SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Infection
rate
in
adult
patients
with
open
fractures
treated
at
the
emergency
hospital
and
at
the
ULBRA
university
hospital
in
Canoas,
Rio
Grande
do
Sul,
Brazil
夽
Marcelo
Teodoro
Ezequiel
Guerra,
Fernando
Machado
Gregio
∗,
Adriane
Bernardi,
Cyntia
Cordeiro
de
Castro
UniversidadeLuteranadoBrasil(Ulbra),HospitalUniversitário,Canoas,RS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received26August2016 Accepted1September2016 Availableonline25August2017
Keywords:
Openfractures Infection Emergencies
a
b
s
t
r
a
c
t
Objective:Toidentifytheinfectionrateinadultpatientswithopenfracturestreatedattwo tertiaryhospitalsinthecityofCanoas,RioGrandedoSul,Brazil.
Methods:ThisquantitativedescriptivestudywasconductedatHospitaldeProntoSocorro deCanoas.Eligibleparticipantswereadultsaged18–60yearswithopenfractureswhowere admittedtotheorthopedictraumaservicefromJanuarytoMay2014andfollowed-upfor oneyear.
Results:Atotalof133patientswithopenfractureswereincluded;mostweremen(92.48%), withameanageof36years.TherewasapredominanceofGustilo-AndersontypeIII frac-tures.Theinfection ratewas18.80%, beingmorefrequent inGustilo-Andersontype III fractures(72.00%).ThemostcommonlyobservedbacteriawereStaphylococcusaureusand
Enterobacteraerogenes.
Conclusion:Theinfectionrateinopenfracturesofpatientsinitiallytreatedattheemergency departmentofHPSCwas18.8%.TheinfectionsoccurredpredominantlyinGustilo-Anderson typeIIIfractures.ThebacteriawiththehighestincidenceininfectionswereStaphylococcus aureusandEnterobacteraerogenes.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
PaperdevelopedatUniversidadeLuteranadoBrasil(Ulbra),HospitalUniversitário,DepartamentodeOrtopediaeTraumatologia, Canoas,RS,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](F.M.Gregio). http://dx.doi.org/10.1016/j.rboe.2017.08.012
Taxa
de
infecc¸ão
em
pacientes
adultos
com
fratura
exposta
atendidos
no
hospital
de
pronto
socorro
e
no
hospital
universitário
Ulbra
do
município
de
Canoas,
Rio
Grande
do
Sul
Palavras-chave:
Fraturasexpostas Infecc¸ão
Emergências
r
e
s
u
m
o
Objetivo: Identificarataxadeinfecc¸ãoempacientesadultoscomfraturaexpostaatendidos emdoishospitaisterciáriosnomunicípiodeCanoas,RioGrandedoSul.
Métodos: Estudoquantitativodescritivofeitono HospitaldePronto Socorrode Canoas (HPSC).Foramelegíveisospacientesentre18e60anosinternadoscomfraturaexposta nosetordetraumatologiaeortopediadaemergênciadoHPSC,dejaneiroamaiode2014,e queforamacompanhadosporumano.
Resultados: Foramincluídos133pacientescomfraturaexposta,amaioriadosexo mas-culino(92,48%),commédiade36anos.HouvepredomíniodefraturasdotipoIIIdeGustilo eAnderson.Ataxadeinfecc¸ãofoide18,80%,maisfrequenteemfraturasdotipoIIIde GustiloeAnderson(72%).Asbactériasmaisfrequentementeidentificadasnasinfecc¸ões foramStaphylococcusaureuseEnterobacteraerogenes.
