Brazilian
Journal
of
OTORHINOLARYNGOLOGY
www.bjorl.org
ORIGINAL
ARTICLE
Profile
of
patients
assessed
for
cochlear
implants
夽
Maria
Helena
de
Magalhães
Barbosa
a,∗,
Felippe
Felix
b,c,
Marcia
Gonc
¸alves
Ribeiro
d,
Shiro
Tomita
e,f,
Cintia
Pinheiro
b,
Monica
Machado
Baptista
baServiceofOtorhinolaryngology,HospitalUniversitárioClementinoFragaFilho(HUCFF-UFRJ),RiodeJaneiro,RJ,Brazil bUniversidadeFederaldoRiodeJaneiro(UFRJ),RiodeJaneiro,RJ,Brazil
cHospitaldosServidoresdoEstado(HSE/RJ),RiodeJaneiro,RJ,Brazil
dInstitutodePuriculturaePediatriaMartagãoGesteira(IPPMG),HospitalUniversitárioClementinoFragaFilho(HUCFF-UFRJ),
RiodeJaneiro,RJ,Brazil
eUniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil
fDepartmentofOtorhinolaryngology,UniversidadeFederaldoRiodeJaneiro(UFRJ),RiodeJaneiro,RJ,Brazil
Received26May2013;accepted22March2014 Availableonline11June2014
KEYWORDS
Cochlearimplants; Healthprofile; Hearingloss,bilateral
Abstract
Introduction:Knowledgeofthecharacteristicsrelatedtoprofoundhearinglossisamatterof greatimportance,asitallowsfor theetiologicalandprognostic identificationandstrategic planningforpublichealthinterventions.
Objective: Toassess thedifferentetiologies ofhearing loss,ageatdiagnosisofthehearing loss,itsrelationtolanguageacquisition,andtheageatthefirstconsultationinthisservicefor cochlearimplantassessment.
Methods:This was ahistorical cohort, cross-sectional study,usingretrospective analysis of therecordsof115patientswithconfirmedsensorineuralhearingloss,whowerefollowedina universityhospital,basedongender,ageofhearingloss,ageatthefirstconsultation,language, andhearinglossetiology.
Resultsandconclusion:Themajorityofpatientsassessedforcochlearimplantsattendthefirst consultationwhentheyareolderthanoneyear(analarmingmeanof3.8yearsintheprelingual group)inspiteoftheearlydiagnosisofhearingloss.Thisreflectsanalreadydeficienthealth caresystem,intermsofreferral.Theidiopathiccauseremainsthemostfrequentlyidentified. Amongtheknowncauses,themostprevalentareperinatalcausesandmeningitis.
© 2014Associac¸˜aoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:BarbosaMH,FelixF,RibeiroMG,TomitaS,PinheiroC,BaptistaMM.Profileofpatientsassessedforcochlear
implants.BrazJOtorhinolaryngol.2014;80:305---10. ∗Correspondingauthor.
E-mail:[email protected](M.H.deMagalhãesBarbosa).
http://dx.doi.org/10.1016/j.bjorl.2014.05.011
1808-8694/©2014Associac¸ãoBrasileirade OtorrinolaringologiaeCirurgiaCérvico-Facial.Published byElsevierEditoraLtda.Allrights
PALAVRAS-CHAVE
Implantecoclear; Perfildesaúde; Perdaauditiva bilateral
Perfildospacientesemavaliac¸ãoparaimplantecoclear
Resumo
Introduc¸ão:Oconhecimentodascaracterísticasrelacionadasàperdaauditivaprofundaéde extrema importância já que permite a identificac¸ão etiológica ede fatores prognósticos e planejamentoestratégicoparaintervenc¸õesdesaúdepública.
Objetivo:Verificarasdiferentesetiologiasdaperdaauditiva,idadedediagnósticodaperda, relacionadaounãoàaquisic¸ãodelinguagemeidadedospacientesaoprocuraroservic¸opara aavaliac¸ãodeimplantecoclear.
Método: Estudodecasos,decoortehistóricatransversal,comanáliseretrospectivadearquivos de115pacientescomperdaauditivaneurossensorialcomprovadaacompanhadosnumhospital universitário, combaseem sexo, idade daperda, idade naprimeira consulta,linguagem e etiologiadaperda.
