Brazilian
Journal
of
OTORHINOLARYNGOLOGY
www.bjorl.org
ORIGINAL
ARTICLE
Balloon
laryngoplasty
for
acquired
subglottic
stenosis
in
children:
predictive
factors
for
success
夽
,
夽夽
Rebecca
Maunsell
a,
Melissa
A.G.
Avelino
b,c,d,∗aHospitaldeSumaré,UniversidadeEstadualdeCampinas(UNICAMP),Campinas,SP,Brazil bPontifíciaUniversidadeCatólicadeGoiás(PUC-GO),Goiânia,GO,Brazil
cHospitaldaCrianc¸adeGoiânia,Goiânia,GO,Brazil dUniversidadeFederaldeGoiás(UFG),Goiânia,GO,Brazil
Received11December2013;accepted24May2014 Availableonline23July2014
KEYWORDS
Laryngostenosis; Laryngoplasty; Dilatation; Child
Abstract
Introduction:The treatment ofsubglottic stenosisin children remainsa challenge for the otorhinolaryngologist,andmayinvolvebothendoscopicandopensurgery.
Objective: Toreportthe experience oftwo tertiary facilities inthe treatment ofacquired subglotticstenosisinchildrenwithballoonlaryngoplasty,andtoidentifypredictivefactorsfor successofthetechniqueanditscomplications.
Methods:Descriptive,prospectivestudyofchildrendiagnosedwithacquiredsubglotticstenosis andsubmittedtoballoonlaryngoplastyasprimarytreatment.
Results:Balloonlaryngoplastywasperformedin37childrenwithanaverageageof22.5months; 24presentedchronicsubglotticstenosisand13acutesubglotticstenosis.Successrateswere 100%foracutesubglotticstenosisand32%forchronicsubglotticstenosis.Successwas signifi-cantlyassociatedwithacutestenosis,initialgradeofstenosis,childrenofasmallerage,and theabsenceoftracheostomy.Transitorydysphagiawastheonlycomplicationobservedinthree children.
Conclusion: Balloonlaryngoplastymaybeconsideredthefirstlineoftreatmentforacquired subglotticstenosis.Inacutecases,thesuccessrateis100%,andalthoughtheresultsareless promisinginchroniccases,complicationsarenotsignificantandthepossibilityofopensurgery remainswithoutprejudice.
© 2014Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:MaunsellR,AvelinoMA.Balloonlaryngoplastyforacquiredsubglotticstenosisinchildren:predictivefactors forsuccess.BrazJOtorhinolaryngol.2014;80:409---15.
夽夽
Institution:UniversidadeFederaldeGoiás(UFG),Goiânia,GO,Brazil.
∗Correspondingauthor.
E-mail:[email protected](M.A.G.Avelino).
http://dx.doi.org/10.1016/j.bjorl.2014.07.012
PALAVRAS-CHAVE
Laringoestenose; Laringoplastia; Dilatac¸ão; Crianc¸a
Laringoplastiacombalãoparaestenosesub-glóticaadquiridanainfância:fatores preditivosdesucesso
Resumo
Introduc¸ão:Otratamentodasestenosessubglóticasemcrianc¸asaindarepresentaumdesafio paraootorrinolaringologista,epodeenvolvertantoprocedimentosendoscópicosquanto cirur-giasreconstrutivasabertas.
Objetivo:Apresentaraexperiênciadedoisservic¸osterciáriosnomanejodasestenoses subglóti-casadquiridasemcrianc¸as,atravésdalaringoplastiacombalãoeidentificarfatorespreditivos desucessoeascomplicac¸ões.
Método: Estudodescritivoprospectivodecrianc¸ascomestenosesubglóticaadquirida submeti-dasàlaringoplastiacombalãocomotratamentoprimário.
Resultados: Foramincluídas37crianc¸as(médiadeidade22,5meses):24crianc¸asportadoras deestenosesubglóticacrônicae13deestenosesubglóticaaguda.Ataxadesucessodo trata-mentofoide100%paraoscasosagudose32%paraoscasoscrônicos.Osucessodotratamento tevecorrelac¸ãosignificativacom:tempo deevoluc¸ãodaestenose,grauinicial daestenose, menoridadedascrianc¸aseaausênciadetraqueostomiaprévia.Disfagiatransitóriafoiaúnica complicac¸ãoobservadaemtrêspacientes.
