REVISTA
PAULISTA
DE
PEDIATRIA
www.rpped.com.br
ORIGINAL
ARTICLE
Phase
angle
and
World
Health
Organization
criteria
for
the
assessment
of
nutritional
status
in
children
with
osteogenesis
imperfecta
Vicky
Nogueira
Pileggi,
Antonio
Rodolpho
Hakime
Scalize,
José
Simon
Camelo
Junior
∗FaculdadedeMedicinadeRibeirãoPreto,UniversidadedeSãoPaulo(FMRP-USP),RibeirãoPreto,SP,Brazil
Received21September2015;accepted28February2016 Availableonline14July2016
KEYWORDS
Osteogenesis imperfecta; Phaseangle; Nutritionalstatus
Abstract
Objective: Tocomparethephaseangleofpatientswithosteogenesisimperfectatreatedata tertiaryuniversityhospitalwithpatientsinacontrolgroupofhealthychildren,andtoassess thenutritionalstatusofthesepatientsthroughthebodymassindexproposedbytheWorld HealthOrganization.
Methods: Cross-sectionalstudycarriedoutinauniversityhospitalthatincludedsevenpatients with osteogenesisimperfecta andacontrol group of17 healthychildren of thesame gen-derandage.Weightandheightweremeasuredandbioelectricalimpedancewasperformed. Subsequently,thephaseanglewascalculatedbasedonresistanceandreactancevalues. Results: Thephaseangleofthegroupofchildrenwithosteogenesisimperfectawassignificantly lowerthanthatofthecontrolgroup(p<0.05).ThebodymassindexcriterionforageoftheWorld HealthOrganizationshowednodifferencebetweengroups.
Conclusions: Childrenwith osteogenesisimperfecta havea nutritionalrisk detected by the phaseangle,whichisausefultoolfornutritionalscreening.Thecalculationresultcouldhelp inthediettherapyofpatientswithosteogenesisimperfecta.
©2016SociedadedePediatriadeS˜aoPaulo.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBYlicense(http://creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Osteogênese imperfeita; Ângulodefase; Estadonutricional
ÂngulodefaseecritériosdaOrganizac¸ãoMundialdeSaúdenaavaliac¸ãodoestado
nutricionalemcrianc¸ascomosteogêneseimperfeita
Resumo
Objetivo: Compararoângulodefasedepacientescomosteogêneseimperfeitaatendidosem umhospitaluniversitárioterciáriocompacientesdeumgrupocontroledecrianc¸assaudáveis, bemcomoavaliaroestadonutricionaldessespacientespeloíndicedemassacorporalproposto pelaOrganizac¸ãoMundialdeSaúde.
∗Correspondingauthor.
E-mail:[email protected](J.S.CameloJunior).
http://dx.doi.org/10.1016/j.rppede.2016.03.010
Métodos: Estudotransversal feito em hospital universitário que incluiu setepacientes com osteogênese imperfeitaeum grupocontrolecompostopor17 crianc¸as saudáveisdemesmo sexoeidade.Foramaferidospesoeestaturaefoifeitooexamedeimpedânciabioelétrica. Posteriormente,oângulodefasefoicalculadoapartirdosvaloresderesistênciaereactância. Resultados: Oângulodefasedogrupodecrianc¸ascomosteogêneseimperfeitafoi significati-vamentemenordoqueodogrupocontrole(p<0,05).Ocritériodeíndicedemassacorporalpor idadedaOrganizac¸ãoMundialdeSaúdenãomostroudiferenc¸aentreosgrupos.
Conclusões: Crianc¸as com osteogêneseimperfeita têm um risco nutricionaldetectado pelo ângulodefase,éumaferramentaútilparatriagemnutricional.Oresultadodocálculopoderia auxiliaradietoterapiadepacientescomosteogêneseimperfeita.
©2016SociedadedePediatriadeS˜aoPaulo. PublicadoporElsevier EditoraLtda.Este ´eum artigoOpenAccesssobumalicenc¸aCCBY(http://creativecommons.org/licenses/by/4.0/).