Conclusão: Ataxadeinfecc¸ãoemfraturasexpostasdepacientesatendidosinicialmentena emergênciadoHPSCfoide18,80%.Asinfecc¸õesocorrerampredominantementeemfraturas dotipoIIIdeGustiloeAnderson.Asbactériascommaiorincidêncianasinfecc¸õesforam
StaphylococcusaureuseEnterobacteraerogenes.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Traumaticpathologieshaveanincreasingincidencebothin diagnosesand hospitaladmissions,1 duetothe increasein
violenceandcaraccidents,maincausesofthesetraumasin adults.Asaconsequence,thereisanincreaseinemergency expenses,whichisusuallymoreonerousthanmost conven-tionalprocedures.2,3
Openfractures,alsoknownascompoundfractures,areone ofthe consequencesoftrauma.Insuchcases,the fracture segmentscommunicatewiththecontaminatedenvironment throughskin4andadjacentsofttissues,5nomatterhowsmall
thesofttissuelesionis.6Theopenfracturemaybeanisolated
injury,orcanoccurtogetherwithaseriesofmultiplewounds,4
andisusuallyassociatedwithalargenumberofcomorbidities. Itisestimatedthattheincidenceofopenfracturesoflong bones is 11.5 cases per 100,000 people per annum.7 Open
fracturesaremorecommoninmenandhaveabimodalage distribution,withthetibiabeingthemostaffectedbone.6
Thepresenceofanopenfractureresultsinarangeof clin-icalsituations, amongwhich the mostcommon and most seriouscomplicationisinfection.8,9 Basedonthecriteriaof
theBrazilianNational Health SurveillanceAgency (Anvisa), whichinvolveclinical,histologicalandimaging characteris-tics, the presence of one of the altered criteria is already determinantforthediagnosisofinfection.10Theprevalence
ofinfectioniscloselyrelatedtotheseverityofthepatient’s fracture,11,12thatis,accordingtotheclassificationbyGustilo
andAnderson,13thehigherthe lesiontype,the greaterthe
likelihoodofinfection.14
Duetothelargenumberofvictimsofopenfractures,and totheircomplexity,itisnecessarytostudytheratesofopen
fractures intertiary hospitalstoallowbetter planning and careorganizationforthesepatients.Thus,thisstudyaimed toidentifytheinfectionrateinadultpatientswithopen frac-turestreatedattwohospitalsinthecityofCanoas,stateofRio GrandedoSul.
Material
and
methods
Thisisadescriptivestudy,basedon consecutivesampling, performedinanemergencyhospitalandinanothertertiary hospitalinthe city ofCanoas. Thestudy wasapprovedby the Research Ethics Committeeofbothinstitutions (proto-col#447594.15.2.0000.5349).Theanonymityoftheparticipants wasassured,aswellastheuseofdataonlybythemainauthor, exclusivelyforstudypurposes.
Allpatientsbetween18and60yearsofageattendedand admittedwithopenfracturesbythetraumaandorthopedics teaminthehospitalemergencyroom,fromJanuary1toMay 24,2014,wereeligibleforthestudyandwerefollowedupfor oneyearintheinstitutions.Thepatientswho couldnotbe evaluatedforaperiodofoneyear,fromthedateofadmission, andthepatientswhowerenotadmittedbythetraumatology andorthopedicsteamoftheinstitutionwereexcluded.
Patientdatawerecollectedfromthemedicalrecordsfrom JulytoAugust2015bythemainauthorwithaspecificform. Thepatientswereevaluatedbyage,gender,typeoffracture accordingtoGustiloandAndersonclassification,13andforthe
presenceofinfectionattheopenfracture siteaccordingto Anvisa’scriteria10andbacteriologicalprofile.
Table1–Relationbetweengenderandtypeoffracture,accordingtotheGustiloandAndersonclassification.
Type
I II IIIA IIIB IIIC
Gender n % n % n % n % n %
Female 1 3.10 1 2.60 3 8.10 3 17.60 2 25.00
Male 31 96.90 38 97.40 34 91.90 14 82.40 6 75.00
Fisher’sexacttest,p<0.065.
questionnaires;the consistency and coherence of the data wereanalyzed.DatawerethenstoredinadatabaseusingExcel software.
Quantitative variables were presented by mean and standarddeviation(SD)andcategoricalvariablesbyabsolute (n)andrelative(%)frequencies.Theassociationbetweenthe categoricalvariableswasevaluatedusingFisher’sexacttest, anappropriatemethodforthis evaluationwhenmorethan 25%ofthevaluesarebelowthelevelofsignificance(p<0.05). Forthevariables withnormaldistribution,the meanswere comparedwiththevarianceanalysis(Anova).Thestatistical analysiswasperformedwiththeStatisticalPackagefortheSocial Sciences(SPSS)software,version18.0(SPSSInc.,IBMCompany, Chicago,IL,USA)andthelevelofsignificanceusedwas5% (p<0.05).
Results
FromJanuary1toMay24,2014,519patientswereattended andadmittedbythetraumatologyandorthopedicsteamof theemergencyhospital,withameanof1.08caseperday.Of these,154patientshadanopenfractureandwereanalyzed forinclusioninthestudy.Twenty-onepatientswereexcluded becausetheydidnothaveaone-yearfollow-up,countingfrom thedayofadmission,whichresultedin133patientswithan openfractureincludedinthestudy.
Themeanageofthepatientswithopenfractureswas36 years(SD:12.60years)andmostofthemweremale(n=123; 92.48%).Themeanagewas35.50years(SD:12.45years)among males,and41.60years(SD:14.50years)amongfemales.