Conclusão:Alaringoplastiacombalãopodeserconsideradacomoprimeiralinhadetratamento nasestenosessubglóticas.Noscasosagudosataxadesucessoéde100%eoganho,mesmoque parcialnoscasoscrônicos,éinsento decomplicac¸õessignificativasenãotrazprejuízopara cirurgiasreconstrutivasposteriores.
©2014Associac¸ãoBrasileira deOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicadopor ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Inrecentyears,therehasbeenareductionofmortalityin neonatalintensive care units (ICUs) due tothe impactof recenttechnologicaladvancesintheperinatalarea.1 Asa
consequence,prolongedorotrachealintubationincreasedin
frequency,andincontrasttoadults,inwhomtracheostomy
isawellestablishedprocedureforthesecases,inthe
pedi-atricagegroupthisindicationiscomplex.2
Thus,anincreaseinacquiredsubglotticstenosis(SGS)has
beenobservedinchildren.SGSisanarrowingofendolarynx,
representingoneofthemostcommoncausesofstridorand
respiratorydistressinchildren.Thepediatricpopulationis
themostcommonlyaffected,becausethisisthenarrowest
regionoftheairwayatthisage.SGSmaybecongenitalor
acquired.Theacquiredformisresponsiblefor90%ofcases
ofsubglotticnarrowinginchildrenandisusuallysecondary
toprolongedtrachealintubation.
The treatment of acquired stenosis may involve
endo-scopicprocedures,bothintheacutephaseandthechronic
phase.Withinthearsenalofendoscopicprocedures,theuse
ofballoon dilatation or balloon laryngoplastyis becoming
popularacrosstheworldasaprimarytherapeuticoption.3In
theacutephase,oneoftherapeuticoptionsistracheostomy.
Despitetheimmediateresolutionofrespiratoryfailure,the
necessarycare,mainlyinthecase ofsucklinginfantswith
tracheostomy,isconsiderable,causingmuchanguish,fear,
andsociallimitationforcaregiversandforthechild.Therisk
of obstruction of the tracheostomy tube inside and
espe-cially outside the hospitalsetting cannot beignored, nor
theriskofdeath.Furthermore,thetracheostomyitselfcan
createadditionalcomplicationstotheairway,suchas
col-lapse,stenosis,andpersistenttrachealgranulationtissue.4
Itmust alsobeconsidered that tracheostomydoes not
solvethe problem ofhealing of theinflammatory process
alreadyembeddedinthesubglotticregion,andoften
chil-dren withtracheostomy after an intubation for laryngitis
evolvetoSGSthatisonlydiagnosedlater.
In chronic SGS, open surgeries for laryngeal
recon-struction, when carefully planned, exhibit high rates of
resolution. However, these procedures require the
coor-dination of an experienced team for postoperative care,
involving sedationweaningandthemanagementof
unsta-bleairways.Moreover,theseoperationsinvolverisksofgraft
infection,dehiscence,sepsis,andrestenosis,whichshould
not be underestimated. Thus, the management of these
patientsremainsabonafidechallengetothe
otorhinolaryn-gologist.
Balloon dilatation has been usedto treat laryngeal or
tracheal stenosis in children as early as the 1980s, with
encouragingresults.5Themainadvantageofthistechnique,
incomparisonwithothermethodsofendoscopicdilatation
withtracheal tubesand dilators,isthe possibilityto
pro-motean outwardexpansion,eveninthepresence ofvery
reducedlumen.Itisspeculatedthatitsuse,incomparison
withothermethodsofdilatation,promoteslesstissueinjury
and,thus,lessscarformation.
In a systematic review and meta-analysis in 2013 on
balloon laryngoplasty in cases of pediatric SGS, Lang and
Brietzke3 concludedthatthistreatment hasagood
short-termsuccessrate,withrarecomplications;andthatfailures
The objectiveof thepresentstudywastodemonstrate
theexperienceoftwotertiaryservicesinthemanagement
of SGS secondary to tracheal intubation in children, with
balloonlaryngoplastyasaprimarytreatment,andtorelate
thepredictorsoftechnicalfailureanditscomplications.
Methods
This was a prospective, descriptive study of children
diagnosed with acquired SGS after tracheal intubation,
undergoing balloon laryngoplasty as a primary treatment
fromAugustof 2011toSeptemberof 2013in two
depart-ments of otorhinolaryngology in tertiary hospitals. The
procedureswereperformedineach oftheservicesbythe
same surgeons, with training and experience in pediatric
airwaymanagement.
