www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Treatment
of
large
persistent
tracheoesophageal
peristomal
fistulas
using
silicon
rings
夽
Ibrahim
Erdim
a,
Ali
Ahmet
Sirin
a,
Bahadir
Baykal
a,
Fatih
Oghan
b,∗,
Ali
Guvey
b,
Fatma
Tulin
Kayhan
aaBakirkoySadiKonukEducationandResearchHospital,DepartmentofORL,Istanbul,Turkey bDumlupinarUniversity,FacultyofMedicine,DepartmentofORL,Kutahya,Turkey
Received24April2016;accepted22June2016 Availableonline21July2016
KEYWORDS
Voiceprosthesis; Siliconring; Fistula
Abstract
Introduction:Tracheoesophagealperistomalfistulaecanoftenbesolvedbyreducingthesize ofthefistulaorreplacingtheprosthesis;however,evenwithconservativetechniques,leakage aroundthefistulamaycontinueintotallaryngectomypatients.Also,severaltechniqueshave beendevelopedtoovercomethisproblem,includinginjectionsaroundthefistula,fistulaclosure withlocalflaps,myofascial flaps,orfreeflapsandfistulaclosureusingaseptalperforation siliconbutton.
Objective:Topresenttheresultsoftheapplicationofsiliconringexpandingthevoiceprosthesis inpatientswithlargeandpersistentperi-prostheticfistula.
Methods:Avoiceprosthesiswasfittedto42patientsafter totallaryngectomy.Leakage was detectedaroundtheprosthesisin18ofthese42patients.Fourpatientsdemonstrated improve-mentwithconservativemethods.Eightof18patientswhocouldn’tbecuredwithconservative methodsweretreatedbyusingprimarysutureclosureand4patientsweretreatedwithlocal flaps.Assiliconringwasappliedasaprimarytreatmentinthe2remainingpatientsandalso, appliedto2patientswhohadrecurrenceaftersuturerepairandto2patientswhohad recur-renceafterlocalflapimplementation.Siliconringswereusedinatotalof6patientsduetothe secondarytrachea-esophagealfistula.Patientsweretreatedwithprovox-1initiallyandlater withprovox-2.Atthetimeofleakagearoundthefistula,6patientshadprovox-2.
Results:Fistulaeweretreatedsuccessfullyin6patients,andeffectivespeechofpatientswas preserved.Patientsexperiencednoadaptationproblem.Prosthesischangingtimewasnot dif-ferent between silicon rings expanded andnormal prosthesis applied patients. Silicon ring combinedvoiceprosthesiswasused26times;therewasnorecurrenceinfistulacomplication during29±6monthsfollowup.
夽 Pleasecitethisarticleas:ErdimI,SirinAA,BaykalB,OghanF,GuveyA,KayhanFT.Treatmentoflargepersistenttracheoesophageal peristomalfistulasusingsiliconrings.BrazJOtorhinolaryngol.2017;83:536---40.
∗Correspondingauthor.
E-mail:[email protected](F.Oghan).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.06.011
Conclusion: Siliconringsformodifiedexpandedvoiceprosthesisseemstobeaneffective treat-mentforpersistentperi-prostheticleakage,forboth,fistulaclosureandpreservingthepatients speech.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Prótesevocal; Aneldesilicone; Fistula
Tratamentodefístulaperiestomaltraqueoesofágicagrandeepersistentecomanéis desilicone
Resumo
Introduc¸ão: Fístulastraqueoesofágicaspersistentespodemserresolvidasatravésdareduc¸ãodo tamanhodafístulaousubstituic¸ãodaprótese;noentanto,mesmocomtécnicasconservadoras, opertuitoemtornodafístulapodecontinuarempacientescomlaringectomiatotal.Alémdisso, váriastécnicastêmsidodesenvolvidasparasuperaresseproblema,incluindoinjec¸õesaoredor dafístula,fechamentodafístulacomretalhoslocais,retalhomiofasciais,ouretalhoslivrese fechamentodafístulausandoumbotãoseptaldesilicone.
