SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Experience
in
fixation
of
infected
non-union
tibia
by
Ilizarov
technique
–
a
retrospective
study
of
42
cases
夽
Jimmy
Joseph
Meleppuram
∗,
Syed
Ibrahim
VinayakaMissionsMedicalCollegeandHospital,DepartmentofOrthopaedics,Pondy,India
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received15September2016 Accepted10November2016 Availableonline30December2016
Keywords: Tibia
Ilizarovtechnique Infection Externalfixators
a
b
s
t
r
a
c
t
Objective:Theaimofthestudyistoevaluatetheclinicalandfunctionaloutcomein treat-mentofinfectedtibialnonunionbytheIlizarovmethod.
Methods:Theauthorsretrospectively analyzed42patientswithinfectedtibialnonunion withboneloss;shorteninganddeformitytreatedatthisinstitutionduringtheperiodof February2012toApril2015wereincludedinthestudy.Theresultswereevaluatedaccording toAssociationfortheStudyandApplicationoftheMethodsofIlizarov(ASAMI)criteria.Pin tractinfectionswereassessedbyMooreandDahlscore.
Results:Boneresultswereexcellentin60%ofpatients(n=25),goodin15%(n=6),fairin25% (n=11),andpoorinnone.Thefunctionalresultswereexcellentin55%ofpatients,goodin 30%,fairin5%,andpoorin10%.Themostcommoncomplicationfoundinthisstudywas pintractinfection.
Conclusion:Ilizarovring fixator stillremains an excellent treatment modality fortibial nonunion,asitaddressestheproblemsassociatedwiththecondition,althoughthe pro-cedureiscumbersome.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Experiência
na
fixac¸ão
de
pseudartrose
infectada
da
tíbia
usando
a
técnica
de
Ilizarov
–
estudo
retrospectivo
de
42
casos
Palavras-chave: Tíbia
TécnicadeIlizarov Infecc¸ão
Fixadorexterno
r
e
s
u
m
o
Objetivo:Oobjetivodoestudoéavaliarodesfechoclínicoefuncionalnotratamentoda pseudartroseinfectadadatíbiapelométododeIlizarov.
Métodos:Osautoresanalisaramretrospectivamente42pacientescompseudartrose infec-tadadatíbiacomperdaóssea.Oscasosdeencurtamentoedeformidadetratadosnesta instituic¸ãoduranteoperíododefevereirode2012aabrilde2015foramincluídosnoestudo.
夽
WorkperformedintheVinayakaMissionsMedicalCollegeandHospital,DepartmentofOrthopaedics,Pondy,India.
∗ Correspondingauthor.
E-mail:[email protected](J.J.Meleppuram).
http://dx.doi.org/10.1016/j.rboe.2016.11.008
OsresultadosforamavaliadosdeacordocomoscritériosdaAssociac¸ãoparaoEstudoe Aplicac¸ãodosMétodosdeIlizarov(AssociationfortheStudyandApplicationoftheMethods ofIlizarov[ASAMI]).Asinfecc¸õesnotrajetodosfiosepinosforamavaliadaspelaclassificac¸ão deMooreeDahl.
Resultados: Osresultadosósseosforamexcelentesem60%dospacientes(n=25),bonsem 15%(n=6)emoderadosem25%(n=11);nenhumpacienteapresentouresultadosruins.Os resultadosfuncionaisforamexcelentesem55%dospacientes,bonsem30%,razoáveisem 5%eruinsem10%.Acomplicac¸ãomaiscomumencontradanesteestudofoiinfecc¸ãono trajetodosfiosepinos.