Patientsolderthan14years,withlessthanthreemonths
of follow-up, undergoing other previous laryngeal
proce-dures,withcongenitallaryngealstenosis,andthosewhose
parentsor guardiansrefusedtosigntheinformedconsent
wereexcluded.
Thisstudywasapprovedbytheethicscommitteesofeach
departmentundernumbers 002/2011and001/2011. After
beinginformedabouttheprocedureanditsrisks,allparents
orguardianssignedaninformedconsent.
Allenrolled patientswereevaluatedfor age,lengthof
stenosis,numberofdilatations,degreeofinitialsubglottic
stenosis,andpresenceoftracheostomy.
The childrenwerefurtherdividedintotwogroups: the
groupofchronicSGS,i.e.,childrenunderdilatationofSGS
in a period >30 days fromthe onset of symptoms of SGS
and/or from diagnosis, and the group of acute SGS, i.e.,
thosechildrendilatedintheperiod≤30daysfromtheonset
ofsymptomsorfromdiagnosisofSGS.
The degreeofsubglotticstenosis wasdeterminedusing
theclassificationofMyerandCotton,6whichwasobtained
afterbronchoscopy usinga 0-degreerigid endoscopewith
a diameter ranging from 2.7mm to 4mm. Retrograde
endoscopywithMachida® 3.2mmflexible fiberendoscope
was also performed in patients undergoing tracheostomy
whenitwasnotpossibletopasstherigidendoscopethrough
thestricture,thusallowingabetterstagingofthedegree
ofacquiredSGS.
Thedilatationswerealwaysperformedwiththepatient
under general anesthesia, spontaneous ventilation, and
intermittent apnea during balloon inflation, as needed.
Vascular balloons of three different brands (Acclarent®,
Boston®,andE.Tamussino®)wereused,alwayswithalength
of20---30mm.Thediametersoftheballoonsvaried
accord-ingtothechild’sage.Generally,theoutsidediameterofthe
most suitable endotracheal tube was considered for each
child,addingapproximately2mmtodeterminethe
diame-teroftheballoon.Thetimeandnumberofinflationsvaried
according tosizeof the airway, aswellas thepulmonary
reserve of the child and/or the perception of
supraglot-tic/glottic edema secondary to dilatation. Generally, the
maintenance time of the inflated balloon did not exceed
1.5min,andtheinflationswererepeatedthreetimes.The
inflationpressureoftheballoonsrangedfrom3to15mmHg
withaprogressivetendencyfortheuseofhigherpressures
in the last year, after analyzing reports and personal
Figure1 Balloonduringdilatation.Childduringballoon laryn-goplasty.
communicationsfromothercolleagueswithrenowned
expe-rienceinthesubject,especiallyinthemostextensiveand
chronicstenoses.Thetimeelapsedbetweendilatation
pro-ceduresranged from15 to60 days,due toavailabilityof
surgicaltimeandpossibleclinicalcomplications,orthelack
offavorableconditionsforgeneralanesthesia.
All pre- and post-dilatation endoscopies were
docu-mented, aswell as a detailed description in the medical
record regarding the post-procedural outcomes and the
occurrenceofcomplications.
Treatmentwasconsideredsuccessfulinpatientswho,in
thestudyperiod,weredecannulatedand/orhadnofurther
signsorsymptomsofdiscomfort,eveninthefaceofresidual
stenosis.
To correlate the predictors of successful outcomes,
a statistical analysis was performed using nonparametric
Mann---WhitneyUandFisher’sexacttests,withasignificance
levelsetat0.05.
Results
Atotalof37childrenwhounderwentballoonlaryngoplasty
(Fig. 1) were included in the study; 24 had chronic SGS
(Fig.2)and13 hadacuteSGS(Fig.3).Themeanage was
22.5months(range:1monthto11years)(Table1).Twoof
24patientswithchronicSGSand10of13patientswithacute
SGSwerenottracheostomized.AstothedegreeofSGS,two
patientshadgradeI,fivehadgradeII,and30hadgradeIII.