Objetivo: Apresentarosresultadosdaaplicac¸ãodeaneldesiliconeparaexpansãodaprótese vocalempacientescomgrandesfístulasperiprotéticaspersistentes.
Método: Prótesevocalfoicolocadaem42pacientesapóslaringectomiatotal,efístulafoi detec-tadaaoredordapróteseem18desses42pacientes.Quatropacientesobtiverammelhoracom métodosconservadores.Oitodos18pacientesquenãoobtiveramsucessocommétodos conser-vadoresforamtratadosusandosuturaprimáriaequatropacientesforamtratadoscomretalhos locais.Umaneldesiliconefoiaplicadoinicialmentenosdoispacientesrestantese,também, aplicadoadoispacientesquetiveramrecorrênciaapósatécnicadesuturaeadoispacientes quetiveramrecorrênciaapósautilizac¸ãoderetalholocal.Nototal,seispacientesreceberam anéisdesiliconeemdecorrênciadafístulatraqueoesofágicasecundária.Ospacienteshaviam sidotratadoscomprovox-1inicialmenteeposteriormentecomprovox-2.Nomomentodetecc¸ão dafístulaemtornodoestoma,seispacienteshaviamrecebidoprovox-2.
Resultados: Afístulafoitratadacomsucessoemseispacientes.Alémdisso,apósotratamento afalafoimantidadeformaeficaznospacientes.Nãohouveproblemadeadaptac¸ão.Otempo detrocadapróteseexpandidacomosanéisdesiliconenãofoidiferentedotempoqueseleva paraacolocac¸ãodaprótesenormal.Oaneldesiliconecombinadocomaprótesevocalfoiusado 26vezesempacientesnaépocadatrocadepróteseenãohouverecorrênciadafístuladurante os29±6mesesdeacompanhamento.
Conclusão:Os resultados sugeremque em casosde grandes fístulasperi-prostéticas persis-tentes, anéis expandidosde silicone eprótese vocalmodificada, sãoeficazes tanto para o fechamentodafístulacomoparaamanutenc¸ãodafaladopaciente.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Oneofthemostimportantproblems ofpatientswhohave
undergonetotallaryngectomyislossofspeech.Avoice
pros-thesis can solve the problem in most patients; however,
there can be numerous complications, including a
peris-tomal fistula.1---4 This frequent complication can result in
severemorbidity,includingaspirationpneumoniaand
mal-nutrition,orevenmortality.5---7
Such problems can be solved by reducing the size
of the fistula or replacing the prosthesis; however, even
with conservative techniques, leakage around the fistula
may continue. Several techniques have been developed
toovercomethisproblem,includinginjectionsaroundthe
fistula8---11; fistula closure with local flaps,12 myofascial
flaps,1,13,14 free flaps;1,5 and fistula closure using a septal
button.6,13
Theproblemscausedbysmallfistulas(5---10mm)are
eas-iertoovercomecomparedtothosecausedbylargefistulas;
indeed,itmaynotbepossibletosolvetheproblemscaused
bylargefistulas,andcomplicationssuchasspeechlossand
morbiditymayresultfromintervention.
Here, we report the application of a silicone ring
expanded voice prosthesis in patients who had a
large-sized fistula and persistent peri-prosthetic
Methods
Avoiceprosthesiswasfittedto42patientsaftertotal
laryn-gectomybetweenJanuary2005andDecember2011.Ethical
approvalwasobtainedfromethicalcommitteeasanumber
of32/2015.Leakagewasdetectedaroundtheprosthesisin
18 of the 42 patients. While fourpatients improved with
conservativemethods,eightpatientsimprovedatfirstwith
conservativemethodsbutlaterdidnotrespondtotherapy,
and six patients did not respond to conservative therapy
eveninitially.
