REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Efficiency
of
levobupivacaine
and
bupivacaine
for
supraclavicular
block:
a
randomized
double-blind
comparative
study
Cenk
Ilham,
Elif
Bombaci,
Serhan
Yurtlu
∗,
Serhan
C
¸olako˘
glu
Dr.LütfiKırdarResearchandEducationHospital,Istanbul,Turkey
Received16April2012;accepted20March2013 Availableonline23October2013
KEYWORDS
Supraclavicularblock; Bupivacaine;
Levobupivacaine
Abstract
Backgroundandobjectives: Success rate of catheter applications is low in supraclavicular block.Thus,bupivacaineandlevobupivacainebecomeimportantwiththeirlongeffecttimein singleinjectionpractices.Inthisstudy,weaimedtocomparetheeffectiveness,sideeffects andcomplicationsofbupivacaineandlevobupivacaineinsupraclavicularblock.
Methods:Sixtypatientsagedbetween20and65,withbodyweightbetween50and100kg,in theASAI-II-IIIgroupwhowerescheduledforhand,forearmandarmsurgeryusing supraclavicu-larblockwererandomizedintotwogroupsof30.Thepatientsreceived30ml0.5%bupivacaine (GroupB)or30ml0.5%levobupivacaine(GroupL).Motorandsensoryblockswereevaluated. Motor andsensory block onsettimes, total block durations, postoperative pain,amount of postoperativeanalgesicusedandpatientsatisfactionwererecorded.
Results:Demographicdata,distributionofsurgicalareaandhemodynamicdataweresimilar betweenthetwogroups.Surgery,motorandsensoryblockdurationsofGroupBandLpatients didnotvarystatisticallysignificantly.However,motorandsensoryblockonsettimesinGroup B were significantly shorter thanGroup L (p<0.05). The mean time for first postoperative analgesicdemandwere16.6±8.0hinGroupBand14.4±7.3hinGroupL(p>0.05).
Conclusion: 30ml0.5%bupivacaineandlevobupivacaineprovidesimilarblockcharacteristics forsupraclavicularblock.Bupivacaineleadstofastermotorandsensoryblockonsetcompared tolevobupivacainehoweversimilardurationofpostoperativeanalgesia.
© 2013SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
Introduction
Currently bupivacaine is one of the most commonly used
local anesthetic for central and peripheral nerve blocks.
∗Correspondingauthor.
E-mail:[email protected](S.Yurtlu).
However,ithasapotentialtocauseseriouscardiovascular sideeffectsandthe newlocalanestheticlevobupivacaine is reportedto be safer in this respect.1,2 The experience
withlevobupivacaine islimited in peripheral blockswhen comparedtobupivacaine.
Supraclavicularblockenablesacomplete anesthesiato thearm,elbowandhand.Postoperativeanalgesiarequires acatheterinsertion perineurally,however success rateof
0104-0014/$–seefrontmatter©2013SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
catheterapplicationsinsupraclavicularblockislowerthan otherbrachialplexusnerveblocksites.Ananotherwayof providingpostoperativeanalgesiaistouselocal anesthet-icswithlong duration of action. Long termpostoperative analgesiawithasingleapplicationispossiblewiththeuse of bupivacaine, levobupivacaine or ropivacaine. Thus we aimedtocomparebupivacainewithitsS(+)enantiomer, lev-obupivacaine in terms of their effectiveness, side effects andcomplicationsinsupraclavicularblock.
Methods
Priortothestudy,approvalofthehospitalethicscommittee (DrLütfiKırdarResearchandEducationEthicsCommittee, Date:29-03-2007,Number:3)hasbeenobtained.
Sixtypatientsagedbetween 20and65years,weighing between 50 and 100kg and at ASA I-II-III physical condi-tionwhowerescheduledforelectivehand,forearmorarm surgerywereincludedinthisstudy.Awritteninformed con-sentofparticipatingpatientswereobtained.