Conclusão: Emborasejaumprocedimentocomplicado,afixac¸ãodeIlizarovcontinuaaser umamodalidadedetratamentoexcelenteparapseudartrosedatíbia,umavezqueaborda osproblemasassociadosàcondic¸ão.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Tibia,asasubcutaneousbonewhichisvulnerabletotrauma anditsfracturesarecommonwhicharemostlyopenand com-plexamongthelongbonefractures.Delayedunion,non-union withassociated infection are relatively common complica-tionsseen.Thenon-unionrangesfrom3to11%ofalltibia fractures.Treatmentofinfectednon-unionoftibiaisoneof theperplexingdilemmasinorthopaedicsurgerybecauseof itsdelayedmanagementafterahighenergytrauma,asithas thinsofttissuecoveragewithpoorvascularsupplyand com-plexfracturepatternsthatresultusuallyinanunfavourable outcome.
Aftermultiplesurgerieswithhugeburdenofcostaswell as prolonged period of immobilization makes the patient lifemiserable, eventhenthe endresultsareunsatisfactory along withamputation may still bethe outcome.To erad-icate infection and to establish bony union with a good functional extremity oftenrequires a courageousmeasure. Thetreatmentofinfectednon-union oftibiabydistraction osteosynthesis using ilizarovtechnique can alsoaddress a coincidingdeformity,boneloss,shorteningorinfection.1
AcordingtoIlizarov,toeliminateinfectionandobtainbony union,concernedvascularitymustbeincreased.Inthis tech-nique,vascularityisincreasedbycorticotomyandapplication ofacircularexternalfixator.Italsoprovidesmicromotiondue todistractionandgivesanexcellentbiologicalenvironment forfracture healing.2 Ilizarov technique hasthe additional
advantageofefficientfixationwhichallowsearly mobiliza-tionandmaintainsarticularfunction,eliminatestheneedfor bonegraftingandhasminimalcomplications.3
Inourstudy,weanalyzedtherole ofilizarov fixationin infected non-union of tibia, we assessed for bony union, infection,functionaloutcomeandtoknowthecomplications associatedwithit.
Materials
and
methods
Fortytwopatientswithinfectednon-unionoftibiaformore than6monthstreatedbyilizarovfixationmethodfrom Febru-ary 2012to April 2015were retrospectively analyzed from
Table1–Non-union–GSKulkarni’sclassification.
TypeI Fragmentsinappositionwithmild infectionandwithorwithoutimplant TypeII Fragmentsinappositionwithsevere
infectionwithlargeorsmallwound TypeIII
IIIa IIIb IIIc
Severeinfectionwithagapor deformityorshortening
Defectwithlossoffullcircumference Defectin>1/3rdofcortex
Infectednon-unionwithdeformity
hospitalrecords.There were10femalesand 32maleswith anaverageageof38years(range,26–64years)attheinitial operation.Majorityweremanuallabourersandinjurieswere causedbyroadtrafficaccidents(n=36)andbyfallfromheight (n=6).Therightsidewasincludedin24cases(57%)andthe leftsidein18cases(43%).Infectednon-unionwasclassified byG.S.Kulkarniclassification(Table1).3Infectednon-union
ofdistalonethirdtibiaconstitutedthemostnumberofcases inourstudy.
Inclusioncriteria
Allinfectednon-unionoftibiaassociatedwith:
1. Bonelossoflessthan10cm.
2. Varyingdegreeoflimbshorteningoflessthan2.5cmand deformitylessthan5degrees.
3. Bothmaleandfemale
4. Infectednon-uniontibiaofmorethan6monthsduration.
Exclusioncriteria
1. Congenitalpseudoarthrosisoftibia.
2. Non-uniontibianotassociatedwithinfection. 3. Freshcompoundfractures.
4. Infectedfractureslessthan6months.
Surgicaltechnique
surgeryaccordingtorequiredlengthandwidth.Oblique inci-sionwaspreferredtoavoidwoundclosureproblems.Initial hardwareif presentwas removedandinpatientswho had previousintramedullarynail,reamingoftibiawasdone.The boneendswerethoroughlydebridedandsamplesweretaken formicrobiologyand histopathologyanalysis. Bothends of thebone,if neededwerekeptinalignment withplate and screwstemporarilyandthenframewasappliedwith trans-osseuswiresalongwithhalfpinstopreservetheanatomical axisandavoidanyadditionalsofttissuedamage.Ifrequired, the frames were extended to the foot to minimize equi-nus deformity whenever necessary. Tourniquet was used until debridement and freshening of the edges. The wires introducedafterremovaloftourniquetandweretensionedup to110kgusingtensioner.Ifsofttissuecoveragewasrequired thenthiswasdonebyplasticsurgeonsatthesamesitting. Cor-ticotomywasperformedassecondstageprocedureinneeded casesbywiresusingDeBastianitechnique.4Wheneverunion
isdelayed,weaugmentednon-unionsitewithbonemarrow injectionorbonegrafting.
Postoperatively patient wason appropriateintravenous antibioticsandanalgesicsforaweekwithlegpositionedover thepillowsothatkneekeptextendedallthetimes,passive dorsiflexionsplintsfortheanklewasgiven.Topromoteearly bonehealingimmediateweightbearingwasencouraged in mostcases,intensivephysiotherapytomaintainortoregain normalrangeofmotionofthekneeandanklejointswas con-sideredanimportantpartofthetreatment.
Aftersurgerytherewasnochangesforinitial7days; there-afterallmanipulationsweredonebythepatientsthemselves byturningnutsonthefixatoroftheapparatusfourtimesa day,resultinginmovementintheaxisoftheboneof1mm perday.Incasesrequiringinternalbonetransport,thebone segmentbetweenthenon-unioncorticotomysitewasmoved distallyandthebonesegmentreachedtheformernon-union siteeventuallyfollowedbydocking.
Consequentlyweevaluatedpatientseverytwoweeks clini-callyforpintractinfections,stabilityofframeandradiological assessmentwasdoneeveryfourweeksforunionatthe non-unionsite andconsolidationofthe regenerate.Fixatorwas removed when the regenerate consolidated and the non-unionwascorticolizedonthreeoffoursidesasseenonthe anteroposteriorandlateralX-rays.5,6Weusedprotectivecasts
foranadditional2monthsbecauseofourfearofrefracturein allourcases.
Results
Inourstudyof42patients,nopatientswerelostduringfollow up.Atfollowupexamination14months(range10–24months) afterframeremovalthefinaloutcomewasevaluatedby crite-rialaiddownbyAssociation fortheStudyandApplication ofthe MethodsofIlizarov(ASAMI) forboneand functional results.7Inmajorityofthecasesexternalfixatorheldfora
timeperiodof8–10months.Bone lossafterinitial debride-mentwas2.5–5.5cminmostofourcases.
Inourstudy,85%ofthepatientsweretreatedbybifocal osteosynthesis,whichisacutedockingofthenon-unionsite followedbycorticotomy anddistraction atother site.Limb
Fig.1–Grade4pinsiteinfectionaccordingtoMooreand Dahlclassification.
lengthdiscrepancywasassessedattheendoftreatmentafter union.In35%ofcasestherewasnolimblengthdiscrepancy aftertreatment.Inmostcasesthelimblengthdiscrepancywas 0.5–1.5cm.
In terms of organism, 28 patients grew staphylococcus aureus, sixpatientsgrewpseudomonas,four patientsgrew coagulationnegativestaph,twogrewstreptococcusviridans andpropionibacteriumeach,andtwopatientshadnegative cultureastheywereonantibioticspreoperatively.
Bone resultswere assessedbyASAMIscoring.An excel-lentboneresultwasonethathadnoevidenceofinfection,a deformityof5degreeorlessinanyoneplane,anlimblength discrepancy (LLD) less than 2.5cm and a boneunion wide enoughnottorequirelongtermbracingorprotection.7Inour
study,wehadexcellentresultsin60%ofcases(n=25),all42 patientshadsuccessfulunionafterilizarovbonetransportat theendofoneyear,andnonerequiredamputation.