Thenumberofdilatationsrangedfromonetofive,witha
meanof2.5proceduresperpatient.Threepatientshad
dys-phagiaasacomplicationimmediatelyaftertheprocedure;
thedysphagiawastransient, resolvingin lessthan 24h in
twocases;inonecase,itwaspersistent,requiringtheuse
ofanasoenterictubeforaperiodofthreeweeks.
Inthegroup ofchronic stenoses,themeandurationof
thestenosiswas22months(minimumofthreemonths,and
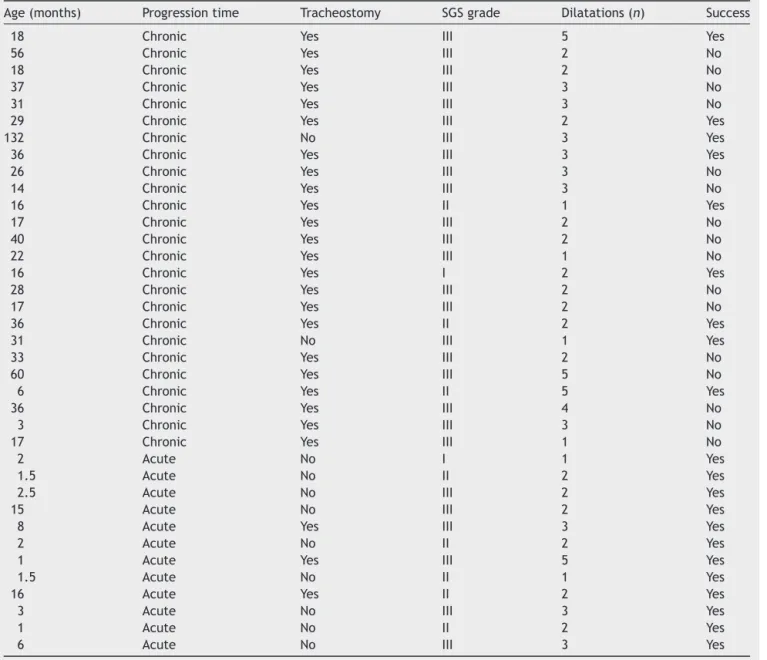
Table1 Descriptionofcaseswithdataregardingage,durationofthedisease,presenceoftracheostomy,degreeofstenosis, numberofdilatations,andtherapeuticsuccess.
Age(months) Progressiontime Tracheostomy SGSgrade Dilatations(n) Success
18 Chronic Yes III 5 Yes
56 Chronic Yes III 2 No
18 Chronic Yes III 2 No
37 Chronic Yes III 3 No
31 Chronic Yes III 3 No
29 Chronic Yes III 2 Yes
132 Chronic No III 3 Yes
36 Chronic Yes III 3 Yes
26 Chronic Yes III 3 No
14 Chronic Yes III 3 No
16 Chronic Yes II 1 Yes
17 Chronic Yes III 2 No
40 Chronic Yes III 2 No
22 Chronic Yes III 1 No
16 Chronic Yes I 2 Yes
28 Chronic Yes III 2 No
17 Chronic Yes III 2 No
36 Chronic Yes II 2 Yes
31 Chronic No III 1 Yes
33 Chronic Yes III 2 No
60 Chronic Yes III 5 No
6 Chronic Yes II 5 Yes
36 Chronic Yes III 4 No
3 Chronic Yes III 3 No
17 Chronic Yes III 1 No
2 Acute No I 1 Yes
1.5 Acute No II 2 Yes
2.5 Acute No III 2 Yes
15 Acute No III 2 Yes
8 Acute Yes III 3 Yes
2 Acute No II 2 Yes
1 Acute Yes III 5 Yes
1.5 Acute No II 1 Yes
16 Acute Yes II 2 Yes
3 Acute No III 3 Yes
1 Acute No II 2 Yes
6 Acute No III 3 Yes
Thesuccessratewas100%and32%foracuteandchronic stenoses,respectively(Fig.4).
Theminimumfollow-uptimewasthreemonths,witha
maximumof12months.
Correlating the patient’s age with the success of the
balloonlaryngoplasty technique,it wasobserved thatthe
youngerthechild,thehigherthesuccessrate(Fig.5).
Correlatingthepresenceoftracheostomyatthetimeof
theprocedurewithproceduralsuccess,itwasobservedthat
non-tracheostomizedpatientshadhigherchancesofsuccess
withtheprocedure(Fig.6).
