www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Association
between
maxillary
sinus
pathologies
and
healthy
teeth
夽
,
夽夽
Gina
D.
Roque-Torres
a,∗,
Laura
Ricardina
Ramirez-Sotelo
a,
Sergio
Lins
de
Azevedo
Vaz
b,c,
Solange
Maria
de
Almeida
de
Bóscolo
a,
Frab
Norberto
Bóscolo
aaDepartmentofOralDiagnosis,FaculdadedeOdontologiadePiracicaba,UniversidadeEstadualdeCampinas(UNICAMP),
Piracicaba,SP,Brazil
bDentalRadiology,UniversidadeEstadualdeCampinas(UNICAMP),Piracicaba,SP,Brazil
cDepartmentofDentalClinic,SchoolofDentistry,UniversidadeFederaldoEspíritoSanto(UFES),Vitória,ES,Brazil
Received24March2014;accepted9December2014 Availableonline10December2015
KEYWORDS
Molartooth;
Premolartooth;
Maxillarysinus;
Dentalroot;
Conebeamcomputed
tomography
Abstract
Introduction:Theproximityoftherootstothemaxillarysinuscancreateavarietyofrisks.
Objective: Toevaluatetherelationshipbetweentherootsofhealthyteethandthemaxillary sinus,aswellastheoccurrenceofsinuspathologies.
Methods:Three radiologistsanalyzed109conebeam computedtomography(CBCT)images. TheKappatestwasusedtoassesstheintra-andinter-rateragreement.Thechi-squaredtest andprevalenceratiowereusedtotestthehypothesisthatrootsofhealthyteethinthemaxillary sinusfavoredtheoccurrenceofsinuspathologies(p=0.01).
Results:Intra-andinter-rateragreementrangedfromgoodtoexcellent.Thechi-squaredtest demonstratedastatisticallysignificantdifference(p=0.006)betweenthetoothrootsin dis-easedmaxillarysinuses(6.09%)andthoseinnormalsinuses(3.43%).Theprevalenceratiotest showedastatisticallysignificanthigherprevalenceoftoothrootsindiseasedsinusesthanin normalsinuses(p<0.0001).Rootsinthemaxillarysinuswere1.82timesmoreassociatedwith diseasedsinuses.
夽 Pleasecitethisarticleas:Roque-TorresGD,Ramirez-SoteloLR,VazSLA,deAlmeidadeBóscoloSM,BóscoloFN.Associationbetween
maxillarysinuspathologiesandhealthyteeth.BrazJOtorhinolaryngol.2016;82:33---8.
夽夽Institution:DepartmentofOralDiagnosis,PiracicabaSchoolofDentistry,StateUniversityofCampinas,Piracicaba,SP,Brazil.
∗Correspondingauthor.
E-mail:[email protected](G.D.Roque-Torres).
http://dx.doi.org/10.1016/j.bjorl.2015.11.004
1808-8694/©2015Associac¸ãoBrasileirade OtorrinolaringologiaeCirurgiaCérvico-Facial.Published byElsevierEditoraLtda.Allrights
Conclusion:Dental roots inthe maxillarysinus arealmost twice as likelyto be associated withdiseasedsinusesthannormalsinuses.Healthyteethwhoserootsareinsidethemaxillary sinusmayinduceaninflammatoryresponseinthesinusmembrane.Itissuspectedthatdental proceduresmayexacerbatethecondition.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Dentemolar;
Dentepré-molar;
Seiomaxilar;
Raizdentária;
Tomografia computadorizada
defeixecônico
Relac¸ãoentredoenc¸asnoseiomaxilaredenteshígidos
Resumo
Introduc¸ão:Aproximidadedasraízescomoseiomaxilarpodecriarumavariedadederiscos.
Objetivo:Avaliararelac¸ãoentreasraízesdosdenteshígidoscomoseiomaxilar,assimcomo comaocorrênciadedoenc¸assinusais.
