REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
Comparison
of
waste
anesthetic
gases
in
operating
rooms
with
or
without
an
scavenging
system
in
a
Brazilian
University
Hospital
Leandro
Gobbo
Braz,
José
Reinaldo
Cerqueira
Braz,
Guilherme
Aparecido
Silva
Cavalcante,
Kátina
Meneghetti
Souza,
Lorena
Mendes
de
Carvalho
Lucio,
Mariana
Gobbo
Braz
∗UniversidadeEstadualPaulista‘‘JúliodeMesquitaFilho’’(UNESP),FaculdadedeMedicina,HospitaldasClínicas,Botucatu,SP, Brazil
Received8September2016;accepted24January2017 Availableonline18May2017
KEYWORDS
Inhaledanesthetics; Operatingrooms; Indoorairpollution; Occupational exposure
Abstract
Backgroundandobjectives: Occupationalexposuretowasteanestheticgasesinoperatingroom withoutactivescavengingsystemhasbeenassociatedwithadversehealtheffects.Thus,this studyaimedtocomparethetraceconcentrationsoftheinhalationalanestheticsisofluraneand sevofluraneinoperatingroomwithandwithoutcentralscavengingsystem.
Method: Wasteconcentrationsofisofluraneandsevofluraneweremeasuredbyinfrared ana-lyzeratdifferentlocations(neartherespiratoryareaoftheassistantnurseandanesthesiologist andneartheanesthesiastation)andattwotimes(30and120minafterthestartofsurgery)in bothoperatingroomtypes.
Results:All isofluraneandsevoflurane concentrations in unscavenged operating room were higherthantheUSrecommendedlimit(2partspermillion),regardlessofthelocationandtime evaluated.Inscavengedoperatingroom,theaverageconcentrationsofisofluranewerewithin thelimitofexposure,exceptfor themeasurementsnear theanesthesiastation,regardless ofthemeasurementtimes. Forsevoflurane, concentrations exceededthe limitvalue atall measurementlocationsandatbothtimes.
Conclusions:Theexposuretobothanestheticsexceededtheinternationallimitinunscavenged operating room. In scavengedoperating room, theconcentrations ofsevoflurane,and toa lesserextentthoseofisoflurane,exceededtherecommendedlimitvalue.Thus,theoperating roomscavengingsystemanalyzedinthepresentstudydecreasedtheanestheticconcentrations, althoughnottotheinternationallyrecommendedvalues.
©2017SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗Correspondingauthor.
E-mail:[email protected](M.G.Braz).
http://dx.doi.org/10.1016/j.bjane.2017.04.008
PALAVRAS-CHAVE
Anestésicos inalatórios; Salascirúrgicas; Poluic¸ãodoarem ambientesfechados; Exposic¸ão
ocupacional
Comparac¸ãoderesíduosdegasesanestésicosemsalasdeoperac¸ão
comousemsistemadeexaustãoemhospitaluniversitáriobrasileiro
Resumo
Justificativaeobjetivos: Aexposic¸ãoocupacionalaosresíduosdegasesanestésicosemsalas deoperac¸ão(SO)semsistemaativodeexaustãotemsidoassociadaaefeitosadversosàsaúde. Assim,oobjetivodoestudofoicompararosresíduosdosanestésicosinalatóriosisofluranoe sevofluranoemSOcomesemsistemadeexaustão.
Método: Concentrac¸õesresiduaisdeisofluranoesevofluranoforammensuradasporanalisador infravermelhoemdiferenteslocais(próximoàárearespiratóriadoauxiliardeenfermageme doanestesiologistaepróximoàestac¸ãodeanestesia)eemdoismomentos(30e120minapós oiníciodacirurgia)emambosostiposdeSO.