Resultadoseconclusão:ospacientesavaliadosparaimplantecoclearchegamàprimeira con-sulta,emsuamaioria,commaisdeumanodeidade(médiapreocupantede3,8anosnogrupo pré-lingual),apesardeodiagnósticodaperdaserprecoce,oquerefleteumsistemaainda defi-cienteemtermosdereferenciamento.Acausaidiopáticaaindaéamaisencontrada.Dentre asetiologiasconhecidas,asmaisprevalentessãoasperinataiseameningite.
©2014Associac¸˜aoBrasileira deOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicadopor ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
DatafromthelastcensusconductedbytheBrazilian Insti-tute of Geography and Statistics (Instituto Brasileiro de Geografiae Estatística---IBGE)in 2010 showthat approx-imately 9.7 million Brazilians have hearing loss, which is severe in approximately 2 million individuals. There are morethan770,000individualswithhearinglossamongthe populationofRiodeJaneirostate.1
It is known that the prevalence of congenital hearing lossexceedsthatof manydiseasesamenabletoscreening in childhood, such as phenylketonuria, sickle-cell ane-mia, congenital hypothyroidism, and congenital adrenal hyperplasia.2,3 A study conducted in 1998, at the begin-ningoftheimplementationofuniversalhearingscreening, demonstratedthatchildrenwithhearinglosswhoundergo interventionbefore6 monthsof ageto3yearshave rates ofreceptiveandexpressivelanguagecomparabletothatof children withnormal hearing, andthat favorable progno-sisinearlyinterventiondoesnotdepend onthedegreeof hearingloss.4
Similarly,individualswithpost-lingualhearinglossshow progressive language deterioration according to the time ofsounddeprivation,whichdeterminesnegativeimpacton theirqualityoflifeandindicatestheneedforearly detec-tionandauditoryrehabilitation.
Thesedataindicatethemagnitudeofhearinglossinthe populationandshowtheimportanceofearlydetectionand referralofthesepatientsforassessment,whichallowsfor propermanagementandimprovedqualityoflife.
Inthis context,theimportanceofidentifyingthe etio-logicalcauseofhearinglossis emphasized,astheprocess becomesmoretargetedtowardtheinterventionand reha-bilitationprocess.
InRiodeJaneiro,cochlearimplantsurgerybythe Brazil-ianPublic HealthSystem (Sistema Únicode Saúde--- SUS)
startedinJuly2011,andatotalof32patientshadreceived implantsbyMarch2013.
The objectiveofthis study wastoassessthe different etiologiesofhearingloss,ageat diagnosisofhearingloss, relationship tolanguageacquisition (pre-or post-lingual), andageofpatientwhenhe/shepresentedtotheservicefor cochlear implantassessment.Withthesedata,thequality ofhearinghealthcarecanbeinferred,inordertopromote theimplementationofimprovementmeasures.
Materials
and
methods
This study was approved by the ethics committee of the institution underresearchprotocol number043/11 --- CEP. A retrospective analysis of the records of 115 patients withprovenprofoundsensorineuralhearinglossreferredfor cochlearimplantassessmentattheotorhinolaryngology out-patientclinicofauniversityhospitalbetween2011and2013 wasperformed.Theassessedpatientswereallsubmittedto tonalandvocalorbehavioralaudiometry,performedbythe samequalifiedaudiologistfromthisservice,including otoa-cousticemissions(OAEs)testandbrainstemauditoryevoked potential(BAEP)testcarriedoutbyexpertsin otolaryngol-ogy, computed tomography (CT),and magnetic resonance imaging(MRI)ofthemastoidsandauditorypathways.
1%
36%
<1 year
1-4 years
5-19 years
20-40 years
>40 years Age
26% 14%
23%
Figure 1 Percentage distribution by age range ofpatients undergoingevaluationforcochlearimplant.
Patientswhodid notmeetthe criteria, or whohadno indicationorreleasebyallprofessionalsinvolvedintheuse of cochlear implants underwentfollow-up at the Hearing Health Outpatient Clinic,which involves otolaryngologists and speech therapists, to maximize hearing gain and/or communicationskills.
Thedataanalyzedweregender,age,etiologyofhearing loss,ageatfirstconsultation,andthetypeofhearinglossin relationtolanguageacquisition(pre-orpost-lingual).These werearrangedinchartsforstatisticalpurposes.
Results
Mostofthepatientsevaluatedwereaged1---4years, corre-spondingto36% ofthesample,followedbytheage group 5---19years(Fig.1),and53%ofthepatientsweremales.
Perinatal/at birth
Up to 20 years
>20 years
Undefined Age at loss
11%
57% 18%
14%
Figure2 Percentagedistributionofpatientsevaluatedinthe cochlearimplant outpatientclinic according to agerange at hearinglossdiagnosis.