Functional results were assessed byASAMI scoring. An excellentfunctionalresultwasoneinwhichthepatienthad nopainormildpain(notrequiringnarcotics),didnotrequire awalkingaidorbrace,didnothavejointcontracturegreater than 5 degree, didnot lose morethan 20 degree of ankle motion,andwasabletoperformallactivitiesofdailyliving.7
Inourstudy,functionalresultswereexcellentin55%(n=23) ofcases.
Complications were sub classified according to Paley in “problems”solvedduringtreatmentwithoutoperative inter-vention, “obstacles”thatrequiresanoperativeintervention andtrue“complications”thatwerenotresolvedbeforetheend oftreatment.8Thetruecomplicationswereconsideredminor
iftheydidnotinterferewithachievingtheoriginalgoal.We recorded38problemsin42patients;theproblemsconsisted mainlyofpintractproblemsofwhich30patientswithpin siteinflammationwhichsubsidedwithregulardressingsand oralantibiotics.Fivepatientswithpinsitesofttissueinfection wereresolvedbyintravenousantibiotics(Fig.1).Threepatient hadtransientparesthesiawhichresolvedbyitself.
revisionfordriftingtransportfragment(n=4),debridement andgraftingatdockingsite(n=11),repeatosteotomy(n=2), iliac bone graft to regenerate (n=2), and foot plate addi-tion for equinus contracture (n=1). There were no major complicationsinourstudy.
Discussion
Theilizarovtechniqueoffersaneffectiveandreliable treat-ment for some of the most challenging conditions in orthopaedicpracticesuchasinfectednon-union oftibia. It wasinitiallydevelopedinKurgan,Russiain1950byProf.Gavril A.Ilizarov.Infectedtibialnon-unionsareacomplicated prob-lem requiringcomplex time consuming surgery.Our study hasdemonstrated,goodfunctioncanbeachievedinterms ofunion,infection,painrelief andactivitiesofdailyliving. Presentstudy,usingASAMIcriteria,whereonparwithother studies.
Adiagnosis ofnon-union can bemade whenatleast 6 monthshaveelapsedwithnoevidenceofprogressionof heal-ing after the time offracture, atthis point, if there is an infectionthenittendstobechronicandorganismtendsto beresistanttomostantibiotics.9,10 Radicalwound
debride-mentwithallnecrotic boneshouldbecompletelyremoved togetherwithproblemslikeleglengthdiscrepancy,deformity, jointstiffness;diffuseosteoporosisshouldbeaddressed.11In
ourstudy,100%eradicationofinfectionwasnotedwhichis
Table2–Bonyresultscomparison.
Results Excellent Good Fair Poor
Paley15 60.87% 26.09% 8.7% 4.35%
Madhusudhanetal.16 22% 36.34% 22% 18.18%
Dendrinosetal.11 50% 29% 3.6% 17.4%
Lalitetal.17 70% 10% 0% 20%
Presentstudy 60% 15% 25% 0%
comparabletootherstudies.11,12Thoughilizarovhadnotused
antibiotics, we have used both appropriateoral and intra-venousantibioticsdependingupontheculturereportfor4–6 weeks.
Inourstudydurationofexternalfixationwas8–10months inmostcaseswhichiscomparabletootherstudies.13Inour
studywenotedbonelengtheningindexi.e.durationrequired forformationof1cmofnewbonewas1.48.Studieshasshown smokinghasapoorstaticallyoutcomeondurationof exter-nalfixatorandbonelengtheningindex.14Ourpatientswere
strictlyadvisedtostopsmokingduringthecourseof treat-ment.