Resultados: Todasasconcentrac¸õesdeisofluranoesevofluranonasSOsemsistemadeexaustão forammais elevadas em relac¸ãoao valor limite recomendadopelos EUA(2 partespor mil-hão),independentemente dolocale momentoavaliados.NasSOcomsistema deexaustão, asconcentrac¸õesmédiasdeisofluranoficaramdentrodolimitedeexposic¸ão,excetoparaas mensurac¸õespróximasàestac¸ãodeanestesia,independentementedosmomentosavaliados. Paraosevoflurano,asconcentrac¸õesexcederamovalorlimiteemtodoslocaisdemedic¸ãoe nosdoismomentos.
Conclusões: Aexposic¸ão aambososanestésicosexcedeu olimite internacional nasSOsem sistemadeexaustão.NasSOcomsistemadeexaustão,asconcentrac¸õesdesevoflurano,eem menorextensãoasdeisoflurano,excederamovalorlimiterecomendado.Dessaforma,osistema deexaustãodasSOanalisadonopresenteestudodiminuiuasconcentrac¸õesdosanestésicos, emboranãotenhareduzidoavaloresinternacionalmenterecomendados.
©2017SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigo OpenAccess sobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Occupationalexposuretoresidualconcentrationsofinhaled (volatile)anestheticsinoperatingrooms(ORs)without scav-enging system has been associated with adverse health effects, such as headache, irritability, neurobehavioral changes,andDNAdamage.1
Although the cause-and-effect relationship has notyet been established,agenciesin severaldeveloped countries recommendlimitvaluesforexposuretoanestheticgasesto minimizehealthrisks.TheUSNationalInstituteof Occupa-tionalSafetyandHealth(NIOSH)2recommendsthevalueof
2partspermillion(ppm)asoccupationalexposurelimitto halogenatedinhalationalanesthetics.
Halogenatedanestheticsarethemostwidelyusedagents ininhalationalanesthesiaworldwide.Ananestheticpower measure refers to the minimum alveolar concentration (MAC). Inadult patients, thehalogenated sevoflurane has aMACofabout 2%,whichishigherthanthatofisoflurane (1.2%).3
Theuseofinhalationalanestheticsrequiresascavenging system toreduce both the OR environmental contamina-tion and occupationally exposed professionals. However, adequateORscavengingsystemsareuncommoninmost hos-pitalsindevelopingcountries.Evenwiththepresenceofan ORscavengingsysteminthesecountries,therearestilllarge differencesinefficiencybetweensystemsindevelopedand developingcountries.4
Duetothesubjectrelevanceandtheabsenceofnational data,this unpublished work aimedto compare the resid-ualconcentrationsofisofluraneandsevofluraneinORswith andwithoutananestheticgasscavengingsysteminapublic universityhospital.
Method
ThisstudywasapprovedbythelocalResearchEthics Com-mittee (4440-2012) and performed in a hospital with a theatersettingof 13ORs, sevenof whichwithout a scav-engingsystem,withonlyoneairconditioner,andsixwitha (partial)scavengingsystemwithonly25%ofcleanexternal air(thus,with75%airrecirculation),withsevenairchanges perhour. Regardingthe anesthesiastations,there wasno scavengingsystemexclusivetoinhalationalanesthetics.
The study wasperformed in the ORs, always withthe measurementofanestheticresiduesduringthefirstgeneral anesthesiaofthe day,underanesthesiamaintenancewith isofluraneorsevoflurane,in24patientswithtracheal intu-bationwithcuffedtube,whichwasfilledwithminimumseal pressuretoavoidleakageduringartificialventilation.
Bothisofluraneandsevofluraneconcentrationswereused around1MAC, accordingtopatient’s need,withfreshgas flow(FGF)of2Lmin−1incircularbreathingcircuitwithCO
Anesthesia Workstation
Operating table
1
Door Air conditioner
Measurement sites: Nursing assistant 1
2
3 1
2
3
Anesthesiologist Anesthesia Workstation
Figure1 Diagramofoperating rooms withair conditioner, withoutanesthetic gas scavenging system.Numbers indicate the measurementsites for residual concentration ofinhaled anesthetics.