Pre-lingual
Post-lingual
Undefined Language
52% 37%
11%
Figure3 Percentagedistributionofpatientsevaluatedinthe cochlearimplantoutpatient clinic according tothe language status.
The age at diagnosis of hearing loss was the perinatal periodinmostcases(57%),whereasin14%ofcasestheage atdiagnosisofhearinglosswasundetermined(Fig.2).
Of the assessed patients, 52% had pre-lingual hearing loss,37% hadpost-lingual loss,and 11%had an undefined status(Fig.3).
Theage atfirstconsultationat thehearinghealth out-patientclinicwasmostlybetween1and4years,andonly 3% of the patients were younger than 1 year (Fig. 4). In thegroupofpre-lingualpatients,themeanageatthefirst consultationforhearinghealthassessmentwas3.8years.
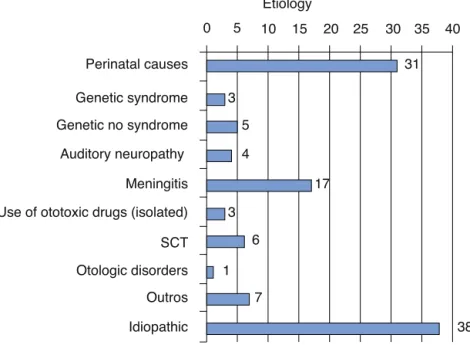
Of the115 assessed patients,31 had nodefinedcause forthehearingloss(33%).Themostfrequentknowncauses wereofperinatalorigin(27%)andmeningitis(15%),asshown inFig.5.
<1 year
1-4 years
5-19 years
20-40 years
Undefined Age at the first consultation
42%
15% 13%
17%
10% 3%
>40 years
3
3 5
4
17
6
7
38 31
0
Perinatal causes
Genetic syndrome
Genetic no syndrome
Auditory neuropathy
Meningitis
Use of ototoxic drugs (isolated)
SCT
Otologic disorders
Outros
Idiopathic
5 10 15 20 25 30 35 40
1
Etiology
Figure5 Distributionofpatientsevaluatedinthecochlearimplantoutpatientclinicaccordingtohearinglossetiology.
Discussion
Thepresentstudywasconductedintheonlypubliccenter thatperformscochlearimplantsurgeryintheentirestateof RiodeJaneiro,Brazil.Thiscenterstartedcochlearimplant proceduresinJuly2011,andbyMarch2013,32patientshad receivedimplants.
The assessment of candidates for cochlear implants includes stringent selection criteria, as well as complete patienthistory,physicalexaminationorevengenetictests, andimagingstudies,inadditiontoassessmentbya psychol-ogist,aspeechtherapist,andasocialworker.Withallthese data,itwaspossibletoanalyzetheprofileofpatientswith profoundsensorineuralhearinglossevaluatedforcochlear implantationinthisoutpatientclinic.
Correctselection of patientswhowillreceive cochlear implants is essential to attain success, which requires a multidisciplinaryapproach,consistingofseveralstagesand involvinghighcostsandtechnology.Studiesonpatient selec-tioncriteriahighlighttheimportanceofstandardization.7---10 It is necessary, however, that this assessment is per-formedefficientlyand rapidlysothatnotimeislostuntil the surgery, as the period of auditory deprivation influ-ences the performance of patients undergoing cochlear implantation.11---13
Itwasobservedthatmostpatientsfollowedinthis out-patientclinic werechildren between 1 and4 years.Male gender predominance was also observed in other stud-ies performed at the national level, as was an unknown etiology identified as the most common cause of hear-ing loss in the evaluated cases.7,14,15 According to Mehra etal.,16 in a review of severalstudies carriedout in the United States from 1966 to 2007, in 56% of cases, the etiology of hearing loss was unknown. Among the known etiologies,geneticcauseswerethemostprevalent.Thisis thesame conclusion of an Australianstudy carriedout in 2003.17
A study carried out in Nicaragua showed preventable causes of hearing loss as an important etiology in non-industrializedcountries.18Inagreementwithdataobserved byPedrettandMoreira,15 perinatalcauses,i.e.,relatedto prematurity, neonatal ICU stay, low birth weight, neona-talhypoxia,hyperbilirubinemia,andconsanguinitywerethe mostprevalentknownetiologyinthepresentsample, with-out considering the use of ototoxic drugs, which in most cases are associated and are also, by themselves, a risk factor for hearing impairment. In other national studies, maternalrubellawasfoundtobethemainknownetiology fortheassessedhearingimpairments;7,14,19however,inthis study,nopatientswiththisetiologywereidentified.