Exclusion criteria included being classified as ASA risk classificationof IV or above, analgesic drug intakein the last 24h, coagulation anormalities, having infection or previoussurgery inthe operative site,anatomic deforma-tions on block site, presence of neurological deficiencies on the operative extremity, uncooperable patients, suf-fering a peripheral nerve disorder, undergoing psychiatric treatment, alcohol and/or drug abuse, known allergy to studymedications,andhavingdiaphragm paralysisand/or pneumothorax on the contralateral side to be oper-ated.
Patients who participated in the study were randomly divided into two groups of 30 individuals in each with a computergenerated randomizationlist (Group B: 30ml 0.5%,5mg/mlbupivacaine; Group L:30ml 0.5%, 5mg/ml levobupivacaine).Patientsweretakentotheregional anes-thesia section within the operating theater 1h prior to surgery.Theywerelaidinsupinepositionontheblocktable. Baseline hemodynamic parameters [systolic arterial pres-sure(SAP),diastolicarterialpressure(DAP), meanarterial pressure (MAP), heart rate (HR), peripheral oxygen satu-rations (SpO2)] andelectrocardiograms were monitorized.
Allvaluesweremeasuredprior totheblockandrecorded as control values. Venous access was obtained by using a 20G branula and crystalloid infusion was initiated. As a premedication, 0.03mg/kg iv midazolam was adminis-tered.
Thepointwhereblockwouldbeadministeredwas iden-tifiedbyusingtheclassicaltechnique.3StimuplexHNS12®
(B. Braun, Melsungen, Germany) wasused as nerve stim-ulator and Stimuplex A® (B. Braun, Melsungen, Germany;
22G,50mm)wasusedasablockneedle.Afteradministering localanesthesiaatthemarkedpointofentry,ablock nee-dlewasusedtosearchformovementofmusclesinnervated by thenerves of the brachialplexus Two of these nerves (median, ulnar, radial or .musculocutaneous nerve) were localizedand anequal amount of localanesthetic (15ml) wasadministeredtoeachone.Aspirationtestwasrepeated onceinevery5mlduringtheinjections.Ananesthesiologist whodidnottakepartintherestofthestudypreparedthe localanesthetic solutions according torandomizationand
anotheranesthesiologist(CI)whowasunawareofthesyringe contenthasperformedalltheblockprocedures.GroupBwas administered30ml0.5%bupivacaineandGroupL30ml0.5% levobupivacaine.Fiveminutesaftertheendof injections, thesurgical areastarted tobecheckedwiththepin-prick test with5min intervals. Sensoryblock was assesedwith 3 point scale (0=Nosensory loss, 1=Loss of sensation to pin-prick,2=Loss of sensation totouch) and motor block wasevaluatedwithModifiedBromageScale(MBS;0=Normal musclefunction,1=Elbowflexion,2=Wristflexion,3=Full motorblock)andrecorded.
Motorblockonsettimewastakenasthetimebetween injectionoflocalanestheticandappearanceofMBS1,while sensory block onsettime wastaken asthe time between injectionoflocalanestheticandthelossofpainsensation with pin-prick stimuli. Surgery was allowed when ‘‘pin-prick’’waspositiveinthesurgeryarea.
Sensory block duration was defined as the duration betweensensoryblockonsetandfirstfeelingofpain,while motor block duration wasthe time between motor block onset and full arm mobility. These durations were deter-mined basedon patientreports at postoperative 4th,8th and24thhour.
SAP, DAP, MAP, HR, SpO2 of patients were recorded at
thebeginningofsurgery,at minutes5,10and15 ofblock administration,andthereafterwith10minintervals.
Incaseofpainsensationatthebeginningoforduringthe surgery,localanestheticinfiltration(prilocaine,5---10mlin 2%concentration)tothesurgicalsitewasplanned. Admin-istration50mcgfentanyl and/or1mg midazolamwasalso plannedincasesofpainorstressdespitelocalinfiltration. Thedoseswouldberecordedifadministered.
Allpatientcomplaintsduringandafterblock,all block-related complications and side effects of drugs were recorded.
