SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Case
Report
Monostotic
fibrous
dysplasia
of
the
metacarpal:
a
case
report
夽
Kátia
Tôrres
Batista
∗,
Hugo
José
de
Araújo,
Ulises
Prieto
y
Schwartzman
HospitalSarahBrasília,CirurgiaPlásticaeCirurgiadeMão,Brasília,DF,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received27October2015
Accepted8December2015
Availableonline26October2016
Keywords:
Disease Metacarpus
Cysticfibrousosteitis
Fibrousdysplasiaofbone
a
b
s
t
r
a
c
t
Fibrousdysplasiaisabonediseasecharacterizedbyabnormaldifferentiationoffibrous
tis-sueinthebones;itisoftenasymptomatic.Itmayaffectonebone(monostotic)orseveral
bones(polyostotic).Themonostoticformprimarilyaffectstheribs,buthardlyeveraffects
thehand.Itisimportanttomakethedifferentialdiagnosiswithmalignantbonetumors.
Thisarticledescribesthetreatmentandoutcomeofararecaseofapatientadmittedwith
ahistoryoftumorgrowthintherighthand,diagnosedasfibrousdysplasiaoftheright
sec-ondmetacarpal.Malepatient,14yearsofage,admittedtotheSarahHospitalwithlesion
onthedorsumoftherighthandwithoutpaincomplaints,previoushistoryoftrauma,nor
localsignsofinflammation.Physicalexaminationrevealedswellingonthedorsumofthe
secondmetacarpal,painless,withunalteredmobilityandsensitivity.Radiography,
com-putedtomography,andmagneticresonanceimagingindicatedtheinvolvementoftheentire
lengthofthesecondmetacarpal:onlythedistalepiphysiswaspreserved,withareasofbone
lysis.Afterbiopsyconfirmation,thepatientunderwentsurgery,usingalongcorticalgraft
forreconstructingthemetacarpal.Duringthefollow-upperiodoffiveyearstherewereno
signsofrecurrence,andproperdigitalgrowthandfunctionalityoftheoperatedhandwere
observed.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora
Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Displasia
fibrosa
monostótica
em
metacarpo
–
Relato
de
caso
Palavras-chave:
Doenc¸a Metacarpo
Osteítefibrosacística
Displasiafibrosaóssea
r
e
s
u
m
o
Adisplasiafibrosaéumadoenc¸aósseaquesecaracterizapeladiferenciac¸ãoanormalde
tecidofibrosonosossoseémuitasvezesassintomática.Podeacometerumosso
(monos-tótica)ou vários ossos (poliostótica). A formamonostótica acomete principalmenteas
costelas,masraramenteacometeamão.Odiagnósticodiferencialcomtumoresósseos
malignosé importante.Oartigo descreveotratamento eevoluc¸ãodeum casoraro de
夽
StudyconductedatHospitalSarah,Brasília,DF,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](K.T.Batista).
http://dx.doi.org/10.1016/j.rboe.2016.10.008
2255-4971/©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Thisisanopenaccessarticle
pacienteadmitidocomhistóriadecrescimentotumoralnamãodireita,naqualfoi
diag-nosticadadisplasiafibrosadosegundometacarpodireito.Pacientedosexomasculino,14
anos,admitidonoHospitalSarahcomlesãonodorsodamãodireita,semqueixaálgica,
antecedentetraumáticooualterac¸ãoflogísticalocal.Noexamefísico,apresentavaaumento
de volume no dorso do II metacarpo, indolor, mobilidade e sensibilidade inalteradas.
Foramfeitosexamesderadiografia,tomografiaeressonânciamagnética,evidenciou-se
ocomprometimentodetodaaextensãodosegundometacarpo;apenas aepífisedistal
estavapreservada,comáreasdeliseóssea.Fez-setratamentocirúrgicoapósabiópsiade
confirmac¸ão,comousodeenxertolongocorticalparareconstruc¸ãodometacarpo.Durante
otempodeseguimentodecincoanosnãoforamverificadossinaisderecidiva;adequado
crescimentodigitalefuncionalidadedamãooperadaforamobservados.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier
EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Theterm fibrous dysplasiawas introducedby Lichtenstain
in1938todescribetheanomalousreplacementofmedullary
bonebyfibroustissue.Itisabenignlesionthatmayinvolve
one(monostotic)ormorebones(polyostotic),orbe
accom-paniedbyothersystemicalterationsandendocrinedisorders,
suchasintheMcCune–Albrightsyndrome.1,2Theetiologyhas
beendescribedasamutationinthegeneencodingthe
sub-unit␣oftheGsproteinlocatedonchromosome20q13.213.3
The natural history of this lesion depends on its
presen-tation; many lesions are asymptomatic, while others may
causepain,bonedeformity,fractures,functionalandcosmetic
changes,andmalignantdegeneration.Themonostoticform
occurswithgreaterpredilectionforthelongbones,ribs,and
radius;few caseshave been described inthe hand.1–4 The
authorsdescribethetreatmentresultsandevolutionofarare
caseofmonostotic fibrousdysplasialocatedon thesecond
metacarpaloftherighthand.