Método: Trêsradiologistasanalisaram109imagensdetomografia computadorizadadefeixe cônico(TCFC).OtesteKappaavaliouaconcordânciaintraeinterexaminadores.Ostestesde Qui-quadradoe RazãodePrevalência foramutilizadospara testarahipótese deque raízes dedenteshígidosdentrodoseiomaxilarfavorecemaocorrênciadoenc¸assinusais (nívelde significância=0,01).
Resultados: Aconcordânciaintraeinterexaminadoresvarioudeboaaexcelente.Oteste Qui-quadrado mostrou uma diferenc¸a estatisticamente significante (p = 0,006) entre as raízes dentáriasdentrodoseiomaxilarpatológico(6,09%)eaquelasdentrodoseionormal(3,43%). OtestedeRazãodePrevalênciamostrouumaocorrênciaderaízesdentáriasdentrodeseios patológicos estatisticamentemaiordoque dentrodeseiosnormais(p < 0,0001). Asraízes dentrodoseiomaxilarforamencontradas1,82vezesmaisassociadasaseiospatológicos.
Conclusão:Raízesdentárias dentrodoseiomaxilarsãoquaseduas vezesmais associadasa seiospatológicosdoqueaseiosnormais.Denteshígidosquetêmraízesdentrodoseiomaxilar podem induzirumarespostainflamatóriadamucosa sinusal.Suspeita-se queprocedimentos odontológicospossamagravartalsituac¸ão.
©2015Associac¸ãoBrasileira deOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicadopor ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Maxillarysinusescanvaryinsizeandshapefromone
indi-vidualtoanother,orevenbetweentherightandleftsides
inthesameindividual.Inapproximatelyhalf ofthe
popu-lation,theirlength alsovaries. The floorof the maxillary
sinusextendsintothealveolarprocessbetweentherootsof
adjacentteeth,creatingelevations anddepressionscalled
‘‘extensions,’’withnarrowcorticalareas.1,2Through
histo-logicalsections,ithasbeenradiographicallydemonstrated thatmost of the roots projecting intothe maxillarysinus werein fact surrounded bya thin layer of cortical bone, withperforationspresent in 14---28%of cases.3 Under
nor-malconditions,therelationshipbetweenthetoothandthe floorofthemaxillarysinusconsistsofeitherathinlayerof compactbonethatprovidessupporttotheapical periodon-talligamentfibers, towhichit firmlyadheres,or thereis adirectrelationshipwiththemaxillarysinus mucosa.The innerliningofthemaxillarysinuscavityisdevoidof perios-teum;therefore,intheabsenceofathinlayerofintervening bone,theperiodontaltissuesareindirectcontactwiththe basalsurfaceofthesinusmucosa.2
Therootsoftheupperpremolars,molars,and occasion-ally the canine teeth have a close relationship with the
maxillarysinus;insomecases,theymayevenprotrudeinto it.4---6 It has been demonstrated that the closerthe tooth
apexistothefloorofthemaxillarysinus, thegreaterthe impacton antraltissue.7 This relationship canresult in a
varietyofrisks,especiallyforcertainsurgicalprocedures, such as tooth extraction and implant placement, or dur-ingendodonticor orthodontictreatments.4,5,8Anaccurate
description of the relationship between theapices of the upper teethandthe lowerwall of themaxillarysinus, as well as the thicknessof the cortical bone between these structures,isessentialforplanningdentalprocedures.