ThemostprevalenttypeoffracturewastypeIII, account-ingfor46.70%ofallcases(62patients).Ofthese,59.70%(37 patients)weretypeIIIA,27.40%(17)IIIBand12.90%(eight)IIIC. TypeIwastheleastprevalent,with24.70%(32),followedby typeII,with29.30%(39).
TypeIIICfractureswerethemostfrequentamongfemales (25%),whiletypeIIfractureswerethemostfrequentamong males(97.40%).Therewasnoassociationbetweengenderand typeoffracture(p<0.065)(Table1).
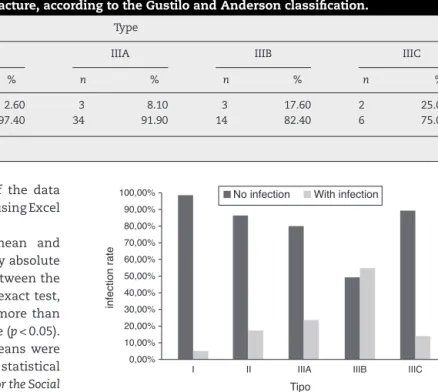
Twenty-five patients(18.80%) developedan infection.Of these,one(4%)wasclassifiedastypeIfracture,six(24%)with typeIIfractures,and 18 (72%)withtypeIIIfractures. Frac-turesclassifiedastypeIIIBpresentedthehighestinfectionrate (36%),whilethoseclassifiedastypeIhadthelowestinfection rate(4%).Therewasasignificantassociationbetweenthetype offractureandtheoccurrenceofinfection(p<0.001)(Fig.1).
Twenty-sevenpositivecultureswerefoundin17infected patients (68%). In these cultures, 11 microorganisms were
100,00%
90,00%
80,00%
70,00%
60,00%
50,00%
40,00%
infection rate 30,00%
20,00%
10,00%
0,00%
I II IIIA IIIB IIIC
Tipo
No infection With infection
Fig.1–Relationbetweeninfectionrateandtypeoffracture, accordingtotheGustiloandAndersonclassification. Fisher’sexacttest,p<0.001.
identified,describedinTable2.Ofthese,33.30%were gram-positivebacteria,and66.70%weregram-negativebacteria.
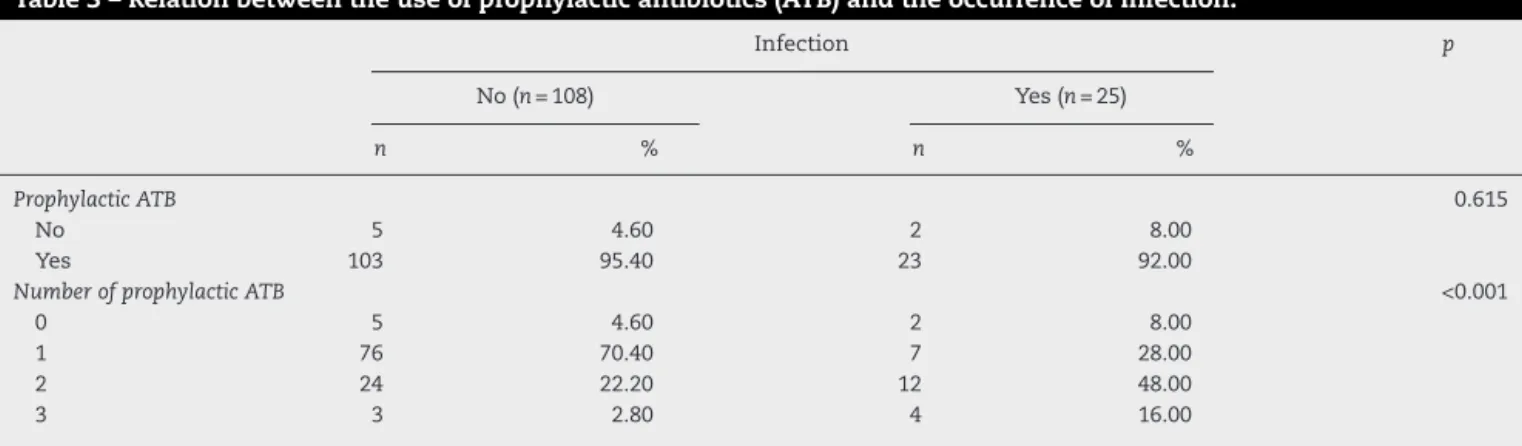
Therelationshipbetweentheuse ofprophylactic antibi-oticsandtheoccurrenceofinfectionispresentedinTable3. Twenty-eightpatientswithtypeIIIfracturesusedtwoormore antibiotics,while13patientswithtypeIorIIfracturesused twoormoreprophylacticantibiotics.