Introduction
Osteogenesisimperfecta (OI)is an inheriteddisease char-acterizedbybone fragilityandpredispositiontofractures thatoccurwithminimalorevenintheabsenceoftrauma. Patientswith thisdisease often have low bone mass,but studies on the nutritional status of children with OI are scarce.1
In2012,astudy ofpatientswithOItypesIandIII
indi-cated the need for knowledge of bodycomposition, asit
is associated withfracture onset.2 The authors indicated
theneedtoindividualize thedietofindividualswithOIto
achievebodycompositionimprovement.
Thephaseangle(PA),obtainedfromthesecondary
analy-sisofbioelectricimpedanceforanalyzingbodycomposition
withouttheuseofanthropometricparameterscouldbeused
in patients withosteogenesis imperfecta, as
anthropome-try, especiallyheightmeasurement,is difficulttoperform
accurately.3,4 The PA is the arctangent of resistance and
reactance ratio (Xc/R), that is, it derived from the
bio-electrical impedance evaluation with the use of direct
measurements of the components of the R and Xc
vec-tor; when used as nutritional status indicator and body
cell mass (BCM), it considerably eliminates the errors of
analysisbybioelectricalimpedance.5Itsusehasbeen
rec-ommendedasanindicatorofprognosisinclinicalpractice.
In adults, positive associations have been found between
PAand survival ofHIV-positive patients,6,7 and thosewith
pulmonarycancer,8aswellassepsisandthoseundergoing
hemodialysis.9
Inthiscontext,theobjectiveofthisstudywastocompare
thePAofpatientswithosteogenesisimperfecta treatedat
HospitaldasClínicasofFaculdadedeMedicinadeRibeirão
Preto of Universidade de São Paulo (HCFRMP-USP) with a
control groupof healthy childrenand toassess the
nutri-tional status of these patients using the World Health
Organization(WHO)parametersofbodymassindexforage
(BMI/A).
Method
This was a secondary analysis of a cross-sectional study that included seven children diagnosed with osteogenesis
imperfecta (types I, III and IV) treated with pamidronate in HCFMRP-USP. All patients were followed at the Pedi-atric Endocrinology and Orthopedic Outpatient Clinic at the same hospital. These children do not represent all pediatric patients with OI treated at the hospital. They were randomly assigned to another study and were ana-lyzedseparatelyduetothediseasecomplexity.Datafrom thesepatients werecomparedwiththosefrom17healthy children of the same gender and age, which comprised the control group. The children from the control group attend the Child Care and Pediatric Outpatient Clinic of CuiabáHealth Unit in the municipality of Ribeirão Preto. This location was chosen asit cares for healthy children of the same socioeconomic level of those treated at the study tertiary hospital. They were stratified by gender and age. There was no pairing, asthey are independent groups.
Fourchildrenfromthestudygroupand12fromthe con-trolgroup signed the term of consent(aged>7 years);all patientshadtheinformedconsentformsignedbytheir par-ents/tutors.Thiswasasecondaryanalysisofthestudy on theprevalence ofmalnutritioninHCFMRP-USPcarriedout in2013.9 The study wasapproved by Institutional Review
BoardofHCFMRP-USP.
Data on weight and bioelectrical impedance were
collected according to international procedures.10 The
height/lengthwasmeasured,insomecases,onthepatients’
ownbed,astheywereunabletoremaininthestanding
posi-tion(n=6).Bodymassindex(BMI)wascalculatedforBMI/A
classificationaccordingtotheWHOcharts.11
The PA was calculated according to the formula:
˚=(Xc/R)×(180◦/),inwhich Xcis thereactancevalue,R
istheresistancevalueandpiisthemathematicalvalueof
3.1415. This conversion is performed toconvert the final
valuefromradiansintodegrees.12
Forthestatisticalanalysisofdata,thefollowingsoftware
wereused:SPSS20.0(StatisticalPackagefortheSocial
Sci-ences,WestlandsRoad,QuarryBay,HongKong,2009)andR
(RFoundationforStatisticalComputing,Universityof
Auck-land, New Zealand, 1993). Nonparametric statistics were
used,considering thatthereis nocertaintyofnormal
dis-tributionforthe anthropometricdataofpatients withOI.
TheMann---Whitneytestforindependentsampleswasused
Table1 Samplecharacteristics:demographicdataofthegroups.