Thisfactcanbejustifiedbyadequatecontrolofmaternal rubella,basedonvaccinationcampaignsforrubella imple-mentedinourstate,whichin2008includedmenandother susceptible groups, and according to data from DATASUL, vaccinationcoverageremainshigh.20However,itmaybedue tofailureintheidentificationandreportingof individuals withcongenitalrubellasyndrome,causingthesecasestobe allocated in groups withhearing loss of unknown or peri-natal cause.This raises questionsregarding the adequacy ofepidemiologicalsurveillancepolicies,andthe identifica-tionand reportingofsuspectedor confirmed casesof the disease.
Meningitiswasthethirdmostprevalentetiologyof hear-ingloss,whichcomprised15%ofthepresent sample.This is also shown in other studies as an important cause of severe/profoundhearingloss,14,15,21 anddepending onthe degreeofcochlearossification,itcancreateachallengeto theintroductionoftheimplantduringsurgery.22
specializedhearinghealthcareserviceshouldbeperformed assoonasthehearinglossisdetected,inordertoprevent social,emotional,andintellectualimpairment.
According toLeal,7the pre-andperi-lingualage range thatbenefitsthemostfromcochlearimplantis0---3years. In case of early intervention, these children can develop languageandcommunicationskillswithasignificantimpact ontheirqualityoflife.ABrazilianstudyassessedthe com-municative skills in children undergoing cochlear implant throughatranslatedand culturally adaptedquestionnaire answered by parents. It was concludedthat the cochlear implanthadapositiveeffectonqualityoflifeofpatients andtheirfamilies,andthatlexicaldevelopmentisthe fac-tor most associated.23 Other studies have shown similar results.11,24
Patientswithpost-lingualhearingimpairmentalsohave important functional outcomes withthe implant. A study evaluating post-lingual patients ten years after surgery showedapositiveimpact;allassessedpatientshadfinished college/universityandwereemployed.25
However,basedontheresultsofthisstudy,thereferral ofthesepatientsortheiraccesstoprimarycareappearsto be deficient, and thus their first consultation at the spe-cialized service will be delayed. This indicates the lack of dynamism of Brazil’s public health care system, which has few specialized centers for the assessment of possi-blecandidatesforcochlearimplantsinconsiderationofthe demands of this typeof disability, and it raises questions regarding the organization of the referral and counter-referral system for patientstreated in hearinghealthcare centers.
Itshouldbeconsidered,especiallyinacontextsuchas thatof hearinghealth, which involvescomplexand inter-disciplinary planning and technology, how the process of referralandmonitoringofpatientspreviouslyidentifiedas havingadisabilitycanbemademoreefficient.Thisinvolves improvedmanagementandbettercommunicationbetween centers.Currently,computerizedsystems,usedtoorganize the priority cases,are definitely feasible as asolution to solvetheaforementionedproblem.
Conclusion
Patientswithprofound sensorineuralhearingloss assessed for cochlear implant present for the first consultation at anagegreaterthan1year(withadistressingmeanof3.8 yearsinthepre-lingualgroup,whichcorrespondsto52%of assessedpatients),eventhoughthelossisdiagnosedatbirth orintheperinatalperiod.Thisreflectsanalreadydeficient healthcaresystemwithrespecttopromptreferralofthese patientstothetertiaryservice.
Idiopathicetiologyofhearinglosswasstillthemost com-monly identified, which indicates alimitation in terms of diagnosis.Themostfrequentknowncauseswereperinatal causesandmeningitis.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Instituto Brasileiro de Geografia e Estatística --- IBGE Atlas
do Censo Demográfico 2010. Rio de Janeiro: IBGE; 2013
[http://www.ibge.gov.br].
2.MinistériodaSaúdeDiretrizesdeAtenc¸ãodaTriagemAuditiva
Neonatal. Brasília:Ministério da Saúde; 2012 [http://bvsms.
saude.gov.br/bvs/publicacoes/diretrizesatencaotriagem auditivaneonatal.pdf].
3.Vespoli S, Marques M, Marane SSG, Santos VF, Chung Man Chin, SantosJL.Análise dasprevalências de doenc¸as detec-tadaspeloprogramanacionaldetriagemneonatalnomunicípio de Araraquara no ano de 2009. Rev CiêncFarm Básica Apl. 2011;32:269---73.