Discussion
Thepresentstudyinvestigatedtheassociationbetweenthe incidence of infections and open fractures in two tertiary hospitalsinthecityofCanoas,inthesouthernregionofthe country.ItwasalsoevidentthelackofresearchinBrazilian
Table2–Prevalenceofmicroorganisms.
Bacteria n %
Enterobacteraerogenes 5 18.50
Staphylococcusaureus 5 18.50
Acinetobactersp. 3 11.10
Enterococcussp. 3 11.10
Pseudomonasaeruginosa 3 11.10
Mixedflora 2 7.40
Serratiasp. 2 7.40
Grambacillus–non-fermenting 1 3.70
Enterobactercloacae 1 3.70
Escherichiacoli 1 3.70
Table3–Relationbetweentheuseofprophylacticantibiotics(ATB)andtheoccurrenceofinfection.
Infection p
No(n=108) Yes(n=25)
n % n %
ProphylacticATB 0.615
No 5 4.60 2 8.00
Yes 103 95.40 23 92.00
NumberofprophylacticATB <0.001
0 5 4.60 2 8.00
1 76 70.40 7 28.00
2 24 22.20 12 48.00
3 3 2.80 4 16.00
literature. An infection rate of 18.80% was found in open fractures ofpatientsseen initially inthe emergency room, and followed up for a year in the hospitalsin which the studieswere conducted.Infectionsoccurred predominantly inGustiloandAndersontypeIIIfractures.
Thestudyhasthreelimitations.Firstly,theshortperiod, becauseonMay25,2014,aprotocolofantibioticprophylaxis andantibiotictherapywasinstitutedintheemergencyroom, whichcouldinterferewiththeresultsoftheresearch.Thus, thestudywasinterruptedonMay24,2014.Secondly,patients withanopenfracturewhowerenotadmittedtothe hospi-tal bythe traumaand orthopedicsteam ofthe emergency roomwereexcludedfromthestudy.Thesehospitalsare refer-enceinOrthopedicsandTraumatologyfor140municipalities inthestateofRioGrandedoSul.However,somepatientshave privatehealthcareplansandprefertobecaredforin hospi-talsoftheirchoice.Inaddition,patientsfromcitiesthatare notareferenceofthemunicipalityofCanoasareoftentaken bytheEmergencyMobileCareService(SAMU)tooneofthe twohealthinstitutionstoreceivefirstcare,thentheyreturn totheirhomemunicipalityforfollow-up.Thirdly,arelevant numberofpatientswithopenfractures(n=21)wereexcluded fromthestudybecausetheyweretransferredorbecausethey lostthelinkwiththehealthinstitutions,makingit impossi-bletoanalyzethesepatientsforafullyearfromthedateof admission.
Inthe present study,mostpatients withopen fractures weremale,withameanageof36years,consistentwiththe lit-erature,whichestimatesthehighestprevalenceamongmen inthefourthdecade.6Thefemaleagegrouppresentedinthe
literatureisover60yearsofage,6differentfromthatfoundin
thepresentstudy,whichwas41.60years,mostprobablydue totheagerangestipulatedasinclusioncriterion(18–60years). TypeIIIfracturesofthe GustiloandAnderson classifica-tionwereprevalent(46.70%),datathatiscommoninprevious studiesofopenfractures.15,16Fortheotherfracturetypes,the
valuesfoundwerealsosimilartothosereportedinthe litera-ture,of15.80%fortypeI,and29.50%fortypeII.15
Theinfectionratefound(18.80%)washigherthanthe10% rate described insimilar international studies,17 but lower
thanthatreportedinnationalstudies,withrateshigherthan 20%.16TheestimatedrateofinfectionfortypeIfracturesis
0–2%,fortypeIIis2–7%,andfortypeIIIis10–25%,valueslower thanthosefoundinthepresentstudy(typeI:4%,typeII:24%, andtypeIII:72%).
Regarding themicroorganismspresent intheinfections,
StaphylococcusaureusandEnterobacteraerogeneshadthehighest incidence,whichisinagreementwiththeliterature.17In
addi-tion,therewasahigherincidenceofgram-negativeagents, whichmaybejustifiedbythepresenceofthesebacteriainthe openfracturesinfections,17,18andbytheprevalenceof
bacte-riaineachinstitution.17ThestudybyCollingeetal.,19inwhich
onlyintravenouscefazolinwasusedinthepatients,showed thattimewasdirectlyassociatedwiththeinfectionrate,but theamountofantibioticsdidnotpresentastatistically signif-icantimpactontheinfectionrate.
