomawere attributed tocancer; and moststomata had a diameterof 20–40mm;thesefindingsare consistentwithotherstudies’ findings.3,8–13,26–28
Itisworthnotingthatthepermanencytimewiththestoma dependsonthecausalfactorandoftheclinicaloutcomeafter itsmaking.Thus,aninitiallytemporarystomamaybecome permanent,dependingonthedrawbackstointestinaltransit restoration,becauseinmanycasesthegastrointestinaltract diseasesleadtoaradicalsurgery,resultinginatemporary,or evenpermanent,ostomy15Regardingthetypeofsystem,48
(68.60%)ofthepatientsusedtwo-piecedevices,whilein44 (62.90%)irrigationwasnotperformed.
Itisworth notingthat whenpatientswere asked about demarcation implementation preoperatively, mostof them reportedthatthisprocedurehadnotbeendone.Demarcation isextremelyimportant,giventhataconvenientlocation facili-tatesself-careandtherehabilitativeprocess.Therefore,when performingthephysicalexamination,thehealthprofessional mustbeawareofthestomapositioningsite,andthe demar-cationofthestomashouldbemadepreoperatively,inorder topreventorminimizepossiblecomplicationsinthestoma andperistomalregion.Itisalsocriticalthat,atthattime,the nursegiveguidancebothtothepatientandtohis/herfamily aboutself-care.3,8,9
self-care,duetolackofproperguidanceand/orassistanceof askilledprofessionalduringthisphaseoftreatment.10
Regarding complications, 36 (48.60%) patients had der-matitis; 14 (20.00%), retraction; and 13 (18.60%) prolapse. Inaddition, 48 (68.60%) patients were not toldthey would receive anintestinal stoma.Oneshould alsoconsider that theincidenceofsomecomplicationsincreaseswithageand inpatientswithoutstomademarcation.Consideringthatthe demarcationwasnotperformedinthisstudypopulation (pre-dominantlymadeupofolderpeople),itcanbesaidthatthis factrepresentedoneofthefactorsthatmayhavecontributed totheoccurrenceofcomplicationssuchasthosecited,thus confirmingthefindingsinotherstudies.
Usually,dermatitidesarelesionsduetoaninappropriate useofcollectordevices,morepreciselybyanexcessive cut-tingoftheholeoftheprotectivebarrier,relativetothestoma (thiserrorleavestheskinexposedtotheeffluentaction),or byaninadequateindicationoftheequipmenttothetypeof stoma.Collectorsand adjuvantequipmentavailableonthe marketmustbepresentedintheminutestdetailtoostomized patients. The equipment used in some services is recom-mendedasaresultoftheevaluationmadeatthetime;but, overtime,theequipmentmaybereplaced–hencetheneed foracontinuousassessment.1,29
Regardingintestinalprolapse,itsoccurrenceisshownin isolationinonecase,withaddedcomplicationsintwocases. Theostomizedpatientwhopresentedassolecomplicationthe prolapse(afemale)hadhersurgeryonanemergencybasis, andpresentedthiscomplicationearly.Inthispatient,the fac-torsofageandstomainsertionsitedidnotcontributetothe problem,giventhatshewas notanelderlyperson andthe locationofthestomawasadequate.Thus,thereisa possibil-ityofsurgicaltechniquefailureduringthestomaconstruction, asinmanycasestheincidenceofprolapseisassociatedwith technicaldetailsused.8,14,17,23,24,27,28,30
Ontheotherhand,thesimultaneouspresenceofprolapse anddermatitishastodowiththeoccurrenceofthefirst com-plicationduetothe second one,that is,depending onthe degreeofexternalizationoftheintestinalloop,thesegment maybeexposingtheskintopatient’seffluentsandtoan exces-sivemucosalsecretion,thusreducingthepooradherenceof thebagandfavoringfecalleakage.23,24,27,28,30
Asforthecasewithstomaretraction,duringtheinterview andphysicalexaminationitwasrealizedthatthispatientwas anelderly,obesewoman,andherstomawaspoorlylocated. Therefore,thesethreefactorsdeterminedtheoccurrenceof animmediateretraction,whichischaracterizedbydiscomfort anddifficultyofadaptationtotheequipment–inshort, com-promisingself-careandtherehabilitativeprocess.8,14,17,23,28–30