Postoperative pain complaints were assessed on a ‘‘verbal ratingscale’’ (VRS) (0: nopain, 1: mild pain, 2: moderatepain,3:severepainand4:unbearablepain),and patientsatisfactionwasassessedat postoperativehour24 as‘‘notsatisfied,slightlysatisfied,andsatisfied’’.Thefirst analgesic (diclofenac iv) dose wasplanned in case of VRS >2. When patients werevisited in theclinic at hours 4---8 and24,complaintsofpainandtotalamount ofanalgesics takenwererecorded.
Statisticalanalysis
As a result of the power analysis we performed, it was decided thateach groupshould have at least a minimum of26cases(80%powerand0.05%˛error).Considering
pos-sibledatalossduetotechnicalreasons,bothgroups were admitted30patients.
Table1 Distributionofpatientswithrespecttodemographics(mean±SD).
GroupB GroupL t p
Age(years) 40.3±14.88 38.2±11.44 0.96 0.643
Bodyweight(kg) 73.8±12.59 73.9±13.81 −0.03 0.977
Height(cm) 171.43±8.34 173.1±7.98 −0.79 0.432
Table2 DistributionofpatientswithrespecttogenderandASAclassification.
GroupB GroupL
Gender
Male 22 73.30% 22 73.30% 2:0
Female 8 26.70% 8 26.70% p=1
ASA
I 19 63.30% 22 73.30%
II 9 30.00% 8 26.70% 2:2.27
III 2 6.70% 0.00% p=0.32
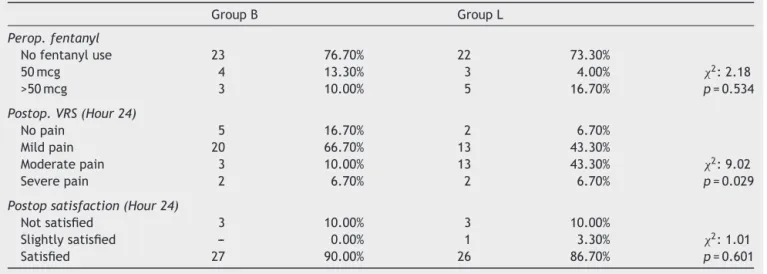
Table3 Comparisonofgroupswithrespecttoperoperativefentanyluse,VRSatpostoperativehour24andsatisfaction.
GroupB GroupL
Perop.fentanyl
Nofentanyluse 23 76.70% 22 73.30%
50mcg 4 13.30% 3 4.00% 2:2.18
>50mcg 3 10.00% 5 16.70% p=0.534
Postop.VRS(Hour24)
Nopain 5 16.70% 2 6.70%
Mildpain 20 66.70% 13 43.30%
Moderatepain 3 10.00% 13 43.30% 2:9.02
Severepain 2 6.70% 2 6.70% p=0.029
Postopsatisfaction(Hour24)
Notsatisfied 3 10.00% 3 10.00%
Slightlysatisfied --- 0.00% 1 3.30% 2:1.01
Satisfied 27 90.00% 26 86.70% p=0.601
Results
The study was implemented on 60 patients and no data
lossoccurred.Nostatisticallysignificantdifferenceexisted
betweenthedemographicdataandASAdistributionsofthe
patients(Tables1and2).HR,SAP,DAP,MAPandSpO2
val-uesweresimilaratallmeasurementtimesincomparisons withinandbetweenthegroups.
The patients in Groups B and L had similar peropera-tiveopioiduseandpostoperativesatisfactionrate(Table3).
Mean postoperative VRS scores of Group L patients was higher than that of Group B patients (p<0.05). Thirteen patients(43.3%)in Group Land3patients (10%)in Group Bhadmoderatepain(Table3).
The operationduration,motorandsensoryblocktimes ofpatientsinGroupBandGroupLdidnotvarysignificantly. ThesensoryandmotorblockonsettimesinGroupBpatients wereshorterthanGroupL(p<0.05)(Table4).