Dental radiographs, such as panoramic radiography, consistoftwo-dimensionalimagesand,assuch,are inappro-priateand/oroflittleuseforaccuratemorphometric assess-mentofbonerelationships.4Incaseswherethepanoramic
radiographrevealsapossiblerelationshipbetweenatooth that has undergone intervention and its contactwith the adjacent maxillary sinus, evaluation by cone beam com-puted tomography (CBCT) can assist in dental treatment planning.Thisimagingmodalityallowsforathorough anal-ysis of theanatomical relationship between themaxillary sinus and the roots of the upper teeth,4,6,9,10 thus
superimposition.11 This techniqueis superiortomulti-slice
computed tomographydue toitshigher imageresolution, reducedradiationexposure,andlowerequipmentcost.12
Inapicalperiodontitis,aperiodontaldisease,13,14
treat-mentwithimplantsandextractionofupperpremolarsand molars15 mayincreasetheriskofpathologicalprocessesin
theadjacentmaxillarysinus.Oftheodontogenicsinus dis-eases,apicalperiodontitisandperiodontaldiseaseaccount for 83% of all cases having dental origin.13,16 The most
frequentmaxillarysinuspathologiesaresinusmucosal thick-eningandmucousretentioncysts,withaprevalenceranging from 8% to29% and 2% to36%, respectively.16---19 Another
studyhasreportedaprevalencerateofodontogenic maxil-larysinusitisrangingfrom10%to86%.20
There are few studies describing the relationship betweenmaxillarysinusdiseasesandhealthyupper poste-riorteeth in contactwiththe maxillary sinus. Therefore, inordertoanswerthisquestion,thisstudyaimedto evalu-atetherelationshipbetweentherootsofhealthyteethwith healthyanddiseased(mucosalthickeningandmucous reten-tioncysts)maxillarysinusesthroughCBCT.Thisresearchcan helpidentifycorrelationsbetweenteethandsinusdiseases withoutcausalfactors.
Methods
For this study,109 CBCT images were selected, obtained independentlyofthisresearchfordiagnosisandtreatment planningpurposes.Allimagesbelongedtothedigitalarchive oftheRadiologyClinic.Afterapprovalofthestudy proto-col bythe local ResearchEthics Committee(Protocol No. 084/2012),thesampleconsistedof78womenand31men, meanage22years(range:18---30years),withoutdistinction byrace,gender,socialclass,orothersocioeconomic charac-teristics.Inallimages,bothmaxillarysinuses(n=218)and therootsofallpremolarsandmolarsonbothsides(n=1875) wereevaluated.
CT scans were obtained using the I-CAT Classic scan-ner(ImagingSciencesInternational---Pennsylvania,United States), using the following exposure parameters: 8mA, 120kVp, acquisition time of 40s, 13cm×17cm field of
vision,andvoxelsizeof0.25mm.Imageswithgood sharp-ness,density,andcontrastwereselected.Theimageshad topresenttheapicesoftheupperposteriorteethandthe maxillarysinusalongtheirentirelength.
Forinclusioninthestudy,theimageshadtopresent com-plete permanent dentition,with noevidence of any type of dental pathology, with fully formed root apexes, and withoutthepresenceofsupernumeraryteeth.Mostreasons forCBCTimagingcomprisedtemporomandibularjoint disor-der,orthodontictreatment,andevaluationofthirdmolars. Imageswithevidenceofcariouslesions,prostheticcrowns, filledrootcanal,periapicallesions,bifurcationlesions,and moderateorseverebonelosswereexcluded.
Three expertsindentalradiology,whohada minimum experience of two years in CBCT, were selected for the study.Inlowlightconditions,theseexpertsindependently assessedthepresenceorabsenceofsinusdisorders(mucosal thickeningormucousretentioncysts),andthe topographi-calrelationshipbetweenthemaxillarysinusandeachapex of the upper posterior teeth (firstand second premolars,
aswellasfirstandsecondmolars).Onlytheseteethwere assessed,astheirroot apexesaretheclosesttothe max-illary sinus floor. The relationship of the root with the maxillarysinuswasdeterminedasfollows:rootsinthe max-illarysinus,androotsoutsideofthemaxillarysinus(apexes incontactornotwiththelimitsofthemaxillarysinus cor-tical).This topographicalevaluation (Fig. 1)of the teeth wasperformedusingmultiplanarreconstruction(MPR).All viewsattainablewithinthesoftwareweremadeavailable for thedetection of pathological findings;thus, the eval-uators were allowed to adjust the brightness, contrast, andzoomof theimage. The useof filters wasnot autho-rized.