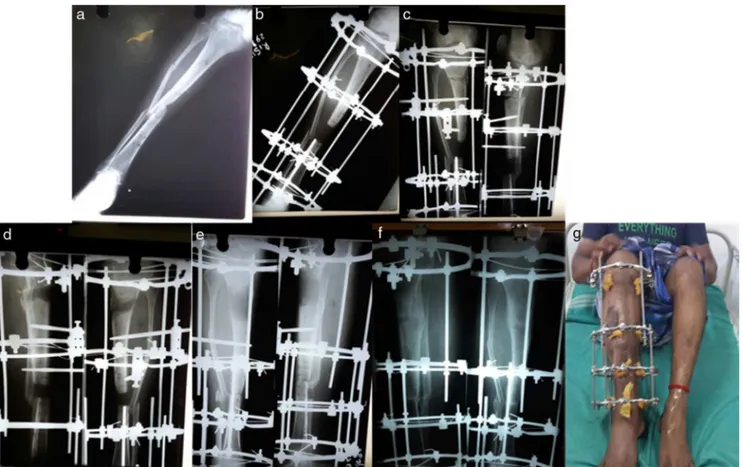
Inourstudy,boneresultswereexcellentin60%ofcases (Fig.2),goodin15%ofcases(Fig.3),fairin25%ofcasesand did not have any poor resultsmaking it superior toother studies (Table 2).15,16,11,17 Inourcurrentstudy thoughbone
resultswere better than functional results.Itshows excel-lent bone doesnot guarantee good functionoutcome.The
Fig.2–(a)36yearoldmalewithinfectednon-unionrighttibiatypeIIIcofKulkarni’sclassification.(b)Post-opXrayshowing radicaldebridementandpreliminaryilizarovringfixation.(c)X-rayshowingpostcorticotomystatus.(d,e)X-rayshowing bonetransport,(f)fractureunited,(g)ilizarovfixatorinsituafter8monthsofunionwithexcellentunionandexcellent
Fig.3–(a)A40yearoldmalewithinfectednon-unionlefttibiatypeIIcofKulkarni’sclassification.(b)Immediatepost-op X-rayshowingradicaldebridementandpreliminaryilizarovringfixation.(c)1monthX-rayshowingcorticotomydone.(d) X-rayshowingongoingbonetransportanddocking.(e)UnitedfracturewithIlizarovringremoved(f)Ilizarovfixator
removedafter7monthsofunionwithexcellentunionandgoodfunctionaloutcome.
functionalresultisaffectedbythesofttissueand neurovascu-larstructures.8Ourfunctionalresultswerebetterascompared
tootherstudies(Table3).
Inourstudy,of42patientswehad50complicationsatthe rateof1.6complicationsperpatientwhichwascomparableto otherstudies.Inthat,therewere38problemsand20 obsta-cles,among38problems30wereduetopintractinfections assessedbyMooreandDahlgrading(Table4).Amongwhich 16patientshadGradeIIinfection,12patientshadgradeIII infectionandtwohadGradeIVinfection forwhichthepin
Table3–Functionalresultscomparison.
Results Excellent Good Fair Poor
Paley15 64% 28% 4% 4%
Madhusudhanetal.16 5.56% 22.22% 33.33% 38.89%
Dendrinosetal.11 25% 39.2% 14.3% 2.15%
Lalitetal.17 26.7% 40% 10% 28.3%
Presentstudy 55% 30% 5% 10%
wasremovedandre-applied.Thehighrateofpintract infec-tionwasduetolowsocioeconomicalstatusandresidenceat villageswherefacilitiesforregulardressingwerealsoless.Soft tissuecomplicationsincludingwoundbreakdown, invagina-tionandsignificantjointcontractureswerenotverycommon inourstudyascomparedtootherstudies.Wealsofoundthat multidisciplinaryapproachwasverymuchhelpfultoour suc-cessfuloutcomes.18
Table4–MooreandDahlpinsiteclassification.