Eightoffourteenpatientswhocouldnotbecuredwith
conservative methods were treated using primary suture
repair, andfour patients were treatedwith localflaps. A
siliconeringwasappliedinitiallytotwopatientswithwide
fistulas.Asiliconeringwasalsoappliedtotwopatientswho
hadrecurrenceaftersuturerepairandtwopatientswhohad
recurrenceafterlocalflapimplementation.Intotal,silicone
ringswerefittedtosixpatients.
FiveofthepatientswhoreceivedProvox2widenedwith
siliconeringsweremaleandonewasfemale.Themeanage
was57±11years.Fourpatientsunderwentbilateral
func-tionalneckdissection,one underwentbilateralfunctional
neckdissectionandrightsubmandibularglandexcision,and
oneunderwentrightfunctional,leftradicalneckdissection
andreconstructionwith a pectoralismajormyocutaneous
flap. Three patients received radiotherapy, one patient
receivedradiotherapyandchemotherapy,andtwopatients
receivedneither.Asecondarytracheoesophagealfistulawas
opened in all patients. The patients were treated with
Provox 1 first and followed later with Provox 2. At the
timeofleakagearoundthefistula,sixpatientshadProvox
2 (outer diameter,22.5 F; Atos Medical, Hörby,Sweden).
Theminimumandmaximumdiametersofthefistulaswere
1.5cm×1.5cmand2cm×2.5cm,respectively.
Preparationandapplicationofthesiliconering expandedvoiceprosthesis
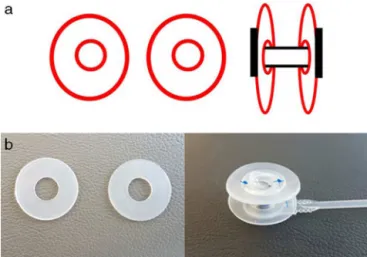
Twosiliconeringsmadeofwingsofseptalbuttonsor
inex-pensive silicone plaques were prepared according to the
widthofthefistulaandinnerdiameterofthevoice
prosthe-sis.Theseringsengagedwiththetrachealandesophageal
flangesofthevoiceprosthesis(Fig.1a).Thesiliconerings
werefixedtothevoiceprosthesisusing3.0non-absorbable
sutures --- 2 at the posterior flange and 2 at the anterior
flange(Fig.1b).Carewastakenthatthepreparedringsdid
nothavesharppiecesontheouterside.Thewingmatched
withtheesophagusengagedwiththefistula.Thevoice
pros-thesiscombinedwiththesiliconeringswasappliedtothe
tracheoesophagealfistula.Last,theuppersideof the
tra-chealflangeofthevoiceprosthesiswassuturedtoskinon
thetracheostomausing3.0non-absorbablesutures(Fig.2a
andb).
Results
Fistulas were treated successfully in six patients. After
treatment,effectivespeechofthepatientswasmaintained.
Noadaptationproblemoccurredinthepatients.Asilicone
ring combinedwith a voice prosthesis wasused 26 times
Figure 1 (a) Schematization of expanded voice prosthesis with siliconerings.(b) Silicone ringsand preparedexpanded voiceprosthesis.
Figure 2 (a) The rings engaged with the tracheal and esophageal flangesofthevoiceprosthesis. (b) Heupperside ofthetracheal flangeofthe voiceprosthesiswas suturedto skinonthetracheostomausing3.0non-absorbablesutures.
in patients when it was time to change the prosthesis,
andtherewasnorecurrenceoffistulacomplicationsduring
29±6 months of follow-up. Prosthesis changing timewas
183.5±58.7(min---max:21---424)daysfortotal42patients,
and 171.6±74.8 (min---max: 32---384) daysfor silicon ring
time was not statistically different between these two
groups(Non-parametricMann---WhitneyUtestwasusedand
p=0.163).