Themodewasobtainedfromthethreeevaluations,both forthetopographicrelationship betweentherootandthe maxillarysinusesandfor thepresence orabsenceofsinus pathology. The frequency of tooth roots inside and out-side of the maxillary sinus and the presence or absence of pathology in the maxillary sinus were quantified and subsequentlyassessedwiththechi-squaredtestand preva-lenceratio.Ap-value<0.01wasconsideredasstatistically significant.
Thirty days after the first evaluation, 27% of the sample was re-evaluated for reliability measurements. Inter-andintra-ratercorrelationwascalculatedusingthe Kappa test (poor agreement, 0.40; moderate agreement, 0.40---0.59; good agreement, 0.60---0.74; excellent agree-ment,0.75---1.00).
Results
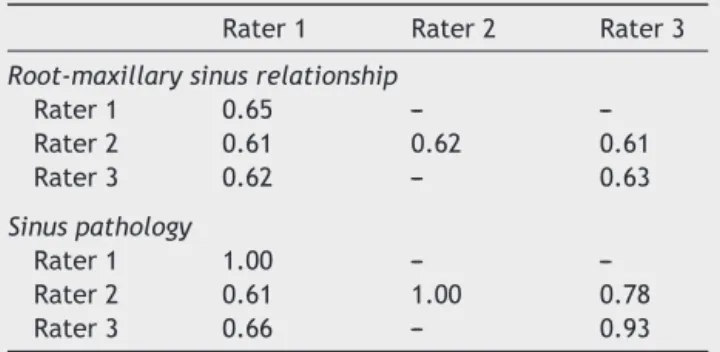
TheKappavaluesforinter-andintra-rateragreementinthe assessmentsofroot-maxillarysinusrelationshipandofsinus disordersrangedfromgoodtoexcellent(Table1).
Thefrequency ofdiseasedmaxillarysinus (34.98%)was lowerthanthatofnormalmaxillarysinuses(65.02%).Most rootswerelocatedoutsidethemaxillarysinus(95.63%).This wasobservedinnormalmaxillarysinuses(96.57%),aswell asindiseasedsinuses(93.91%;Table2).
The chi-squared test demonstrated that there was a statistically significant difference (p=0.006) between the occurrenceoftoothrootswithindiseasedmaxillarysinuses (6.09%) and within normal sinuses (3.43%). A statistically greater difference was observed in the prevalence of toothroots withindiseased sinusesthanin normalsinuses (p<0.0001).Rootslocatedwithinthemaxillarysinuseswere
Table1 Kappavaluesforinter-andintra-rateragreement.
Rater1 Rater2 Rater3
Root-maxillarysinusrelationship
Rater1 0.65 ---
---Rater2 0.61 0.62 0.61
Rater3 0.62 --- 0.63
Sinuspathology
Rater1 1.00 ---
---Rater2 0.61 1.00 0.78
Pathologic sinus
Roots within sin
us
Roots outside sin
us
Normal sinus
Figure1 Thesinuscavitieswereclassifiedasdiseasedornormal.Thetoothrootswereconsideredtobeinsideoroutsidethe sinus.
Table2 Numberofrootsinsideandoutsidediseasedandnormalmaxillarysinuses.
Diseasedsinus,n(%) Normalsinus,n(%) Total,n(%)
Rootsoutsidethemaxillarysinuses 632(93.91) 1208(96.57) 1840(95.63) Rootsinsidethemaxillarysinuses 41(6.09) 43(3.43) 84(4.37)
Total 673 1251 1924
2=7387;p=0.006.
foundtobepresent1.82timesmorefrequentlyindiseased
sinuses(95%confidenceinterval:1.67---1.98).