Aportableanestheticgasanalyzer(InfraRan4-Gas Anes-theticSpecific VaporAnalyzer, Wilks Enterprise,USA) was usedtomeasuretheresidualconcentrationsofboth anes-thetics.Theanalyzerdetectstheanestheticconcentration inrealtimebyinfrared,andtheequipmentdetectionlimit rangesfrom0to50ppmforhalogenatedanestheticagents. Air samples weremeasured in three sites: the anesthesi-ologistandnursing assistantbreathingareas andnearthe anesthesia workstation breathing circuit (Figs. 1 and 2). Sampleswerecollected at twotimes:30 and120minutes (min)afterthestartofsurgery.
Mean residualconcentrations werecalculated for each inhalationalanestheticatbothtimes,atthethree measure-mentsitesandaccordingtotheORtype.Student’sttestwas usedtocompare times,ORtypes,andanesthetics.ANOVA wasusedtocomparethemeasurementsitesforeach anes-thetic,eachtimeandtypeofOR.Significancelevelslower than5%wereconsideredsignificant.
Results
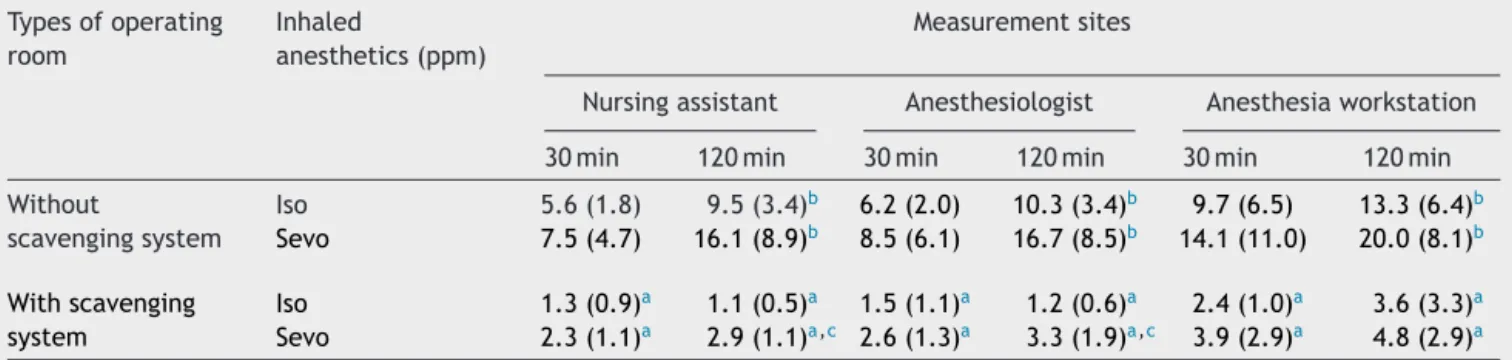
Table1showsthemeanresidualconcentrationsofisoflurane andsevoflurane measured in OR.Regarding the measure-mentsites,theresidualconcentrationvaluesinthenursing assistant and anesthesiologist breathingareas, aswell as intheanesthesiaworkstation,werenotdifferentfor both anesthetics,regardless oftheORtype(p>0.05), withthe highestvaluesclosetotheanesthesiaworkstation.
Concentrationsof both anesthetics werehigher in ORs without scavenging system in all sites and times mea-sured compared to those in ORs with scavenging system
Anesthesia Workstation
Area directly below the turbulent flow; central air
conditioning ventilation
Operating table
Door Air conditioner Measurement sites:
Nursing assistant 1
2
3 1
2
3
Anesthesiologist Anesthesia Workstation
Figure2 Diagramofoperatingroomswithcentralair condi-tionerandscavengingsystem(7airchangesperhour).Numbers indicate themeasurementsitesfor residual concentrationof inhaledanesthetics.