Motorblockscores ofGroup BandGroup Lpatients at minutes1,5,10,15,20,30,45and60werenotstatistically
Table4 Surgery,motorandsensoryblockdurations(meanhour±SD).
GroupB GroupL t p
Surgeryduration 1.48±0.61 1.52±0.66 −0.20 0.84
Motorblockduration 14.55±5.55 13.8±2.95 0.73 0.468
Table5 Motorandsensoryblockonsettimes(meanminute±SD).
GroupB GroupL p
Motorblockonsettime 5.07±4.07 9.2±7.9 0.0041
Sensoryblockonsettime 19.64±10.70 25.66±10.72 0.036
differentatshoulderlevel.Therateoffullmotorblock(MBS 3)atminutes1,5and10intheshoulderregionofGroupB patientswashigherthanthatinGroupLpatients.However,a statisticallymeaningfuldifferencewasnotfoundinthe com-parisonof alltimeintervals includingthese.Nostatistical
differencewasobservedbetweenmotor blockdistribution
ofGroupBandLpatientsatelbowlevelatallmeasurement times.
Whilepartialblockinthefingerswasseenin12patients inGroupL(40%),itwasseenin7patients(23.3%)inGroup B.Thedifferencewasnotstatisticallysignificant(Table5). PatientassessmentaccordingtoMBSshowedthatthere weremorepatientsinGroupBwhohadhigherblockquality atminutes5,10,15and20thaninGroupL(Table6).
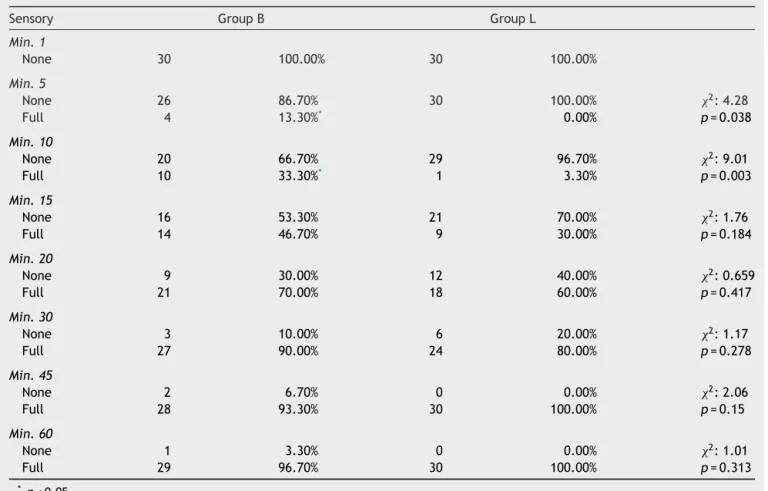
No statistical difference existed between the sensory blockassessmentofGroupBandLpatientsatminutes1,15, 20,30,45and60.SensoryblockratioinGroup Bpatients wasstatisticallyhigherthanthoseinGroupLatminutes5 and10(p<0.05)(Table7).
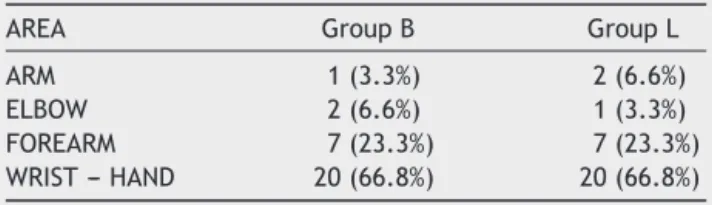
Amongbothgroupsofpatients,thedistributionofsurgery areaswassimilar(Table8).
Table6 Distributionofmeanmotorblockscorebytimein groupswithrespecttoMBSandpatientratio.
Minute GroupB GroupL
1 0 0
5 1(33.3%)* 1(13.3%)
10 2(26.7%)* 2(16.7%)
15 3(20.0%)* 3(3.3%)
20 3(36.7%)* 3(10.0%)
30 3(53.3%) 3(40.0%)
45 3(63.3%) 3(46.7%)
60 3(66.7%) 3(56.7%)
* p<0.05.