The stratification of teeth group with the diseased
sinuses,in increasingorder,wasasfollows:first premolar
(0%),lowersecondpremolar(7.31%),firstmolar(41.46%),
andsecondmolar(51.21%).Theorderfornormalsinuswas
asfollows:firstpremolar(4.65%),secondpremolar(6.97%),
secondmolar(37.2%),andfirstmolar(51.16%;Table3).
Table3 Numberofrootsinsidediseasedandnormalmaxillarysinuses,bytoothgroup.
Diseasedsinus,n(%) Normalsinus,n(%) Total,n(%)
Secondmolar 21(51.21) 16(37.2) 37(44.04)
Firstmolar 17(41.46) 22(51.16) 39(46.42)
Secondpremolar 3(7.31) 3(6.97) 6(7.14)
Firstpremolar 0(0) 2(4.65) 2(2.38)
Discussion
This study aimed to investigate the relationship between
toothrootsinthemaxillarysinusesandthepresenceofsinus
diseases.Thepatientsinthissampledidnotpresentdental
diseasessuchascaries,periapicallesions,filledrootcanals,
orsignificantalveolarboneloss.
The topographic root-maxillary sinus relationship was
assessedusingCBCTimagesobtainedfromanarchive.
Stud-ieshaveshownthatwhenpanoramicradiographwasusedas
amethodofassessment,theroot-maxillarysinus
relation-shipwasimproperlydeterminedin39---57%ofcases.5,21The
literature has alsoshown that the reliabilityin detecting sinus diseases,suchasmucosalthickening,is higherusing CBCTthan2-DX-rays.22Consequently,CBCTwasconsidered
tobeareliablemethodforthepurposesofthepresentstudy. Threeexpertsindentalradiology,whohadatleasttwo yearsexperiencewithCBCTimages,evaluatedtheimagesof thisstudyindependently;themodeofthethreeevaluations wasthenobtained.Theinter-rateragreementwasmeasured bytheKappatest.Thismethodologyisrarelyappliedin simi-larstudies,whichoftenuseonlyoneevaluator,12,20,23ortwo
evaluatorswho then reach aconsensus,22,24,25 and do not
present statistical dataregarding theagreementbetween evaluators.Inthisstudy,intra-andinter-rateragreements regardingthetooth-maxillarysinusrelationshipweregood. For sinus conditions, the inter-rater agreement was also good,butfor raters2and3,itwasexcellent.The differ-encesfoundinthisaspectofthestudymayberelatedtothe factthattheexpertswerefreetoevaluatetheMPRimages aspreferred.Thismayalsoreflectthedifficultyin visualiz-ingthinalveolarcorticalplatesintheregionwheretheroots wereincontactwiththemaxillarysinus.Forfuturestudies, itisrecommendedthattheevaluationofMPRimagesshould bestandardized;however,stillimagesshouldnotbeused, asCBCTrequiresadynamicassessment,comprisingallcuts. Mucosal thickening and mucous retention cysts were groupedasdiseasedsinuses.Thesinusmucosaisconsidered asthickenedwhenthemembraneis2---6mmthick.The eti-ologicalfactorsarerelatedtosometypeofirritation,such asodontogeniccystsorallergy.19,26---31Lightmucosal
thicken-ingofthemaxillarysinusisanormalfindinginasymptomatic patients,32butathickeninggreaterthan2mmcanbe
asso-ciatedwithmaxillarysinusitis.33 Usingprevious studies as
reference,mucosaeatleast3mmthickwereconsideredas thickenedin thepresent study.26,34Mucousretentioncysts
arebodiesthatdevelopasaresultofablockageofthesinus ostiumandusuallyresolvespontaneously.Theyarecommon findings in CBCTimages, but cannotbe detected without propertrainingindentalradiology.35Althoughtheyare
usu-ally present in asymptomatic patients, it is important to disclosetheminCBCTimagereports.