Osteogenesis(n=7) Control(n=17) p-valuea
Mean Median SDb Minimum Maximum Mean Median SDb Minimum Maximum
Age(months) 104.7 123 52.42 10 158 116.1 122 39.81 10 160 0.901
Weight(kg) 24.94 16.5 20.33 6.86 68.65 33.03 31.7 10.76 10.01 48.3 0.047
Height(m) 1.06 10.8 0.26 0.65 1.51 1.37 1.4 0.2 0.78 1.67 0.011
BMI(kg/m2) 19.31 18.59 5.34 13.25 30.11 16.83 16.66 1.58 14.19 20.08 0.187
Resistance 690.6 706.3 158.3 503 965 728.6 726 110.4 503 964.33 0.455
Reactance 56.71 51 15.39 35 76 69.49 70.66 9.36 52 86 0.055
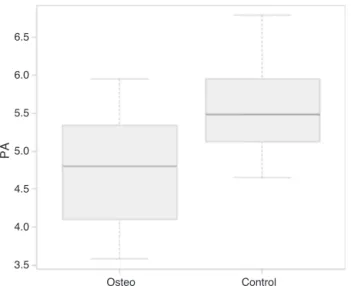
Phaseangle 4.74 4.8 0.93 3.58 5.95 5.5 5.48 0.57 4.65 6.79 0.047
aMann---WhitneyUtest. b SD=Standarddeviation.
Results
Anthropometricsandbodycompositionanalysisby bioelec-tricalimpedance,aswellasthephaseanglecalculationsare showninTable1.
AccordingtotheMann---Whitneytest,patientswith
osteo-genesis had a significantly lower classification of weight,
heightandphaseanglewhencomparedtothatofthe
con-trolgroup.Thedatadistributionregardingthephaseangle
canbeobservedinFig.1.
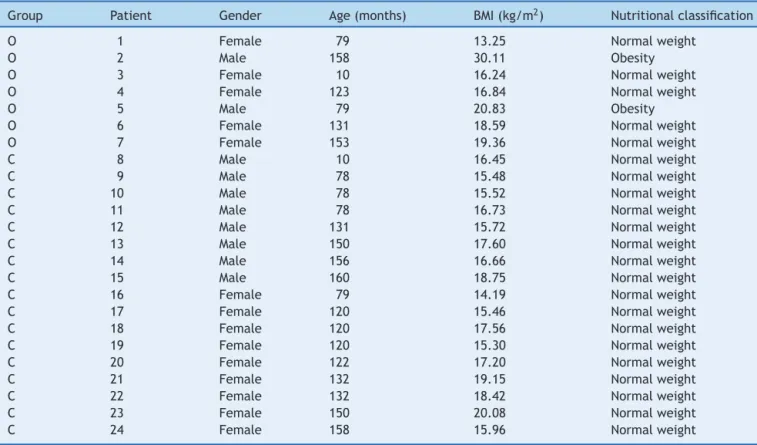
Allpatientsfromthecontrolgroupwereclassifiedas
hav-ing normal weight according to the WHO criteria. In the
groupofpatientswithosteogenesis,twowereclassifiedas
obese(BMIpercentile>97)andtheothersashavingnormal
weight(Table2).
Discussion
Accordingtoourknowledge,thisisthefirststudythatused bioelectricalimpedanceandphaseanglecalculationin pedi-atricpatients withosteogenesis imperfecta asan adjunct testtoassessnutritionalstatus.ThePAhasbeenusedasa
3.5
Osteo Control
4.0 4.5 5.0
PA
5.5 6.0 6.5
Figure1 Comparisonofthephaseangle(PA) databetween thegroups ofpatients withosteogenesisimperfecta (=osteo) andchildreninthecontrolgroup(=control).
markerofnutritionalstatusinclinicalpracticeofadults6---9
and children13 and, when associated withanthropometric
dataofweightandheightinpatientsatnutritionalrisk,it
isagoodscreeningtool.