Discussion
Thesizeofthefistulaandwhetherthepatienthasreceived
radiotherapy are essential factors in the closure of
tra-cheoesophagealfistulas.Thesuccessrateoffistulaclosure
is decreased inpatients whoreceivedradiotherapy,
espe-ciallywhensurgicaltechniques wereapplied.1,14 However,
septalbutton6,13,15andsiliconeringexpandedProvox,which
weused,aremoreeffectiveinpatientswhohavereceived
radiotherapy becausethese techniques have no effecton
woundhealing.
Inmost patients,theproblemcanbesolvedbyusinga
smallerprosthesis.Iftheproblempersists,spontaneous
clo-sureofthefistulacanoccurafterdetachingtheprosthesis.
However,iffistulaclosurewiththismethodfails,the
appli-cationofvarioustechniquescouldberequiredaccordingto
thesizeofthefistula.16
For small fistulas (5---10mm), local suture-repair
tech-niques are appropriate and the success rate is between
60% and 100%.14 Additionally, some studies have reported
the effectiveness of collagen,8 hyaluronate,9 calcium
hydroxyapatite,10andGM-CSF11injectionsforsmallfistulas.
Jacobs et al.17 used the ‘‘submucosal purse-string
suture’’ technique in 20 patients to constrict the fistula
and reuse the voice prosthesis. They were successful in
16 of20 patients (80%).While theyachievedsuccess in 9
of 16 patients in thefirst suture trial, repetitivesuturing
wasrequiredfortheremaining7patients.Thistechniqueis
simpleandcouldbethefirstchoicemethodfor
constrict-ingfistulas.However,itcannotbeconsideredeffectivefor
medium-orlarge-sizedfistulas.Additionally,tracheostoma
narrowness, which excluded one patient from the study,
makes the application of this technique difficult.17 Lee
et al.12 reached the fistula tract by making an incision
fromthe9to3o’clockdirectionontheupperpart ofthe
tracheostoma.Theyelongatedtheincisiontowardthe
ster-nocleidomastoid(SCM) muscle.Aftersplitting the trachea
and esophagus, theyrepaired the esophagealdefect with
absorbablesutures.Rotatingtheinferiorly-basedflap,using
the right SCM muscle, they sutured this on the repaired
esophageal site. Also, they repaired the trachea using
absorbable sutures. The patient’s fistula was closed
com-pletely, and the patient could not speak with the voice
prosthesis.Thelimitationsofthisstudyarethatthe
diame-terofthefistulawasnotstatedandthetechniquewastried
ononly onepatient.12 Additionally,Wong etal.15 usedan
SCM muscle flaptwice consecutivelyto closea
tracheoe-sophagealfistula,buttheywerenotsuccessful.Therefore,
theyclosedthefistulawithaseptalbutton.
Mobashiretal.16removedthefistula,makinganincision
fromthe9to3o’clockdirectionontheupperpart ofthe
tracheostomainmiddle-sizedfistulas(maximumfistulasize,
1.5cm×1cm).Theyputnon-absorbablesuturesonthe
tra-cheal and esophageal parts of the fistula and closed the
fistulaby tying.Inall patients,the fistulaclosed
success-fully,butthepatientscouldnotspeak.
Forlargefistulas,large-basedflapsandfreeflapscould
beused.The pectoralmajormyofascialflap(PMMF)13 and
radialforearmfree flaparemajortypes of flaps usedfor
largefistulas.Inthesesurgeries,therecanbemorbidityat
thedonorsites.RadialflapsaremoresuitablethanPMMFs
becausetheyarethinandshapedeasily.WithaPMMF,
dys-phagiaand constriction of the tracheal lumen may occur
becauseofthemasseffect.Witharadialforearmfreeflap,
microvascularanastomosisisneeded.Thisistechnically
dif-ficult, and the operation time is long. Also, the vascular
status of the patient is important.14 Despite this surgical
technique,theclosure oflarge-sizedfistulas couldnotbe
achievedinpreviousreports.5,13Inparticular,incaseswhere
thevesselinthepediclecouldnotnourishtheflap,closure
ofthefistulacouldnotbeachievedbecauseofnecrosis.