Grade Inflammation
0 Noneormarginal
1 Marginalinflammation
2 Inflamed–serous
3 Inflamed–purulent
4 Inflamedwithinduration–seropurulent 5 Inflamedwithinduration,tenderness,
Conclusion
Overall ilizarov bone transport is an effective salvage tool inobtainingunion inpatients withaninfected non-union associatedwithboneloss.Thelengthytreatmenttimeand considerablenumberofcomplicationsmustbefully under-stoodbothbythesurgeonandthepatientbeforeundertaking thisuniquetreatmentprocess.Inordertoobtainfasterunion rate patient should be a non-smoker and smokers should bestrictlyadvisedcessationofsmoking.Thistechniquealso givesbetterresultsinconcerntobonehealingandalsogives anopportunityforcorrectionofdeformitiesandshorteningat thesametime.
Conflict
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. AronsonJ,JohnsonE,HarpJH.Localbonetransportationfor treatmentofintercalarydefectsbytheIlizarovtechnique. Biomechanicalandclinicalconsiderations.ClinOrthopRelat Res.1989;(243):71–9.
2. IlizarovGA.Thetension-stresseffectonthegenesisand growthoftissues.PartI.Theinfluenceofstabilityoffixation andsoft-tissuepreservation.ClinOrthopRelatRes.
1989;(238):249–81.
3. MarshDR,ShahS,ElliottJ,KurdyN.TheIlizarovmethodin nonunion,malunionandinfectionoffractures.JBoneJoint SurgBr.1997;79(2):273–9.
4. DeBastianiG,AldegheriR,Renzi-BrivioL,TrivellaG.Limb lengtheningbycallusdistraction(callotasis).JPediatrOrthop. 1987;7(2):129–34.
5. MaffulliN,LombariC,MatarazzoL,NeleU,PagnottaG,Fixsen JA.Areviewof240patientsundergoingdistraction
osteogenesisforcongenitalpost-traumaticorpostinfective lowerlimblengthdiscrepancy.JAmCollSurg.
1996;182(5):394–402.
6.PaleyD.Currenttechniquesoflimblengthening.JPediatr Orthop.1988;8(1):73–92.
7.PaleyD,MaarDC.Ilizarovbonetransporttreatmentfortibial defects.JOrthopTrauma.2000;14(2):76–85.
8.PaleyD,Problems.obstacles,andcomplicationsoflimb lengtheningbytheIlizarovtechnique.ClinOrthopRelatRes. 1990;(250):81–104.
9.TowersAG.Woundinfectioninanorthopaedichospital. Lancet.1965;2(7408):379–81.
10.GristinaAG,NaylorPT,MyrvikQN.Mechanismsof musculoskeletalsepsis.OrthopClinNorthAm. 1991;22(3):363–71.
11.DendrinosGK,KontosS,LyritsisE.UseoftheIlizarov techniquefortreatmentofnon-unionofthetibiaassociated withinfection.JBoneJointSurgAm.1995;77(6):835–46.
12.García-CimbreloE,Martí-GonzálezJC.Circularexternal fixationintibialnonunions.ClinOrthopRelatRes. 2004;(419):65–70.
13.SenC,EralpL,GunesT,ErdemM,OzdenVE,KocaogluM.An alternativemethodforthetreatmentofnonunionofthetibia withboneloss.JBoneJointSurgBr.2006;88(6):783–9.
14.McKeeMD,DiPasqualeDJ,WildLM,StephenDJ,KrederHJ, SchemitschEH.Theeffectofsmokingonclinicaloutcome andcomplicationratesfollowingIlizarovreconstruction.J OrthopTrauma.2003;17(November–December(10)): 663–7.
15.PaleyFB,ChirstiansonD.AnanalysisofIllizarovandexternal fixators.ClinOrthopRelatRes.1989;(241):195.
16.MadhusudhanTR,RameshB,ManjunathK,ShahHM, SundareshDC,KrishnappaN.OutcomesofIlizarovring fixationinrecalcitrantinfectedtibialnon-unions–a prospectivestudy.JTraumaManagOutcomes.2008;2(1):6.
17.LalitM,ChadhaM,VishwanathJ,KapoorS,MehtaniA,Dhaon BK.TheIlizarovmethodininfectednonunionoffractures. Injury.2000;31(7):509–17.