Nagano etal. suggested the PA as a useful parameter
fornutritionalassessmentofbodycellmassinstable
pedi-atricpatients.13 Ithasbeen showntobeimportantin the
assessmentofseverityandprognosis,asitreflectsdifferent
electricalpropertiesoftissuesthatareaffectedbydisease,
nutritional status and hydration, considering it evaluates
different dimensions of nutritional status, incorporating
boththefunctionalandthemorphologicalassessment.4,13---15
Therefore,itsvalueisinfluencedbybodycellmassandthe
amountofbodyfluid.16,17
AccordingtoBarbosa-Silvaetal.,thisparameterallows
routinemonitoring througha singleor sequencedanalysis
ofthesickchild,whichcanbeinterpretedasanindicator
of fluid distribution between the intra- and
extracellu-lar spaces and integrityof all cell membranes.15 The low
value of PA suggests cell deathor decreased integrity of
cell membranes, while high values are compatible with
highervalueofreactanceandalargeamountofintactcell
membranes.14,15
In this study, the statistically lower PA values in the
OI group are probably related to lower reactance
val-ues.Althoughthereisnostatisticallysignificantdifference
regarding thereactance data (shownin Table 1),there is
aclear tendency towardlowervaluesin patientswithOI,
probablyinfluenced byosteocyte membrane integrityand
impairednutritionalstatusofthesechildren.
The anthropometric assessment of patients with OI
accordingtotheWHOcriteriamaynotbethemost
appro-priate as, insome cases,it wasnecessary toperformthe
measurementofheight/lengthwiththepatientlyingdown
inbed.Thispreventstheclassificationreliabilityandmakes
secondaryanalyses, suchasthephaseangle,bepreferred
toassessnutritionalrisk.
OIisararediseasethatcausesthebonemineraldensity
reductionandpatientsarethussusceptibletomultiple
frac-turesandconsequentdeformities, preventingan accurate
analysisofnutritionalrisk.ThemainobjectivesofOI
treat-mentaretomaximizemobilityandactivitiesofdailyliving,
aswellasreducebonepainandfragility,18without
neglect-ingnutritionalstatusimprovement,directlyassociatedwith
Table2 NutritionalstatusclassificationaccordingtotheWHOcriteriaandBMI/A.
Group Patient Gender Age(months) BMI(kg/m2) Nutritionalclassification
O 1 Female 79 13.25 Normalweight
O 2 Male 158 30.11 Obesity
O 3 Female 10 16.24 Normalweight
O 4 Female 123 16.84 Normalweight
O 5 Male 79 20.83 Obesity
O 6 Female 131 18.59 Normalweight
O 7 Female 153 19.36 Normalweight
C 8 Male 10 16.45 Normalweight
C 9 Male 78 15.48 Normalweight
C 10 Male 78 15.52 Normalweight
C 11 Male 78 16.73 Normalweight
C 12 Male 131 15.72 Normalweight
C 13 Male 150 17.60 Normalweight
C 14 Male 156 16.66 Normalweight
C 15 Male 160 18.75 Normalweight
C 16 Female 79 14.19 Normalweight
C 17 Female 120 15.46 Normalweight
C 18 Female 120 17.56 Normalweight
C 19 Female 120 15.30 Normalweight
C 20 Female 122 17.20 Normalweight
C 21 Female 132 19.15 Normalweight
C 22 Female 132 18.42 Normalweight
C 23 Female 150 20.08 Normalweight
C 24 Female 158 15.96 Normalweight
GroupO,patientswithosteogenesisimperfecta;GroupC,patientsfromthecontrolgroup.
accordingtotheWHO criteriaforBMI/Ashowedno signif-icantalterations inmostpatients. However,asmentioned before, these values might be unreliable regarding the actualheight/lengthofthechildduetodeformations,with evidentlimb shorting.Thus,anauxiliaryanalysisbecomes necessary.
Barufaldietal. alsopointedout thattheWHO criteria areless sensitive in relation tothe abilitytodetect mal-nutritionandnutritionalrisksituationsandmoresensitive todetectoverweight.Evenachievinggreaterdifferentiation regardingexcessweight,thiscriteriondoesnotdiscriminate thereasonforthechange inrelationtobodycomposition. Thus,theuseofthePAcouldbeconsideredausefuland sen-sitivetooltoclassifybodilychangesregardingmalnutrition inpatientswithOI,althoughlessspecific.19
The bone health of patients with OI can be improved
through a multidisciplinary approach, with the use of
pamidronate,adequate manualtherapies20 andnutritional
therapy.Allpatientsinthisstudywerereceivingthisdrug.