The topographic relationship between tooth roots and the maxillary sinus has been studied in the literature. In onestudy,4theauthors reportedthat twoof the38study
subjects(5%)hadrootsthatprotrudedintothesinuscavity. Asimilarrate(10%)wasobservedinanotherstudy.6
There-fore,theincidenceoftoothroots inthemaxillarysinusin thepresentstudyisinagreementwiththeliterature.4,6Oral
surgeons should be aware of the amount of bone around themaxillarysinus,sothatthe necessaryprecautions can betaken toavoidperforation of thesinus membrane and
introductionofforeignbodiesintothemaxillarysinusduring dentaltreatments.3,36
Theliteraturehasshownthat,duetotheclose relation-shipbetweentheteethandthefloorofthemaxillarysinus, dentalinfectionscanextendtothemaxillarysinus.24Direct
contactbetweenperiodontaltissuesandsinusmucosacan occurbecauseoftheproximityofthemaxillarysinusandthe upperposteriorteethimplantedinthealveolarprocess.
Maxillary sinus infections andmucosal thickening have been identified in 2% of patients with dentulous superior maxillas.18 However, these authors did not find mucous
retention cysts in edentulous patients, which may sug-gestanodontogenicetiologyfor thiscondition.Inanother study,37 75% of cases withmaxillarysinusitis were
associ-atedwithdentalconditions.Otherstudieshaveshownthat periapicallesions19,38andperiodontaldisease12,19,23,24,39are
associatedwithsinuspathologies.Ithasbeendemonstrated that,in casesof apicalperiodontitis,when thetip ofthe tooth root wasin contactwith the floorof the maxillary sinus,theincidenceofmucosalthickeningwaslowerthan when thetipoftherootexceededthefloorofthemaxillary sinus.25
Of all the groups of teeth, the tomographic distance betweentheuppersecondmolarrootapexandthemaxillary sinusfloorisreportedtobethesmallestamongall maxil-laryposterior teeth.4,40 In line withthese reports, in the
presentstudythegroupofteethwiththemostdentalroots withindiseased sinus wasthesecond molar.Likewise,the firstmolarhadmorerootsinsidenormalmaxillarysinuses, althoughthisnumberwasquiteclosetothatofthesecond molar.
Amongthelimitations ofthisstudy,thelack ofclinical dataonpatientsevaluatedbyCBCTisnoteworthy.Itisalso importanttohighlightthatwedidnotanalyzethe histolog-icalsamplesthatmoreaccuratelydetermine thedifferent pathologicalchangesinthemaxillarysinustissue.The den-talradiologistswhoevaluatedtheCBCTimageswerefree toadjustthesoftware,sotherewaslittlestandardization intheassessmentoftheimages.
Conclusions
Inthestudiedsample,toothrootswithinthemaxillarysinus werealmosttwiceaslikelytobeassociatedwith patholog-icalmaxillarysinusesthannormalmaxillarysinuses.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.WaiteDE.Maxillarysinus.DentClinNorthAm.1971;15:349---68.
2.McGrowanDA,BaxterPW,JamesJ.Themaxillarysinusandits dentalimplications.1sted.London:Wright;1993.p.1---25.
3.Wehrbein H, Diedrich P. The initial morphological state in the basally pneumatized maxillary sinus --- a radiological---histological study in man. Fortschr Kieferorthop. 1992;53: 254---62.
floorandtheapicesofthemaxillaryposteriorteeth.OralSurg OralMedOralPathol.1992;73:345---6.
5.SharanA,MadjarD,HashomerT.Correlation between maxil-larysinusfloortopographyandrelatedrootpositionofposterior teethusingpanoramicandcross-sectionalcomputed tomogra-phyimaging.OralSurgOralMedOralPatholOralRadiolEndod. 2006;102:375---81.