Correlatingthedegreeofsubglotticstenosisand
proce-duralsuccess,itwasobservedthatthehigherthedegreeof
thestenosis,thegreaterthechancesoffailure(Fig.7).
Correlating the number of dilatations and the success
ofthetechnique,nostatisticallysignificantcorrelationwas
observed(Fig.8).
Correlatingtheprogressiontimeofsubglotticstenosisin
bothgroups,itwasfoundthatgroup1(children>30daysof
stenosis[chronicSGS])hadhigherchancesoffailure(Fig.4).
Inthegroupofchronicstenoses,nocorrelationbetween
progression, time of the stenosis, and success rate was
observed.
Discussion
Usually,thetreatmentofacquiredSGSinpediatricpatients
is a distressing and painful event both for patients and
their relatives. Inacute cases,the patientis hospitalized
andintubated,failingsuccessivelyinattemptsfor
extuba-tion;orsometimesthechildisextubated,butinastateof
respiratoryfailure.In chroniccases,thechild alreadyhas
Figure2 Chronicsubglotticstenosis.Childwithchronicgrade IIISGS,pre-dilatation.
oflaryngitisorasthma.Thesearechildrenwhorepeatedly
seek health services, often without receiving information
or referral toaprofessionalin apositiontomake a
diag-nosis and establish a sound treatment. The presence of
theotorhinolaryngologisttrainedintheevaluationof
pedi-atric airways and working next to pediatric and neonatal
ICUs is critical to change this scenario. Thus, it will be
possibletoestablishearlydiagnosesandproceduresaimed
at preventing the occurrence of acquired SGS. The
suc-cessofdilatation foracutestenoses,asshownin thisand
otherstudies,7---9confirmsthisneed.Unfortunately,the
pro-cedure of tracheostomyhas been theonly alternative for
thesecases,intheabsenceofaproperevaluation.Despite
the immediate resolution of respiratory failure, the
nec-essary care, mainly in the case of suckling infants with
tracheostomy,isconsiderable,causingmuchanguish,fear,
andsociallimitationbothforcaregiversandfor thechild.
However,theriskoftracheostomytube obstructionandof
Figure3 Acutesubglotticstenosis.ChildwithacutegradeIII SGS,pre-dilatation.
Chronic Acute
Failure Successful 20
15
10
5
0
Figure 4 Correlation of patients in group 1 (chronic) and group2(acute)withthechancesofsuccesswithballoon laryn-goplasty.
Successful Failure
40
30
20
10
0
Age (months)
Figure5 Correlationbetweenpatientageandsuccessof bal-loonlaryngoplasty.
Tracheostomy+ Tracheostomy–
Failure Successful 20
15
10
5
0
Patients (n)
1
Successful Failure 20
15
10
5
0
2 3
0 0
7
11 16
2
G test: Independence
Figure7 Correlationbetweenthedegreeofstenosis accord-ing to Myer---Cotton and failures of balloon laryngoplasty (p=0.0015).
death cannot be ignored --- inside and especially outside
thehospital.Thus,aswasdemonstratedinthisstudy,
bal-loon laryngoplasty, besides being an excellent option for
childrenwithacuteSGS,couldpreventalarge numberof
tracheostomieswhich are unfortunately performed in the
pediatricpopulation,particularlyduringandafter
hospital-izationsinICUs.
Evenafterperformingatracheotomy,theinflammation
generated by the tracheal tube will heal, and
consider-ing that the respiratory condition was stabilized by the
1 10
8
6
4
0 2
3 2
4
5 7
6
G test: Independence
9
1 1
0
4 5
1 2
Successful Failure
Figure8 Correlationbetweenthenumberofdilatationsand balloonlaryngoplastysuccess.Nostatisticalsignificance.