Becausebonehealthisassociatedwithadequatenutrition,
itisnecessarytobeawareofthenutritionalstatusofthese
childrenduringhospitalizationandatdischarge
recommen-dations.
The improvementofbonemineraldensity isassociated
with micronutrient intake (especially of phosphorus,
cal-ciumandzinc), aswellasan adequatesupply ofproteins
with high biological value for age.21 Furthermore, in the
case ofnewborns, exclusive breastfeedingduringthe first
monthsoflifeshouldbeencouraged,asithasbeenshown
tobe aprotective factor for bone formation.22 Thus, the
calculationof thephaseangle usedasan auxiliarytoolto
assessthenutritionalstatuswouldbeimportant,asthe
anal-ysisdoesnotdependonanthropometricalparameters,such
asweightandheightor length,andpossiblyimprovedthe
nutritionalstatusofthepatients.
Thisstudy hassomelimitations. Thefirstwouldbethe
smallnumberofpatients,asitisararedisease.Thesecond
wouldbetoimpossibilitytocreategroupsinrelationtothe
typeof osteogenesis.Athird wouldbethefactthat,
pro-portionally,therearemorefemalepatientsinthegroupof
patientswithOIwhencomparedtothecontrolgroup.We
believe,however,thatbyreportingbioelectricalimpedance
valuescompatiblewithinternationaldatain patientswith
similarschoolage andadolescencephase, pubertal
alter-ations,ifpresent, didnotinfluence thefinal value ofthe
analysis.4
Despitetheselimitations,astherearefewstudiesabout
the nutritional status and classification of children with
osteogenesisimperfecta, thisstudy is importantto
evalu-atetheuseofnewtools(PA)toimprovethetreatmentof
thosewiththecondition.Formoredatatobecollected,we
suggesttheuseofbioelectricalimpedanceasaroutineform
ofassessmentinthesepatients,aswellastheinclusionof
resistanceandreactancedataontheNationalRegisterfor
osteogenesisimperfecta(ReferenceCenterforOsteogenesis
Imperfecta---CentrodeReferênciaemOsteogênese
Imper-feita---Crois--- InstitutoFernandesFigueira ---FIOCRUZ),a
situationwhichwouldpromotetheanalysisofahigher
num-berofpatientsandtheobtainingofmoreconsistentdata.
We conclude that the use of phase angle can help
to classify the nutritional status of children with
multidisciplinary approach. As it is alow cost procedure,
itcan beroutinely incorporated into thecare of patients
withOI in our country. The prospective analysis of these
patients is suggested, as well as their inclusion in the
nationaldatabasetofacilitatethenutritionalimprovement
ofthesepatients,aswellasoftheirbonehealth.
Funding
Master’s Degree Scholarship from Coordenac¸ão de Aperfeic¸oamentodePessoaldeNívelSuperior(Capes).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
TocomputertechniciansVitorHugoPadovanandLuiz Cláu-dioColares.
References
1.Glorieux FH. Osteogenesis imperfecta. Best Pract Res Clin Rheumatol.2008;22:85---100.
2.FariasCL,CamposDJ,BonfinCM,VilelaRM.Phaseanglefrom BIAasaprognosticandnutritionalstatustoolforchildrenand adolescentsundergoing hematopoietic stemcell transplanta-tion.ClinNutr.2013;32:420---5.
3.ChagasCE,RoqueJP,SantarosaEmoPetersB,Lazaretti-Castro M,MartiniLA.Dopatientswithosteogenesisimperfectaneed individualizednutritionalsupport?Nutrition.2012;28:138---42. 4.Bosy-WestphalA,DanielzikS,DörhöferRP,Later W,WieseS,
MüllerMJ.Phaseanglefrombioelectricalimpedanceanalysis: populationreferencevaluesbyage,sex,andbodymassindex. JPENJParenterEnterNutr.2006;30:309---16.