Partialblockoccurredin4patientsinGroupB.Allfour weregivenperoperative50mcgfentanylduetopain. Addi-tional localanesthetics were administeredto onepatient by thesurgery teamdue tomild painat thebeginning of surgery.Generalanesthesiawasinitiatedinthreepatients (10%)duetoblockagefailure.
Table7 Sensoryblockassessmentingroupswithrespecttotime.
Sensory GroupB GroupL
Min.1
None 30 100.00% 30 100.00%
Min.5
None 26 86.70% 30 100.00% 2:4.28
Full 4 13.30%* 0.00% p=0.038
Min.10
None 20 66.70% 29 96.70% 2:9.01
Full 10 33.30%* 1 3.30% p=0.003
Min.15
None 16 53.30% 21 70.00% 2:1.76
Full 14 46.70% 9 30.00% p=0.184
Min.20
None 9 30.00% 12 40.00% 2:0.659
Full 21 70.00% 18 60.00% p=0.417
Min.30
None 3 10.00% 6 20.00% 2:1.17
Full 27 90.00% 24 80.00% p=0.278
Min.45
None 2 6.70% 0 0.00% 2:2.06
Full 28 93.30% 30 100.00% p=0.15
Min.60
None 1 3.30% 0 0.00% 2:1.01
Full 29 96.70% 30 100.00% p=0.313
Table8 Distributionofsurgicalareasinthegroups.
AREA GroupB GroupL
ARM 1(3.3%) 2(6.6%)
ELBOW 2(6.6%) 1(3.3%)
FOREARM 7(23.3%) 7(23.3%)
WRIST---HAND 20(66.8%) 20(66.8%)
ElevenpatientsinGroupLexperiencedpartialblock.As therewasmildpainduringsurgeryin2patients,thesurgery
team administered local anesthesia. Two others needed
50mcgperoperativefentanylduetopain.Sixpatients(20%) requiredgeneralanesthesia.
Motorandsensoryblockrecoverytimesofpatientswho
requiredgeneralanesthesiawerealsorecordedattheend
ofsurgery.
Inthepostoperativestage,16patientsinGroupBand17 inGroupLwereadministeredanalgesicdrugsduetoVRS>3.
Otherpatients didnotneed postoperativeanalgesicdrugs
within thefirst 24h. The mean timebefore the need for
firstpostoperativeanalgesiawas16.61±8.05h inGroupB and14.37±7.27hinGroup L.Thedifferencewasnot sta-tisticallysignificant.
Sideeffects
GroupBpatientsexperiencedsignificantlymoresideeffects thanGroupL.FourpatientsinGroupB(13.3%)sufferedfrom sideeffects,whilenoneinGroupLdid.
TwopatientsinGroupBhadHorner’ssyndromeandthe
other 2 hadprolonged motorblockage (longerthan 24h).
These side effects were not seen in any of the patients
in Group L.Full recovery wasobserved at 8th hrvisit of
patientswhosufferedHorner’ssyndrome.
Discussion
An advantage of supraclavicular block is that the upper
extremity position does not affect application negatively
duringtheprocedure.4,5Eventhoughblockswithultrasound
areknowntoyield more successfuloutcomes,the impor-tanceofexperienceisalsomentionedinpreviousstudies.6,7
Wethereforepreferrednervestimulator(NS)inourstudyas wehadmoreexperiencewithit.Oursuccessfulblockrate withNSwas90%inGroupBand80%inGroupL.
Despite the high doses of bupivacaine and levobupi-vacaine used in peripheral blocks, serious cardiovascular, pulmonary or neurological complications arerare.8---13 Our
resultsarealsosimilar.