4.Yoshinaga-ItanoC,SedeyAL,CoulterDK,MehlAL.Languageof earlyandlateridentifiedchildrenwithhearingloss.Pediatrics. 1998;102:1161---71.
5.MinistériodaSaúde.Portaria587de2004.Brasília:Ministério
daSaúde;2004[http://dtr2001.saude.gov.br/sas/PORTARIAS/
Port2004/PT-587.htm].
6.Associac¸ão Brasileira de Otorrinolaringologia e Cirurgia
Cérvico-Facial --- ABORLCCF. Critérios de indicac¸ão para
implantecoclear.São Paulo: ABORLCCF;2011 [https://www.
aborlccf.org.br].
7.Leal AF.Triagemde pacientespara implantecoclear através de questionário on-line Perfil do grupo de pacientes pré e peri linguais não convocados. Arq Int Otorrinolaringol. 2010;14:184---91.
8.GoffiGomezMVS.Critériosde selec¸ãoeavaliac¸ão médicae audiológicadoscandidatosaoimplantecoclear:Protocolo HC-FMUSP.ArqIntOtorrinolaringol.2004;8:303---23.
9.CostaFoAO,BevilacquaMC,MoretALM.Critériosdeselec¸ãode crianc¸ascandidatasaoimplantecocleardohospitaldepesquisa ereabilitac¸ãodelesõeslábios-palatais---USP.RevBras Otorrin-olaringol.1996;62:306---13.
10.Bento RF, Sanchez TG, Brito RV. Critérios de indicac¸ão de implantecoclear.ArqIntOtorrinolaringol.1997;1:66---7.
11.StuchiRF, NascimentoLT, BevilacquaMC,BritoNetoRV. Lin-guagemoral decrianc¸as comcinco anosdeusode implante coclear.Pró-FonoRAtualCient.2007;19:167---76.
12.Geers A. Factors affecting the developmentof speech, lan-guage,andliteracyinchildrenwithcochlearimplantation.Lang SpeechHearServSch.2002;33:172---83.
13.BevilacquaMC,FormigoniGMP. Odesenvolvimentodas habil-idades auditivas. In: Bevilacqua MC, Moret ALM, editors. Deficiênciaauditiva:conversandocomfamiliarese profission-ais de saúde, 11. Pulso: São José dos Campos; 2005. p. 179---201.
14.Calháu CM, Júnior LR, Reis AM, Capistrano AK, LimaDdo V, Calháu AC, et al. Etiologyprofile of thepatients implanted in the cochlear implant program. Braz J Otorhinolaryngol. 2011;77:13---8.
15.PedrettMS,MoreiraSC.Profileofcochlearimplantusersofthe cityofManaus.IntArchOtorhinolaryngol.2012;16:452---9.
16.Mehra S, Eavey RD, Keamy Jr DG. The epidemiology of hearing impairment in the United States: newborns, chil-drenandadolescents.OtolaryngolHeadNeckSurg.2009;140: 461---72.
17.RussSA,PoulakisZ,BarkerM,WakeM,RickardsF,SaundersK, etal.EpidemiologyofcongenitalhearinglossinVictoria.Aust IntJAudiol.2003;42:385---90.
18.SaundersJE, Vaz S,GreinwaldJH, LaiJ, Morin L, MojicaK. PrevalenceandetiologyofhearinglossinruralNicaraguan chil-dren.Laryngoscope.2007;117:387---98.
20.Ministério da Saúde/SVS --- Sistema de Informac¸ões do
Pro-gramaNacionaldeImunizac¸ões(SI-PNI).F.13Coberturavacinal.
http://tabnet.datasus.gov.br/cgi/tabcgi.exe?idb2006/f13.def
21.MartinsMBB,LimaFVF,JúniorRCS,SantosACG,BarretoVMP, Jesus EPF.Cochlear implants: our experience and literature review.IntArchOtorhinolaryngol.2012;16:476---81.
22.BevilacquaMC,MoretALM,FilhoOAC,NascimentoLT,Banhara MR.Implantescoclearesemcrianc¸asportadorasdedeficiência auditiva decorrentede meningite.Rev BrasOtorrinolaringol. 2003;69:760---4.
23.TavaresTF, Lopes DB, BentoRF, Andrade CRF. Childrenwith coclearimplants:communicationskillsandqualityoflife.Braz JOtorhinolaryngol.2011;78:15---25.
24.AngeloTCS,BevilacquaMC,MoretALM.Percepc¸ãodafalaem deficientesauditivospré-linguaisusuáriosdeimplantecoclear. Pró-FonoRAtualCient.2010;22:275---80.