6.KilicC,KamburogluK,PehlivanS,OzenT.Anassessmentofthe relationshipbetweenthemaxillarysinusfloorandthemaxillary posteriorteethroottipsusingdentalcone-beamcomputerized tomography.EurJDent.2010;4:462---7.
7.Selden H. Endo-Antral syndrome and various endodontic complications.JEndod.1999;25:389---93.
8.HaumanCH,ChandlerNP,TongDC.Endodonticimplicationsof themaxillarysinus:areview.IntEndodJ.2002;35:127---41.
9.HoweR.Firstmolarradicularbonenearthemaxillary sinus: acomparison ofCBCT analysisand grossanatomic dissection for smallbonymeasurement. OralSurgOralMedOralPathol OralRadiolEndod.2009;108:264---9.
10.Nair UP, Nair MK. Maxillary sinusitis of odontogenic origin: cone-beam volumetric computerizedtomography-aided diag-nosis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;110:e53---7.
11.Lofthag-Hansen S, Huumonen S, Grondahl K, Grondahl HG. Limitedcone-beamCTandintraoralradiographyforthe diagno-sisofperiapicalpathology.OralSurgOralMedOralPatholOral RadiolEndod.2007;103:114---9.
12.Brüllmann DD,SchmidtmannI,HornsteinS, SchulzeRK. Cor-relationofconebeam computedtomography(CBCT)findings inthemaxillary sinus withdentaldiagnoses:a retrospective cross-sectionalstudy.ClinOralInvestig.2012;16:1023---9.
13.MelenI,LindahlL,AndreassonL,RundcrantzH.Chronic max-illary sinusitis. Definition, diagnosis and relation to dental infections and nasal polyposis. Acta Otolaryngol. 1986;101: 320---7.
14.AbrahamsJJ,GlassbergRM.Dentaldisease:afrequently unrec-ognized cause of maxillary sinus abnormalities. AJR Am J Roentgenol.1996;166:1219---23.
15.Doud-GalliSK,LebowitzRA,GiacchiRJ.Chronicsinusitis com-plicatingsinusliftsurgery.AmJRhinol.2001;15:181---6.
16.Engström H, Chamberlain D, Kiger R, Egelberg J. Radio-graphicevaluationoftheeffectofinitialperiodontaltherapy on thickness of the maxillary sinus mucosa. J Periodontol. 1988;59:604---8.
17.Bhattacharyya N. Do maxillary sinus retention cysts reflect obstructivesinusphenomena.ArchOtolaryngolHeadNeckSurg. 2000;126:1369---71.
18.MathewAL, PaiKM,SholapurkarA.Maxillarysinusfindingsin theelderly:apanoramicradiographicstudy.JContempDent Pract.2009;10:E041---48.
19.ValloJ, Suominen-TaipaleL,HuumonenS, SoikkonenK, Nor-bladA.Prevalence ofmucosal abnormalitiesofthemaxillary sinus and their relationship to dental disease in panoramic radiography: results from the Health 2000 Health Examina-tionSurvey.OralSurgOralMedOralPatholOralRadiolEndod. 2010;109:e80---7.
20.Ritter L, Lutz J, Neugebauer J. Prevalence of pathologic findingsinthemaxillarysinusincone-beamcomputerized tomo-graphy. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;111:634---40.
21.FreisfeldM,DrescherD,SchellmannB, SchüllerH. The max-illarysixth-yearmolaranditsrelationtothemaxillarysinus. Acomparativestudybetweenthepanoramictomogramandthe computedtomogram.FortschrKieferorthop.1993;54:179---86.
22.LowKM,DulaK,BürginW, VonArxT.Comparisonof periapi-calradiographyandlimitedcone-beamtomographyinposterior maxillaryteethreferredforapicalsurgery.OralSurgOralMed OralPatholOralRadiolEndod.2007;103:114---9.