Althoughinmostcasesthemakingofanostomyaimsto savelives,theprocedureinvolvesnumerousandvaried adap-tationsthat imposeadditional problemsforthe ostomized patient.Thesedifficultiesrelatetotheacceptanceofchanges inbodyimage,lifestyle,socialrelationshipsandsexuality per-formance,allofwhichcangeneratesocialandpsychological disorders,oftendifficulttoovercome.10
Therefore,inview ofthemany aspectsthat involvethe rehabilitationoftheostomized individual,the nursingcare for this kind of client should have its start at the very momentofdiagnosisandindicationofsurgery.Thus,themain
objectiveistominimizesufferingandgetabetteradaptation. Theemphasisonself-carehasbeendescribedasan alterna-tivetoenablethepatienttoactivelyparticipateinhis/herown care,stimulatingtheresponsibilityforthecontinuityofcare.10
Thisstudyshowstheimportanceofusingaclear, acces-sible and objective language by all professionals (nurses, doctors,psychologists)involvedinthecareofostomypatients, forabetterunderstandingbytheclient,consideringthata good nursingcareshould begininthe preoperativeperiod, withevaluations,guidanceandcareintheneededpreparation tofacethesurgery.Andthispreparationshouldbe continu-ousthroughouttheperiodduringwhichthepatientremains withtheostomy–andperhapsthismeanspermanently.The ostomizedpatientshouldbewellguided,taughtandtrained for the skills needed totake careof himself/herself, espe-ciallywhenitcomestohandlingthestoma,suchascleaning theperistomalskin,specificationsandavailabilityofspecific equipmentandadjuvantmeansforeffluentcollection.31
Conclusion
Withthisstudy,webecameawareoftheprofileofostomized patients treated in Pouso Alegre/MG; with these data it is expectedthattheimprovementofcaretothispopulationcan besubsidized.Wesuggest that nursingprofessionalsthink about health strategieswithrespectto guidance onstoma manufactureandmeasuresaimingforthepreventionof pos-siblecomplications,promotingwaystohelpthesepatientsto makedecisionsand toverbalizetheirfeelings,sothatthey feelsupportedincopingwithchangesintheirbodyimage,for thesakeofsurvival.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.FernandesRM,MiguirELB,DonosoTV.Perfildaclientela
estomizadaresidentenomunicípiodepontenova,minas
gerais.BrasColoproct.2011;30(4):385–92.
2.SantosCHM,BezerraMM,BezerraFMM,ParaguassuBR.Perfil
doPacienteOstomizadoeComplicac¸õesRelacionadasao
Estoma.BrasColoproct.2007;27(1):016–9.
3.SantosVLCG,CessarettiIUR.AssistênciaemEstomaterapia:
cuidandodoostomizado.SãoPaulo:Atheneu;2000.
4.TaylorC,LillisC,LeMoneP.FundamentosdeEnfermagem:a
arteeaciênciadocuidadodeenfermagem.5thed.Porto
Alegre:Artmed;2007.p.589–635.
5.GemelliLMG,ZagoMMF.Ainterpretac¸ãodocuidadocomo
ostomizadonavisãodoenfermeiro:umestudodecaso.
Latino-amEnfermagem.2002;10(1):34–40.
6.CostaVF,AlvesSG,EufrásioC,SaloméGM,FerreiraLM.Body
imageandsubjectivewell-beinginostomistsinBrazil.
GastrointestNurs.2014;12(5):37–47.
7.SaloméGM,AlmeidaSA.Associationofsociodemographic
andclinicalfactorswiththeself-imageandself-esteemof
individualswithintestinalstoma.JColoproctol.
2014;34(3):159–66.
8.AguiarESS,SantosAAR,SoaresMJGO,SilvaAncelmoMN,
PeriestomalcomPacientescomEstomasIntestinales.Rev
Estima.2011;9(2):22–30.
9. MoraesJT,VictorDR,AbdoJR,SantosMC,PerdigãoMM.
Characterizationofenterostomalpeopleassistedbythe
MunicipalGeneralOfficeofHealthofDivinópolis-MG.Rev
Estima.2009;7(3):31–7.
10.TosatoSR,ZimmermannMH.Conhecimentodoindivíduo
ostomizadoemrelac¸ãoaoautocuidado.ConexãoUEPG.
2006;1(1):33–7.
11.CesarettiIUR,SantodsVLCG,ViannaLAC.Qualidadedevida
depessoascolostomizadascomesemusodemétodosde
controleintestinal.RevBrasEenferm.2010;63(1):16–21.
12.ZimnickiKM.Preoperativestomasitemarkinginthegeneral
surgerypopulation.JWoundOstomyContNurs.