Coxetal.14comparedbupivacaineandlevobupivacaine
inbrachialplexusblock.Theyfoundnodifferencebetween the dose-dependent effects of 0.25% and 0.5% levobupi-vacaine; however, they found that 0.25% levobupivacaine hadsloweronset,shortermaintenanceandaloweroverall success rate than theother two groups (0.5% levobupiva-caine,0.5%bupivacaine).Theyreportedageneralsuccess rateof65---80%inrelationtotheanesthesiatechnique.This studyfoundlevobupivacainetobeappropriateforbrachial plexusblock.Itslowertoxicpotentialthanbupivacainealso supportsthis,andlevobupivacaineisexpectedtoincrease the safety margin in regional anesthesia. No statistically
meaningfuldifferencewasfoundbetweenthesensoryand motorblockonsettimesofthetwodrugs.
In our study,the motor and sensoryblock onset times
were meaningfully shorter in Group B than Group L
(p<0.05).Meanmotorblockonsettimewas5mininGroup Band9mininGroupL,whilemeansensoryblockonsettime was19mininGroupBand25mininGroupL.Eventhough thereisastatisticaldifferencebetweenthetwodrugs,we areoftheopinion thata6mindifferenceisnotof signifi-canceinclinicalapplication.
Another noteworthy finding from Cox et al.’s14 study
is that 0.5% levobupivacaine had the longest effect duration. They found that sensory block duration was 892min (approximately 14h) with 0.25% levobupivacaine; 1.039min(approximately 17h)with0.5%levobupivacaine; and 896min (approximately 15h) with 0.5% bupivacaine. Asonsensoryblock,0.5%levobupivacainehadthelongest effect duration on motor block as well (approximately 17.5h).However,thedifferencebetweengroupsregarding sensoryand motor block maintenance durationand block levelwasnotstatisticallymeaningful.Ourresultsalso cor-roboratethesefindings.
Lisanantti etal.13 found nomeaningful differencewith
respecttosensory blockquality between(45ml and0.5% concentration) ropivacaine, levobupivacaine and bupiva-caine at minutes 5, 10 and 15. There was a higher rate of achievinganesthesiaat adesired level at min 45 with ropivacaineandbupivacaine thanin comparisonwith lev-obupivacaine.Thefrequencyofobtainingsensoryandmotor blockatmin45wassimilaracrossall3groups.Meantotal sensory block duration was 17.1±6.5h in the levobupi-vacaine group, 17.8±7.2h in the bupivacaine group and 15.0±5.4hintheropivacainegroup.Thedifferencewasnot statistically significant. Mean total motor block durations were 19.5±8.0h with levobupivacaine, 19.3±7.7h with bupivacaine,and17.3±6.6hwithropivacaine.D’Ambrosio et al.15 compared 0.5% concentrations of ropivacaine,
bupivacaine and levobupivacaine in two different blocks (brachialandfemoral),andfoundthatropivacaineprovided fasterblockbuthadashorteranalgesiadurationthanthe othertwo.Theydidnotobserveadifferencebetween lev-obupivacaineandbupivacaine.Nodruginducedsideeffects aroseinthestudyand,consideringthepotentialcardiotoxic andneurotoxicsideeffectsofbupivacaine,theauthors con-cludedthat ropivacaineor levobupivacaine couldbe used dependingontheneedforanesthetic.
In our study,we did not found a statistical difference betweenthetotalmotorandsensoryblockdurationsofthe twogroups.Comparedtosimilarstudies,sensoryblock dura-tionwithlevobupivacaine wassimilarwhile that ofmotor blockwasshorter.Thisdifferencemaybeattributedto dif-ferencesintechniqueandmethods.
Postoperative VRS values in the study by D’Ambrosio et al.15 were higher in the ropivacaine group than the
other two (levobupivacaine and bupivacaine). No differ-enceexistedbetweenthelevobupivacaineandbupivacaine groups.
BpatientsthanthoseinGroupL,weareoftheopinionthat thedifferenceisnotsignificantinclinicalpracticesincethe scoresarebelow3.