Case
report
Amale14yearoldpatientwasadmittedtotheSarahHospital
with a lesion on the dorsum of the right hand withslow
progressionduringthecourseoftwoyears;thepatienthad
nopaincomplaints, noprevioushistory oftrauma, andno
localsigns ofinflammation.Physical examinationrevealed
painless swellingon the dorsumofthe second metacarpal
withunalteredmobilityandsensitivity.Radiography,CTscan
andmagneticresonanceimagingindicatedtheinvolvement
oftheentirelengthofthesecondmetacarpal:onlythedistal
epiphysis was preserved with areas of bone lysis.(Fig. 1).
Thelevels ofC3 199.0, C4 38.5, and alkaline phosphatase,
aswell asthechestX-raywerenormal.Thepatient
under-went anincisional biopsy disclosingfibrous dysplasia. The
patient then underwent general anesthesia, plexus block,
blodemptyingontheupperlimbusinganEsmarchbandage
and tourniquet positioning with pressure of 200mmHg,
and removalofthelesion onthe second right metacarpal.
Reconstruction was made using a 5-cm bone graft taken
fromtherightfibula.Themetacarpalphalangealjointofthe
second fingerwas preserved,withalocalmargin from the
edgeof1mm;thefibulagraftwasproximallyfixatedwithtwo
transcorticaltitanium screwsand distallywithtwocrossed
1-mmKirschnerwires(Fig.2).Theprocedurewasbloodless.
Thematerialwassenttoforanatomopathological
examina-tion,culture,andantibiogram.Prophylacticantibioticswere
administeredfor48h.Patientwassubmittedtoradiographic
postoperativecontrol(Fig.3)andimmobilizationwithcircular
antebrachiopalmarplasterforsixweeks.Kirschnerwireswere
removedaftersixweeksafterbonegrafthealing,when
phys-icaltherapyprogramwasinitiated.Thetranscorticalscrews
wereremovedafterfiveyears,duetolocalpaincomplaints.
Theresultofthehistopathologicalexamindicatedfibrous
dys-plasiawith46,XY,add(6)(q27),t(14:21)(q22;p1?11.2)[4]/46,XY[12]
karyotype(Fig.4).Follow-upcontinuedforfiveyearswithout
recurrence,showingnormalfunctionoftheoperatedhand.
Discussion
Fibrousdysplasiarepresents7%ofbenignbonetumors,and
itsexactetiologyisunknown.Themonostoticformismore
commonandtheradiographicfindingsarenonspecific.5–7
Theetiologyofthetumorremainsunclear,butitappears
tobelinkedtoasinglenucleotidemutationintheGs␣gene
onthelongarmofchromosome20(20q13.2-3),whichresults
inadisturbanceofthetissuedifferentiationprocess.1,8This
mutationoccursinsomaticcellssometimeafterfertilization,
andthereforeisnotinherited.Chromosome12hasalsobeen
implicatedinthepathogenesisoffibrousdysplasia;however,
to date, no chromosomal abnormalities have been
consis-tently demonstrated.Thelesions inthe longbonesusually
appear in the metaphysis as an intramedullary expansion
withcortexthinningandhazyaspect;however,dependingon
theextentofthefibroustissueanddysplasticchangesinbone,
aswellasthedegreeofcalcification,thefindingsmay vary
from sclerotic toradiolucent.3,7 Clinically,theselesionsare
eithercharacterizedbyvolumeexpansionorasymptomatic.
Asinseveraltumors,thedifferentialdiagnosisshouldinclude
sarcomas.
Radiographically, the differential diagnosis may include
Paget’s disease, solitarybone cysts, aneurysmalbone cyst,
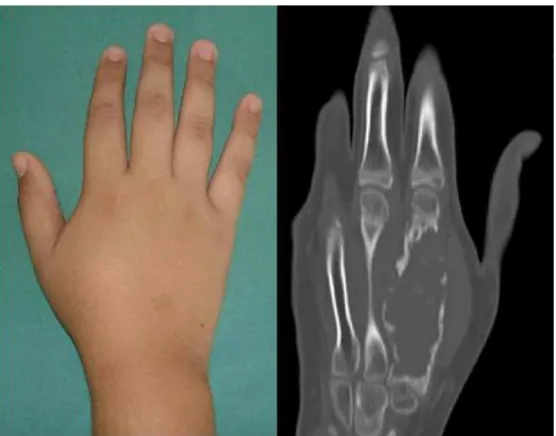
Fig.1–Physicalandradiologicalexaminationshowingthetumoronthesecondmetacarpal.
osteosarcoma,osteofibrousdysplasia,andgiantcelltumor.3
Theradiological findings suggestive ofmalignancy include
lyticregionsinpreviouslymineralizedareas,intralesional
cal-cification, periosteal reaction, cortical disruption, and soft
tissue invasion. Some aspects of these alterations were
observed preoperatively inthe present case.Moreover, the
needforpreoperativebiopsyforthediagnosisofbonetumors
shouldbeemphasized.