tracheostomy, often the resultingscarringor stenosis will
beignoredforweeks,months,orevenyears.Insuchcases,
thestenosiswillbediagnosedlate.Inthesechroniccases,
thetherapeuticalternativesmayinvolveendoscopic
proce-duresorexternalsurgeries.Inthepresentstudy,itwasfound
thateveninchroniccases,thesubglotticstenosesmaybe
amenabletorelativelylessinvasivetreatments,suchas
bal-loon dilatation, although in thisstudy the success rate in
childrenwithchronicSGSwasonly32%.Theresultsreported
in theliterature for balloon laryngoplastydo not
discrim-inate among chronic and acute cases, but some authors8
suggest that the results would not be good.According to
thepresentresults,inchronicstenosiscasesthereseemsto
bearelationshipbetweentimeofstenosisprogressionand
therapeuticsuccesswithballoonlaryngoplasty.Thisseems
to be more related to the degree of stenosis and to the
characteristicsofthescar.Thesedatadiffersomewhatfrom
thosereportedbyWhighametal.10In2012,theseauthors10
suggestedthatfailureintheprimarytreatmentofstenoses
withballoondilatation isrelatedtoothercomorbiditiesin
theairways,andfoundnorelationshipbetweentherapeutic
successandageoftheirchildren,degreeofstenosis,andits
characteristics(softorfibrous),divergingfromthefindings
ofthepresentstudy,whichobservedbettersuccessratesfor
youngerchildrenandthosewithlowerdegreesofstenosis.
Thinorlaminarscarsappeartobemorepronetogoodresults
withballoon dilatation. This makessense,sincethe thick
andfibroticcartilaginousframeworkofthelarynxcannotbe
dilated.However,thisisonlyanimpressionoftheauthors,
andthisfindinghasnotbeenmeasuredinthepresentstudy.
In this study, the absence of prior tracheostomy had
sig-nificantcorrelationwiththesuccessoftheprocedure.This
findingmayreflectthegeneralhealthstateofthesechildren
who, despite showing severe stenosis, had no significant
comorbidities,inagreementwithliteraturereports.10
Although in this study thefailure of balloon dilatation
occurred in 68% of children treated for chronic SGS, it is
believedthatevenincaseswherethereisnopossibilityof
stenosis anddecannulation, theincrease ofthesubglottic
diameteratthecostofmucosalscartissuedilatationoften
allows vocalization. The possibility of vocal emission and
communicationsignificantlyimpactthequalityoflifeofthe
patientandof theirrelatives,whooften musttowaitfor
thecontrolofcomorbidities---which cantakemonthsand
sometimesyears---forprogramminganopenreconstruction
surgery.
Theprincipalattractivefeatureofballoonlaryngoplasty
istherelativeeaseofitsimplementationandthepossibility
ofitsuseeveninseverestenosis,consideringthediminutive
diameteroftheballoon,whichdifferentiatesitfromother
forms of dilatation. This techniquealso does not exclude
thepossibilityof anexternalreconstructivesurgeryinthe
caseoffailure;norwasitshowntocauseanincreaseinthe
scarred area,hindering subsequent treatments that were
performedin fivechildreninthisgroup.Thesuccessrates
ofballoonlaryngoplastyforprimarytreatmentofacquired
SGSvariesbetween60%10and100%11intheliterature.8,12---14
Recently,thegroupofBlanchardetal.13suggestedeventhe
primary treatment of congenital subglottic stenoses with
thismethod.
However, the dilatation of non-tracheostomized
with the glottis obstructed by a balloon can lead to
serious complications, such as pulmonary edema.
There-fore, it is essential to involve the surgical team with
the anesthesia team, so that spontaneous breathing and
apneas are coordinated during the procedure ---
espe-ciallyinnon-tracheostomizedchildren.Somechildrenhave
extremely reactive airways, and edema of the
supraglot-ticregion mayresult in transient cough anddysphagia as
clinical implications. Obstructiveconditions,secondary to
dilatation,werenotfoundinthisgroup,evenamong
non-tracheostomizedchildren.Transientdysphagiawasobserved
in only three children, representing an 8% incidence of
complications.Thiswasconsideredaminorcomplication,as
theseweretransientepisodes.Therewerenootherevents
orcomplicationsrelatedtoballoonlaryngoplasty.
Currently,the maindifficulties inlaryngoplastyballoon
proceduresrelateprincipallytothelackofstandardization,
mainlywithregardtothenumberofdilatations.Inthe
liter-ature,thereisnostandardizationwithrespecttodilatation
pressure,dilatationtime,intervalbetweendilatations,and
useofmoldsandoftopicalorinjectablemedications.The
authors’ impression is that the inflation pressure and the
duration of balloon inflation should be adjusted to each
patient,dependingontheobservationof reactiveedema.