2013;40(5):501–5.
13.NakagawaH.Stomalocationrequiresspecialconsiderationin
selectedpatients.JWoundOstomyContNurs.
2013;40(6):565–6.
14.NakagawaH,MisaoH.Effectofstomalocationonthe
incidenceofsurgicalsiteinfectionsincolorectalsurgery
patients.JWoundOstomyContNurs.2013;40(3):287–96.
15.SallesVJA,BeckerCPP,FariaGMR.Theinfluenceoftimeon
thequalityoflifeofpatientswithintestinalstoma.J
Coloproctol.2014;34(2):73–5.
16.MelottiLF,BuenoIM,SilveiraGV,SilvaMEN,FedosseE.
Characterizationofpatientswithostomytreatedatapublic
municipalandregionalreferencecenter.JColoproctol.
2013;33(2):70–4.
17.MacedoMS,NogueiraLT,LuzMHBA.Perfildosestomizados
atendidosemhospitaldereferênciaemTeresina.Estima.
2005;3(4):25–8.
18.PereiraAP,CesarinoCB,MartinsMR,PintoMH,NetinhoJG.
Associationsamongsocio-demographicandclinicalfactors
andthequalityoflifeofostomizedpatients.RevLatAm
Enfermagem.2012;20(1):93–100.
19.PaulaMAB,TakahashiRF,PaulaPR.Ossignificadosda
sexualidadeparaapessoacomestomaintestinaldefinitivo.
BrasColo-proctol.2009;29(1):77–82.
20.BecharaRN,BecharaMS,BecharaCS,QueirozHC,OliveiraRB,
MotaRS,etal.Multidisciplinarystaffofthestomized.Bras
Colo-proctol.2005;25(2):146–9.
21.WongSK,YoungPY,WidderS,KhadarooRG.Adescriptive
surveystudyontheeffectofageonqualityoflifefollowing
stomasurgery.OstomyWoundManage.2013;59(12):16–23.
22.KnowlesSR,WilsonJ,WilkinsonAM.Psychologicalwell-being
andqualityoflifeinCrohn’sdiseasepatientswithanostomy:
apreliminaryinvestigation.JWoundOstomyContNurs.
2013;40(6):623–9.
23.SilvaAC,SilvaGNS,CunhaRR.Caracterizac¸ãodePessoas
EstomizadasatendidasemConsultadeEnfermagemdo
Servic¸odeEstomaterapiadoMunicípiodeBelém-PA.Estima.
2012;10(1):12–9.
24.ZilbersteinB,Gama-RodriguesJ,Habr-GamaA,SaadWA,
MachadoMCC,CecconelloI,etal.Cuidadosprée
pós-operatóriosemcirurgiadigestivaecoloproctológica.São
Paulo:Roca;2001.p.104.
25.MinistériodaSaúde(Brasil),SecretariadeAtenc¸ãoàSaúde.
Portarian◦400,de16denovembrode2009.Brasília(DF):
MinistériodaSaúde;2009.
26.OliveiraCAGS,RodriguesJC,SilvaKN.Identificac¸ãodonível
deconhecimentodepacientescomcolostomiasparaa
prevenc¸ãodepossíveiscomplicac¸ões.Estima.2007;5(4):
26–30.
27.ChilidaMSP,SantosAH,CalvoAMB,BelloBEC,AlvesDA,
GuerinoMI.Complicac¸õesmaisfrequentesempacientes
atendidosemumpolodeatendimentoaopacientecom
estomanointeriordoEstadodeSãoPaulo.Estima.
2007;5(4):31–6.
28.SonobeHM,BarichelloE,ZagoMMF.Avisãodo
colostomizadosobreousodabolsadecolostomia.Bras
CancerolRevBrasCancerol.2002;48(3):341–8.
29.SaloméGM,AlmeidaSA,SilveiraMM.Qualityoflifeand
self-esteemofpatientswithintestinalstoma.JColoproctol.
2014;34:231–9.
30.Habr-GamaA,AraújoSEA.EstomasIntestinais:aspectos
conceituaisetécnicos.In:SantosVLCG,CesarettiIUR,editors.
AssistênciaemEstomaterapia:cuidandodoostomizado.São
Paulo:Atheneu;2000.p.39–40.
31.LuzMHBA,AndradeDS,AmaralHO,BezerraSMG,Benício
CDAV,LealACA.Caracterizac¸ãodospacientessubmetidosa
estomasintestinaisemumhospitalpúblicodeTeresina-PI.