23.Phothikhun S, Suphanantachat S, Chuenchompoonut V, Nis-apakultornK.Cone-beamcomputed tomographicevidenceof the association between periodontal bone loss and mucosal thickening of the maxillary sinus. J Periodontol. 2012;83: 557---64.
24.ArijiY,ObayashiN,GotoM,IzumiM,NaitohM,KuritaK,etal. Rootsofthemaxillaryfirstandsecondmolarsinhorizontal rela-tiontoalveolarcorticalplatesandmaxillarysinus:computed tomographyassessmentforinfectionspread.ClinOralInvestig. 2006;10:35---41.
25.LuY,LiuZ,ZhangL,ZhouX,ZhengQ,DuanX,etal. Associ-ationsbetweenmaxillarysinusmucosalthickeningandapical periodontitisusingcone-beamcomputedtomographyscanning: aretrospectivestudy.JEndod.2012;38:1069---74.
26.GordtsF,ClementPAR,Destryker B,DesprechinsB,Kaufman L.PrevalenceofsinusitissignsonMRIinanon-ENTpaediatric population.Rhinology.1997;35:154---7.
27.LimWK,RamB,FasulakisS,KaneKJ.Incidentalmagnetic res-onanceimagesinusabnormalitiesinasymptomaticAustralian children.JLaryngolOtol.2003;117:969---72.
28.MehraP,MuradH.Maxillarysinusdiseaseofodontogenicorigin. OtolaryngolClinNorthAm.2004;37:347---64.
29.ObayashiN,ArijiY,GotoM,IzumiM,NaitohM,KuritaK,etal. Spreadof odontogenic infectionoriginating in themaxillary teeth:computerizedtomographicassessment. OralSurgOral MedOralPatholOralRadiolEndod.2004;98:223---31.
30.MadaniG,BealeTJ.Differentialdiagnosisinsinonasaldisease. SeminUltrasoundCTMRI.2009;30:39---45.
31.CarmeliG,ArtziZ,KozlovskyA,SegevY,LandsbergR.Antral computerizedtomographypre-operativeevaluation: relation-shipbetweenmucosalthickeningandmaxillarysinusfunction. ClinOralImplantsRes.2011;22:78---82.
32.SavolainenS,EskelinM,Jousimies-SomerH,YlikoskiJ. Radio-logicalfindingsinthemaxillarysinusesofsymptomlessyoung men.ActaOtolaryngolSuppl.1997;529:153---7.
33.RakKM,NewellJD2nd,YakesWF,DamianoMA,LuethkeJM. Paranasalsinuseson MRimages ofthe brain:significance of mucosalthickening.AJRAmJRoentgenol.1991;156:381---4.
34.Rege IC, Sousa TO, Leles CR, Mendonc¸a EF. Occurrence of maxillary sinus abnormalities detected by cone beam CT in asymptomaticpatients.BMCOralHealth.2012;10:12---30.
35.AhmedF, Brooks SL, Kapila SD. Efficacy of identifying max-illofacial lesions in cone-beam computed tomographs by orthodontistsand orthodonticresidentswiththird-party soft-ware.AmJOrthodDentofacialOrthop.2012;141:451---9.
36.Khongkhunthian P,Reichart PA.Aspergillosisofthemaxillary sinusasacomplicationofoverfillingrootcanalmaterialinto thesinus:reportoftwocases.JEndod.2001;27:476---8.
37.MailletM,BowlesWR,McClanahanSL,JohnMT,AhmadM. Cone-beamcomputedtomographyevaluationofmaxillarysinusitis. JEndod.2011;37:753---7.
38.NenzénB,WelanderU.Theeffectofconservativerootcanal therapy onlocalmucosal hyperplasia in themaxillary sinus. OdontolRevy.1967;18:295---302.
39.CasamassimoPS,LillyGE.Mucosalcystsofthemaxillarysinus: aclinicalandradiographicstudy.OralSurgOralMedOralPathol. 1980;50:282---6.