Theballoonsusedhaveanindicationofmaximumdiameter
withrespecttoacertainpressure;therefore,toexceedthe
prescribedpressuredoesnotincreasetheexpansionofthe
airway,butonlyincreasestheriskofballoonbreakage,
ren-deringnewinflationsimpossible.Usually,theauthorsagree
that theballoon shouldbeinflated at least twice ineach
procedure.
An extremelyinterestingfindingobservedin thisseries
wasthelackofcorrelationbetweensuccessrateand
num-berofdilatations.Considerablecommonsenseiscalledfor
inordertoavoidperformingunnecessaryproceduresandthe
creationoffalseexpectationsoftherapeuticsuccessforthe
childandhis/herfamily.Videodocumentationandserial
cal-ibrationoftheairwaywithtrachealtubesatthebeginning
andendofeachprocedureprovidealittlemoreobjectivity
tothefollow-upofthesecases.Furthermore,theyallowthe
surgeontoactuallymaterializethebenefitsofintervention,
andtodeterminewhentostopthistreatmentandelectthe
reconstructivesurgerymostappropriateforthecase.
Conclusion
Balloonlaryngoplastycanbeconsideredasafirst-line
treat-mentin SGS,both acuteandchronic. Inacutecases, this
procedure was100% successful.In chronic cases the
ben-efits,evenpartial,were freeof significantcomplications,
withoutprejudicetofuturereconstructivesurgeries.
Thepredictivefactorsofsuccessinthisstudywere:
pres-enceofacutestenosis,dilatationatanearlyage,dilatation
intheabsenceofpriortracheostomy,andlesssevere(grade
IandII)stenoses.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.GouldJB,BenitzWE,LiuH.Mortalityandtimetodeathinvery lowbirthweightinfants:California,1987and1993.Pediatrics. 2000;105:E37.
2.FragaJC,deSouzaJCK,KruelJ.Pediatrictracheostomy.J Pedi-atr(RioJ).2009;85:97---103.
3.Lang M,Brietzke SE.A systematic review and meta-analysis ofendoscopicballoondilationofpediatricsubglotticstenosis. OtolaryngolHeadNeckSurg.2014;150:174---9.
4.Monnier P, editor. Pediatric airway surgery. Heidelberg: Springer;2010.
5.HebraA,PowellDD,SmithCD,OthersenHB.Balloon tracheo-plastyinchildren: resultsofa 15-yearexperience.JPediatr Surg.1991;26:95761.
6.MyerCM,O’ConnorDM,CottonRT.Proposedgradingsystemfor subglotticstenosisbasedonendotrachealtubesizes.AnnOtol RhinolLaryngol.1994;103:319---23.
7.SchweigerC,SmithMM,KuhlG,ManicaD,MarosticaPJC. Bal-loonlaryngoplasty inchildrenwithacute subglotticstenosis: experienceofatertiary-carehospital.BrazJOtorhinolaryngol. 2011;77:711---5.
8.DurdenF,SobolSE.Balloonlaryngoplastyasaprimary treat-mentforsubglotticstenosis.ArchOtolaryngolHeadNeckSurg. 2007;133:772---5.
9.Avelino M,Fernandes E. Balloon laryngoplasty for subglottic stenosis caused byorotracheal intubation at a tertiary care pediatrichospital.IntArchOtorhinolaryngol.2013[Epubahead ofprint].
10.WhighamAS,HowellR,ChoiS,Pe˜naM,ZalzalG,PreciadoD. Outcomesofballoondilationinpediatric subglotticstenosis. AnnOtolRhinolLaryngol.2012;121:442---8.
11.GuariscoJL,YangCJ.Balloondilationinthemanagementof severeairwaystenosis inchildrenand adolescents.JPediatr Surg.2013;48:1676---81.
12.Hautefort C, Teissier N, Viala P, Van Den Abbeele T. Bal-loondilationlaryngoplastyforsubglotticstenosisinchildren: eight years’ experience. Arch Otolaryngol Head Neck Surg. 2012;138:235---40.
13.Blanchard M, Leboulanger N, Thierry B, Blancal J-P, Glynn F,DenoyelleF,et al. Managementspecificities ofcongenital laryngealstenosis:externalandendoscopicapproaches. Laryn-goscope.2013[Epubaheadofprint].
14.Collins WO, Kalantar N, Rohrs HB, Silva RC. The effects of balloon dilation laryngoplasty in children withcongenital heart disease. Arch Otolaryngol Head Neck Surg. 2012;138: 1136---40.