Analternativeapproachforalarge-sizedfistulaisa
sep-tal button.6,13,15 Septal buttons can be appliedeasily and
rapidlyandarewelltolerated.Theypreventaspirationand
pulmonaryinfections,andpatientscaneatanddrink
com-fortably. Salivary bypass tubes (Boston Medical Products,
Westborough, MA) can also be used for eating and
drink-ingin patientswithlarge fistulas. However,depending on
theduration of usage of the tube, large granulomasmay
developonthetipandfeedingcandeteriorate,13makingthe
patientuncomfortable.Anotheruncomfortablesituationis
therequirementforsuturerepairofthesalivarybypasstube
toneckskintostabilizeit.13 Forthesereasons,septal
but-tonusageis recommendedfor largefistulas, orforfailure
ofthe flapsusedfor fistulaclosure.6,13,15 When avoidance
ofsurgical morbidity is required and ifthereare medical
contraindications,thistechniquecouldberecommended.13
However,thedisadvantagesofaseptalbuttonarethatthe
patientcannotspeakagain,andtherecanbefungal
prolif-erationaroundthebutton.15
Hilgeretal.18demonstratedthetreatmentof
tracheoe-sophagealfistulasbyattachingasiliconeringtothetracheal
flangeoftheprosthesis.Theypreventedfistularecurrence
in29of32patientsbutfailedin3patients;subsequently,
in9patients,thefistularelapsedandadditional
interven-tions were needed. Therefore, in 20 of 32 patients they
obtainedsuccessfulresults,butin12 patients(37.5%)the
fistulacouldnotbetreatedusingthismethodalone.Inthis
study,foreithersmallorlargefistulas,thesametechnique
wasattemptedonallpatients.Inourstudy,2patientswith
alocalflapwhohadarelapse,2patientswhohadarelapse
aftersuturerepair,and2patientswhohadverylarge
fistu-las(6patientsintotal)receivedinterventionwithsilicone
rings.The differencebetween our technique and that of
Hilgeretal.18istheattachmentofthesiliconeringtoboth
thetrachealandesophagealflangesofthevoiceprosthesis
insteadofattachingthesiliconeringtoonlyoneside.Inthis
way,weaimedtopreventrecurrentaspiration.
EricBlomdesignedadjustable abi-flanged fistula
pros-thesis(Blom-Singer®)madefrommedical-gradesiliconefor
the management of hypopharyngeal fistulas. Our silicone
ringsaresimilartothisprosthesisbutourringsareusedto
preventtracheoesophagealfistulas. The prosthesisflanges
designedbyBlomaresoft,flexible,andtranslucentlikeour
rings.
With a septal button, the patient cannot speak again
despiteclosureofthetracheoesophagealfistula.Similarly,
speak. Also, there is a failure risk with flaps because of
necrosisoftheflaporopeningofthesuturesontheflaps.
However,usingourtechnique,thefistulawasclosedandthe
patientretainedtheabilitytospeak.Additionally,theneed
forsurgery wasprevented. Inpatients whohavereceived
radiotherapy,thesuccessrateoffistulaclosuredecreases1,14
witheitherlocalorothersurgicaltechniques.Inourstudy,
thesuccessratewasindependentofradiotherapy.However,
oneof the disadvantages of ourtechnique is the need to
preparesiliconeringseverytimetheprosthesisischanged.
Conclusions
Although we demonstrated our technique only in six
patients, we managed to treat resistant enlarged
tra-cheoesophageal fistula while preserving speech without
periprostheticleakage recurrence.According toourstudy
the use of expanded voice prosthesis with silicone rings
forlargetracheoesophagealfistulaswithpersistentleakage
appearstobeeffective.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.HosalSA,MyersEN.HowIdoit:closureoftracheoesophageal puncturesite.HeadNeck.2001;23:214---6.