5.Schiesser M, Kirchhoff P, Müller MK, Schäfer M, Clavien PA. The correlation of nutrition risk index, nutrition risk score, and bioimpedanceanalysis with postoperativecomplications in patients undergoing gastrointestinal surgery. Surgery. 2009;145:519---26.
6.OttM,FischerH,PolatH,HelmEB,FrenzM,CasparyWF,etal. Bioelectricalimpedanceanalysisasa predictorofsurvivalin patientswithhumanimmunodeficiencyvirusinfection.JAcquir ImmuneDeficSyndrHumRetrovirol.1995;9:20---5.
7.SchwenkA,BeisenherzA,RömerK,KremerG,SalzbergerB,Elia M.Phaseanglefrombioelectricalimpedanceanalysisremains anindependentpredictivemarkerinHIVinfectedpatientsin theeraofhighlyactiveantiretroviraltreatment.AmJClinNutr. 2000;72:496---501.
8.VanLettowM,KumwendaJJ,HarriesAD,WhalenCC,TahaTE, KumwendaN,etal.Malnutritionandtheseverityoflungdisease inadultswithpulmonarytuberculosisinMalawi.IntJTuberc LungDis.2004;8:211---7.
9.Maggiore Q, Nigrelli S, Ciccarelli C, Grimaldi C, Rossi GA, Michelassi C. Nutritional and prognostic correlates of bioimpedance indexes in hemodialysis patients. Kidney Int. 1996;50:2103---8.
10.PileggiVN,MarguttiAV,MonteiroJP,CameloJSJr.Prevalence ofchildmalnutritionataUniversityHospitalusingtheWorld HealthOrganizationcriteriaandbioelectricalimpedancedata. BrazJMedBiolRes.2016;49:e5012.
11.deOnisM,OnyangoAW,BorghiE,SiyamA,NishidaC,Siekmann J.Development ofa WHO growthreference for school-aged childrenand adolescents.Bull WorldHealth Organ.2007;85: 660---7.
12.PiccoliA,RossiB,PillonL,BuccianteG.Anewmethodfor mon-itoringbodyfluidvariationbybioimpedanceanalysis:theRXc graph.KidneyInt.1994;46:534---9.
13.NaganoM,SuitaS,YamanouchiT.Thevalidityofbioelectrical impedancephaseanglefornutritionalassessmentinchildren. JPediatrSurg.2000;35:1035---9.
14.NormanK,StobäusN,PirlichM,Bosy-WestphalA.Bioelectrical phase angle and impedance vector analysis --- clinical rele-vanceand applicability ofimpedance parameters. ClinNutr. 2012:854---61.
15.Barbosa-SilvaMC,BarrosAJ,PostCL,WaitzbergDL,Heymsfield SB.Canbioelectricalimpedanceanalysisidentifymalnutrition inpreoperativenutritionassessment?Nutrition.2003;19:422---6. 16.TosoS,PiccoliA,GusellaM,MenonD,BononiA, CrepaldiG, etal.Alteredtissueelectricpropertiesinlungcancerpatients asdetectedbybioelectricimpedancevectoranalysis.Nutrition. 2000;16:120---4.
17.AzevedoZM,SilvaDR,DutraMV,ElsasMI,Barbosa-SilvaMC, Fon-secaVM.Associac¸ãoentreângulodefase,PRISMIegravidade dasepse.RevBrasTerIntensiva.2007;19:297---303.
18.HarringtonJ,SochettE,HowardA.Updateontheevaluation andtreatmentofosteogenesisimperfecta.PediatrClinNorth Am.2014;61:1243---57.
19.BarufaldiLA,CondeWL,SchuchI,DuncanBB,CastroTG. Bio-electrical impedance values among indigenous children and adolescentsinRioGrandedoSul,Brazil.RevPanamSalud Pub-lica.2011;30:39---45.
20.Zeitlin L, Rauch F, Plotkin H, Glorieux FH. Height and weightdevelopmentduringfour yearsoftherapy with cycli-cal intravenous pamidronate in children and adolescents withosteogenesis imperfectatypes I, III, and IV. Pediatrics. 2003;111:1030---6.
21.YamaguchiM.Nutritionalfactorsandbonehomeostasis: syner-gisticeffectwithzincand genisteininosteogenesis.MolCell Biochem.2012;366:201---21.