Fig.3–Radiologicalfollow-upofthehandinthepostoperativeperiod.
Malignanttransformationoccurswithrapidbonegrowthin
approximately0.5%ofpatientswithmonostoticfibrous
dys-plasiaandin4%ofthosewithMcCune–Albrightsyndrome,1,2
withosteosarcoma beingthemostcommon.Other tumors,
suchasfibrosarcoma,chondrosarcoma,ormalignantfibrous
histiocytoma,mayalsobeobserved.Histologically,low-grade
osteosarcoma ismorecellular, moreatypical,and presents
moremitosis, havingahigher activitythan fibrous
dyspla-sia.Furthermore,theregularlyspacedbonyspiculesseenin
fibrousdysplasiaarenotpresentinosteosarcoma.2
Thetreatmentoffibrousdysplasiaforasymptomaticand
stablelesionsisregularfollow-up.Surgeryisindicatedonlyfor
confirmationbiopsy,correctionofdeformities,non-operative
therapy failure, preventionofpathological changes,and/or
eradicationofsymptomaticlesions.1,9–11Incasesoffractures,
thetreatmentcanbedonewithclosedfixation.Other
treat-mentoptionsincludecurettage,curettageplusbonegraft,or
internalfixation.9–11Moreextensivecasesmayrequirebone
graftorvascularizedbonegraft.12
In the present case, three important aspects should be
highlighted:thefirstistheoccurrenceofsecondmetacarpal
monostoticdysplasiaintheupperlimb,alesscommonarea;
thesecondistheimportanceofthedifferentialdiagnosiswith
other lesions, including malignant degeneration; the third
aspectisthetreatmentusingfreecorticalbonegraft,allowing
foradequatebonelengthofthefingerandnormalfunctionof
thehand.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. DiCaprioMR,EnnekingWF.Fibrousdysplasia.
Pathophysiology,evaluation,andtreatment.JBoneJointSurg Am.2005;87(8):1848–64.
2. ResnickD,KyriakosM,GreenwayGD.Tumorsandtumorlike lesionsofbone:imagingandpathologyofspecificlesions.In: ResnickD,KransdorfMJ,editors.Diagnosisofbonedisorders. Philadelphia:WBSaundersCompany;2002.
3.FitzpatrickKA,TaljanovicMS,SpeerDP,GrahamAR,Jacobson JA,BarnesGR,etal.Imagingfindingsoffibrousdysplasiawith histopathologicandintraoperativecorrelation.AmJ
Roentgenol.2004;182(6):1389–98.
4.SniedersMN,vanKemenadeFJ,vanRoyenBJ.Monostotic fibrousdysplasiaofalumbarvertebralbodywithsecondary aneurysmalbonecystformation:acasereport.JMedCase Rep.2009;3:7227.
5.ShahZK,PehWC,KohWL,ShekTW.Magneticresonance imagingappearancesoffibrousdysplasia.BrJRadiol. 2005;78(936):1104–15.
6.TraibiA,ElOueriachiF,ElHammoumiM,AlBouzidiA,Kabiri elH.Monostoticfibrousdysplasiaoftheribs.Interact CardiovascThoracSurg.2012;14(1):41–3.
7.HughesEK,JamesSL,ButtS,DaviesAM,SaifuddinA.Benign primarytumoursoftheribs.ClinRadiol.2006;61(4): 314–22.
8.KumtaSM,LeungPC,GriffithJF,KewJ,ChowLT.Vascularised bonegraftingforfibrousdysplasiaoftheupperlimb.JBone JointSurgBr.2000;82(3):409–12.
9.CasoMartinezJ,AgoteJemeinJA,AránSantamaríaC,López UnzuA.Monostoticfibrousdysplasiainthehand.Acase report.AnnChirMainMembSuper.1994;13(4):
282–4.
10.YanagawaT,WatanabeH,ShinozakiT,TakagishiK.Curettage ofbenignbonetumorswithoutgraftsgivessufficientbone strength.ActaOrthop.2009;80(1):9–13.
11.RemottiF,FeldmanF.Nonneoplasticlesionsthatsimulate primarytumorsofbone.ArchPatholLabMed.
2012;136(7):772–88.