2.OpdeCoulBM,HilgersFJ, BalmAJ,TanIB,vandenHoogen FJ,vanTinterenH.Adecadeofpostlaryngectomyvocal reha-bilitationin318patients:asingleInstitution’sexperiencewith consistent applicationofprovox indwellingvoiceprostheses. ArchOtolaryngolHeadNeckSurg.2000;126:1320---8.
3.Hutcheson KA, Lewin JS, Sturgis EM, Kapadia A, Risser J. Enlarged tracheoesophageal puncture after total laryngec-tomy: a systematic review and meta-analysis. Head Neck. 2011;33:20---30.
4.DayangkuNorsuhazenahPS,BakiMM,MohamadYunusMR,Sabir HusinAtharPP,AbdullahS.Complicationsfollowing tracheoe-sophagealpuncture:atertiaryhospitalexperience.AnnAcad MedSingapore.2010;39:565---8.
5.Wreesmann VB, Smeele LE, Hilgers FJ, Lohuis PJ. Closure of tracheoesophageal fistula with prefabricated revascular-izedbilaminarradialforearmfreeflap.HeadNeck.2009;31: 838---42.
6.Mirza S, Head M, Robson AK. Silicone septal button in the managementofalargetracheo-oesophageal fistulafollowing primary puncture ina laryngectomy. ORL JOtorhinolaryngol RelatSpec.2003;65:129---30.
7.HutchesonKA,LewinJS,SturgisEM,RisserJ.Multivariable anal-ysisofriskfactorsforenlargementofthetracheoesophageal punctureaftertotallaryngectomy.HeadNeck.2012;34:557---67. 8.Remacle M, Declaye XJ. Gax-collagen injection to correct anenlargedtracheoesophagealfistula fora vocalprosthesis. Laryngoscope.1988;98:1350---2.
9.LuffDA,IzzatS,FarringtonWT.Viscoaugmentationasa treat-ment for leakage around the Provox 2 voice rehabilitation system.JLaryngolOtol.1999;113:847---8.
10.KasbekarAV,ShermanIW.Closureofminortracheoesophageal fistulae with calcium hydroxlapatite. Auris Nasus Larynx. 2013;40:491---2.
11.MargolinG, MasucciG, Kuylenstierna R,BjörckG, Hertegård S, Karling J. Leakage around voice prosthesis in laryngec-tomees: treatment with local GM-CSF. Head Neck. 2001;23: 1006---10.
12.Lee LM,Razi A. Three-layer technique toclose a persistent tracheo-oesophagealfistula.AsianJSurg.2004;27:336---8. 13.SchmitzS,VanDammeJP, HamoirM.Asimpletechniquefor
closureofpersistenttracheoesophagealfistulaaftertotal laryn-gectomy.OtolaryngolHeadNeckSurg.2009;140:601---3. 14.KochM,ZenkJ,BirkS,AlexiouC,IroH.Surgicalclosureof
per-sistenttracheoesophagealfistulasbyesophagealsuturingand cranialtransposition ofthe trachea. Otolaryngol Head Neck Surg.2010;143:843---4.
15.WongBY,KurianM,ChidambaramA.Alternativemanagement ofleakingtracheoesophagealfistulaafterlaryngectomyusing nasalseptalbutton.ClinOtolaryngol.2011;36:97---9.
16.MobashirMK,BashaWM,MohamedAE,AnanyAM.Management ofpersistenttracheoesophagealpuncture.EurArch Otorhino-laryngol.2014;271:379---83.
17.JacobsK, DelaerePR,VanderPoorten VL.Submucosal purse-stringsutureasatreatmentofleakagearoundtheindwelling voiceprosthesis.HeadNeck.2008;30:485---91.