(p<0.001).Therewasasignificantincreaseinthe concen-trations of both isoflurane and sevoflurane at 120min of surgerycomparedto30minonly inthe ORswithout scav-engingsystematallmeasurementsites(p<0.01).
Sevofluraneconcentrationsweresignificantlyhigherthan thoseof isofluraneat 120min inthe nursingassistant and anesthesiologistbreathingareasinORswithscavenging sys-tem(p=0.02).
Discussion
Thepresentstudydemonstratedthat:(i)theuseof isoflu-rane and sevoflurane in ORs without an anesthetic gas scavengingsystemresultedinmeanresidualconcentrations that largely exceeded the 2ppm values recommended by NIOSH;(ii)ORswithscavengingsystemshowedmean resid-ualisofluraneconcentrationslowerthanthatrecommended byNIOSHattwoofthethreemeasurementsites;(iii)ORs withscavengingsystem showedmeanresidualsevoflurane concentrationsthatexceededtheNIOSHrecommended lim-itsatallsitesmeasured.
Thus, monitoring the concentrations of halogenated anesthetic gases in OR with and without a scavenging system, asevidenced inour study,demonstratedthe fun-damentalroleofascavengingsystemtoremoveanesthetic gasfromORs,reducingbothanestheticpollutionand occu-pationalexposure,particularlyregardingisoflurane.Modern ORscavengingsystemsconsistofalaminarflowsystemwith atleast15airchangesperhour,withoutairrecirculation.5
Table1 Residualconcentrationofisoflurane(Iso)andsevoflurane(Sevo)(meanandstandarddeviation)inpartspermillion (ppm)inoperatingroomswithandwithoutananestheticgasscavengingsystem.Measurementswereperformedatthreedifferent sitesat30and120minfromthestartofsurgery.
Typesofoperating room
Inhaled
anesthetics(ppm)
Measurementsites
Nursingassistant Anesthesiologist Anesthesiaworkstation 30min 120min 30min 120min 30min 120min Without
scavengingsystem
Iso 5.6(1.8) 9.5(3.4)b 6.2(2.0) 10.3(3.4)b 9.7(6.5) 13.3(6.4)b
Sevo 7.5(4.7) 16.1(8.9)b 8.5(6.1) 16.7(8.5)b 14.1(11.0) 20.0(8.1)b
Withscavenging system
Iso 1.3(0.9)a 1.1(0.5)a 1.5(1.1)a 1.2(0.6)a 2.4(1.0)a 3.6(3.3)a
Sevo 2.3(1.1)a 2.9(1.1)a,c 2.6(1.3)a 3.3(1.9)a,c 3.9(2.9)a 4.8(2.9)a
a p<0.001comparedwithoperatingroomswithoutscavengingsystemsatallmeasurementsitesat30minor120min. b p<0.01comparedwith30minintheoperatingroomswithoutscavengingsystem,atallsites.
c p=0.02comparedwithisofluraneat120minintheoperatingroomswithscavengingsystem.
has shown that mean concentrations of isoflurane4,6 and
sevoflurane7residueswerebelow2ppm.However,the
anes-thetic gas scavenging system present in the ORs of our surgicaltheater isconsidered partial,asitgeneratesonly sevenairchangesperhour,withairrecirculation,with tur-bulent flow system. Thus, this less effective technology mayexplainthehigherobservedresidualconcentrationsof sevoflurane, but notisoflurane. Due toits low anesthetic potency,theadministrationofsevofluraneshouldbedone atMACtwicethatofisoflurane,whichincreasesthe possi-bilityofagreaterresidualconcentrationofthisagentinthe ORs.