Regarding postoperative analgesia, Liisanantti et al.13
found that first postoperative analgesia was needed at 17.8±7.2h in the bupivacaine group, 17.1±6.5h in the levobupivacainegroup,and15.0±5.4hin theropivacaine group. The difference was not statistically meaningful. D’Ambrosio et al.15 did not find any difference
regard-ing postoperative analgesia need with levobupivacaine andbupivacaine.Ourresultscorroboratethisfinding.Cox14
states that a sharp decline from 0.2% to0.01% has been observed in the last 30 years in incidences of systemic toxicitywith localanesthetics, andthat even though the incidenceofsystemictoxicityishighestinperipheralnerve blockswith7.5in10,000,theincidenceofneuraldamage islowestat1.9in10,000.Inourstudy,Horner’ssyndrome occurredin2patientsandprolongedparesthesiaoccurred in another2 in Group B.No complications were notedin GroupL.Notoxicityfindingsrelatedtobupivacaineor lev-obupivacainewaspresent ineithergroup.Onfollow-up,a permanentneurologicaldisorderwasnotdetectedinanyof thepatientswhodevelopedcomplications.
Insum, wefound that 30ml0.5% bupivacaineand lev-obupivacaine was enough to obtain motor and sensory supraclavicular block. Considering the higher side effect rateofbupivacaineanditspotentialcardotoxicsideeffects, we are of the opinion that levobupivacaine may be the preferreddrug for brachialplexus blockswith the supra-clavicularapproach.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.FosterRH,MarkhamA.Levobupivacaine:areviewofits pharma-cologyanduseasalocalanaesthetic.Drugs.2000;59:551---79.
2.Morgan GE, Mikhail MS, Murray MJ, et al. Peripheral nerve blocks. In: Clinical anesthesiology. 3rd ed. New York: Lange Medical Books/Mc Graw Hill Company; 2002. p.283---309.
3.CasatiA.Upperextremitymultiplestimulationtechniques.In: ChellyJE,editor.Peripheralnerveblocks.Philadelphia: Lippin-cottWilliams&Wilkins;2004.p.66---8.
4.ErsoyÖ,TürkmenC,BoyacıA,etal.Supraklavikülerveaksiller yaklas¸ımlauygulananbrakiyalpleksuskars¸ılas¸tırılması.Erciyes tıpdergisi.1994;16:210---6.
5.Franco CD,Vieira ZE. 1,001 subclavian perivascular brachial plexusblocks:successwithanevrestimulator.RegAnesthPain Med.2000;25:41---6.
6.ChanV,ParlasA,RawsonR.Ultrasound-guidedsupraclavicular brachialplexusblock.AnesthAnalg.2003;97:1514---7.
7.Albright GA. Cardiac arrest following regional anesthesia with etidocaine or bupivacaine. Anesthesiology. 1979;51: 285---7.
8.Knapik P, Gallert G, Knapik M. Contraversies regard-ing the use of 0.75% bupivacaine. Wiad Lek. 1992;45: 523---6.
9.Coussaye JE, EledjamJJ, Brugada J. Cardiotoxicity of local anesthetics.CanAnesthesiol.1993;41:589---98.
10.TuominenM,RosenbergPH,KalsoE.Bloodlevelsofbupivacaine after single dose, supplementary dose and during continu-ousinfusioninaxillaryplexusblock.ActaAnaesthesiolScand. 1983;27:303---6.
11.Brown DL, Ransom DM, Hall JA. Regional anesthesia and localanesthetic-inducedsystemic toxicity:seizurefrequency and accompanying cardiovascular changes. Anesth Analg. 1995;81:321---8.
12.BedderMD,KozodyR,CraigDB.Comparisonofbupivacaineand alcalinizedbupivacaineinbrachialplexus anesthesia.Anesth Analg.1988;67:48---52.
13.LiisananttiO,LuukkonenJ,RosenbergPH.Highdose bupiva-caine,levobupivacaine and inaxillary brachialplexus block. ActaAnaesthesiolScand.2004;48:601---6.
14.Cox CR, Checketts MR, Mackenzie N, et al. Comparison of S(−)-bupivacainein supraclavicularbrachial plexusblock.Br JAnaesth.1998;80:594---8.