Conclusion
Thepresentstudyaimedtoidentifytherateofinfectionin open fractures in two tertiary hospitals, HPSC and HU, by meansofthevariablesgender,age,severityofopenfractures, infectionandinfectiousagents.Therateofinfectioninopen fracturesfoundinpatientsadmittedthroughtheHPSC emer-gency was 18.80%, and the mostfrequent microorganisms wereEnterobacteraerogenesandStaphylococcusaureus.Itshould benotedthattheinfectionisnotdirectlylinkedtothenumber ofantibioticsused.Inviewofthedataobtained,the impor-tanceofthefollow-upofthestudiesisemphasized,sothat therecanbeaconstantimprovementinpatientcare.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.deCastroRR,RibeiroNF,deAndradeAM,JaquesBD. Orthopedicsnursingpatients’profileofapublichospitalin Salvador-Bahia.ActaOrtopBras.2013;21(4):191–4.
2.MinayoMC.ViolênciaeSaúde.RiodeJaneiro:Fiocruz;2006. 3.MalvestioMA,SousaRMC.Sobrevivênciaapósacidentesde trânsito:impactodasvariáveisclínicasepré-hospitalares. RevSaúdePública.2008;42(4):639–47.
4.HoffWS,BonadiesJA,CachechoR,DorlacWC.EastPractice ManagementGuidelinesWorkGroup:updatetopractice managementguidelinesforprophylacticantibioticusein openfractures.JTrauma.2011;70(3):751–4.
epidemiológicoeprospectivo.ActaOrtopBras. 2009;17(6):326–30.
6. GumJL,SelignoD.Updateonthemanagementofopen fractures.AmAcadOrthopaedicSurgeonsWebsite: OrthopaedicKnowledgeOnlineJ.2012;10(9).Availablein: www.aaos.org/jaaos/.
7. Court-BrownCM,RimmerS,PrakashU,McQueenMM.The epidemiologyofopenlongbonefractures.Injury.
1998;29(7):529–34.
8. OkikeK,BhattacharyyaT.Trendsinthemanagementofopen fractures.Acriticalanalysis.JBoneJointSurgAm.
2006;88(12):2739–48.
9. PatzakisMJ,WilkinsJ,MooreTM.Useofantibioticsinopen tibialfractures.ClinOrthopRelatRes.1983;(178):31–5. 10.AgênciaNacionaldeVigilânciaSanitária.Critérios
diagnósticosdeInfecc¸õesrelacionadasàassistênciaàsaúde. Brasilia,2013.Availablein:http://www20.anvisa.gov.br/ segurancadopaciente/images/documentos/livros/Livro2-CriteriosDiagnosticosIRASaude.pdf.
11.SungaranJ,HarrisI,MouradM.Theeffectoftimetotheatre oninfectionrateforopentibiafractures.ANZJSurg. 2007;77(10):886–8.
12.BartonCA,McMillianWD,CrookesBA,OslerT,BartlettCS3rd.
CompliancewiththeEasternAssociationfortheSurgeryof Traumaguidelinesforprophylacticantibioticsafteropen extremityfracture.IntJCritIllnInjSci.2012;2(2):57–62.
13.GustiloRB,AndersonJT.Preventionofinfectioninthe treatmentofonethousandandtwenty-fiveopenfracturesof longbones:retrospectiveandprospectiveanalyses.JBone JointSurgAm.1976;58(4):453–8.
14.PatzakisMJ,WilkinsJ.Factorsinfluencinginfectionratein openfracturewounds.ClinOrthopRelatRes.1989; (243):36–40.
15.MatosMA,NascimentoJM,SilvaBVP.Estudoclínico
demográficodasfraturasexpostascausadasporacidentesde motocicleta.ActaOrtopBras.2014;22(4):214–8.
16.MüllerSS,SadenbergT,PereiraGJC,SadatsuneT,KimuraEE, NovelliFilhoJLV.Estudoepidemiológico,clínicoe
microbiológicoprospectivodepacientesportadoresde fraturasexpostasatendidosemhospitaluniversitário.Acta OrtopBras.2003;5:158–69.
17.ChenAF,SchreiberVM,WashingtonW,RaoN,EvansAR. Whatistherateofmethicillin-resistantStaphylococcusaureus andGram-negativeinfectionsinopenfractures?ClinOrthop RelatRes.2013;471(10):3135–40.
18.GoldmanL,AusielloD.CecilMedicina.RiodeJaneiro: Elsevier;2009.Traduc¸ãoAdrianaPittelaSudré. 19.CollingeCA,McWilliam-RossK,KellyKC,DombroskiD.