Inhalational anesthetics leakage from the anesthesia workstationmayalsohavecontributedtotheresidual anes-theticconcentrations.Infact,thehighestconcentrationsof sevofluraneandisofluranewerefoundneartheanesthesia workstationbreathingcircuit,althoughtherewerenoleaks fromtheDrägerFabiusanesthesiaworkstation.Itshouldalso be considered that the more modernanesthesia worksta-tionsarelikelytohavelessleakage,asthereis aneedto performtheleakagetestbeforeusingtheequipment.8Other
causesofORcontaminationincludefailuretoshutdownthe flowcontrolvalves,flushingthebreathingcircuitwithhigh FGF,leakage of inhaled anestheticduring fillingof vapor-izers, useof uncuffed trachealtube, anduse of highFGF (≥3Lmin−1).9
Indeed,moreeffortsareneeded toreduceexposureto inhalationalanesthetics.Frequentmonitoringofanesthetic gasresidualconcentrations inORsshouldbethefirststep towardunderstanding thevaluesofoccupationalexposure in the workplace. The proper installation and operation of the OR scavenging system and use of new anesthesia workstations, aswell asstafftraining,arealso important toreducethelevelsofoccupationalexposure.10 Moreover,
reducingFGF(≤1Lmin−1)isespeciallyimportantinan envi-ronmentwithoutanactivescavengingsystem.11Inaddition,
thereplacementofinhalationalanestheticsbyvenous anes-thetics, when possible, shouldbe done in the absenceof anadequatesystemtoremoveanestheticgasresiduesina surgicaltheather.4
Inconclusion,ourstudydemonstratedhighresidual con-centrations of isoflurane and sevoflurane in ORs without
a scavenging system, which considerably exceed the val-ues recommended by international agencies. In ORs with a partial scavenging system, the halogenated anesthetic concentrationsarelowerthaninORswithoutascavenging system,buttheexposure,particularlytosevoflurane,still exceedstherecommendedlimit.
Funding
This study was funded by Fundac¸ão de Amparo à Pesquisa do Estado de São Paulo (FAPESP), processes numbers: 2013/05084-8 and 2013/21130-0, and by Con-selhoNacionaldeDesenvolvimentoCientíficoeTecnológico (CNPq),processnumber471604/2013-5.GASCreceived sci-entific initiation grant from the Pró-Reitoria de Pesquisa (PROPe)/UNESP.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.CostaPaesER,BrazMG,LimaJT,etal.DNAdamageand antiox-idant status in medical residents occupationally exposed to wasteanestheticgases.ActaCirBras.2014;29:280---6. 2.NIOSH---NIOSHpocketguideforchemicalhazards.TheNational
Institute for Occupational Safety and Health of The United StatesofAmerica;1994.
3.NickallsR,MaplesonW.Age-relatediso-MACchartsfor isoflu-rane, sevoflurane and desfurane in man. Br J Anaesth. 2003;91:170---4.
4.WiesnerG,HarthM,SzulcR,etal.Afollow-upstudyon occu-pationalexposuretoinhaledanaestheticsinEasternEuropean surgeonsandcirculatingnurses.IntArchOccupEnvironHealth. 2001;74:16---20.
5.AIA---AmericanInstitutesofArchitects.Guidelinesfor construc-tionandequipmentofhospitalsandmedicalfacilities;1992. 6.HobbhahnJ,HoeraufK,WiesnerG,etal.Wastegasexposure
7.ByhahnC,HellerK, Lischke V,et al.Surgeon’s occupational exposure to nitrous oxide and sevoflurane during pediatric surgery.WorldJSurg.2001;25:1109---12.
8.TokumineJ,NittaK,HigaT,etal.Leakageinanesthesia circuits-a comparison between 1998 and 2005 investigations. Masui. 2007;56:453---8.
9.Oliveira CRD. Exposic¸ão ocupacional a resíduos de gases anestésicos.RevBrasAnestesiol.2009;59:110---24.
10.SartiniM,OttriaG,DalleraM,etal.Nitrousoxidepollutionin operatingtheatresinrelationtothetypeofleakageandthe numberofefficaciousairexchangesperhour.JPrevMedHyg. 2006;47:155---9.