F. L. Mitchell’
Simple, trouble-free laboratory instruments are proposedfor use in area-s where heat, humidity, irregular power su$#ly, and inadequate maintenance service #resent #roblems in connection with sofihisticated equipment.
The advances that have taken place so far in the short history of clinical chemistry have unfolded almost entirely in countries with highly developed technologies and economies. And it would appear that there has been an accelerating tendency toward increased sophistication and escalating costs.
Until 1974, for example, in the Division of Clinical Chemistry at the Clinical Research Center in London, a major part of the research effort was concentrated on the development of multichannel analyzers controlled by high-speed computers. Al- though this approach might help to meet the needs of the highly sophisticated laboratories in the developed world, it is completely out of place for developing countries, which, taken together, account for some 80 to 90 per cent of the world’s population. It is not even appropriate for a number of laboratories in some of the highly developed countries. For example, West Germany has over 30,000 clinical chemistry laboratories, most of them asso- ciated with the offices of general practi- tioners, for which purposes the main need is for systems that are simple, reliable, sturdy, and inexpensive. It is debatable whether medical care is always best served by complex and costly laboratory equipment. Moreover, many laboratories with such
IPaper presented at Symposium on Evaluation of Clinical Laboratory Automation (Mexico City, 5 March 1976); also appearing in Bol Of&&t Panam 81 (3): 224-231, 1976.
2Division of Clinical Chemistry, Clinical Research Center, Harrow, Middlesex, England.
installations are becoming cost-conscious. Thus, on the basis of these considerations, the Division’s policy was reoriented some two years ago.
To study the problem in typical develop- ing countries, the deserts and tropical rain forests of Africa were visited. The situations found were not very encouraging. Many of the conditions taken for granted in the developed countries were lacking: regular supply of electricity, reasonable climate, well-trained technicians both to operate and repair equipment, good maintenance ser- vice available on short call, a reliable and efficient supply of reagents, and, above all, reasonable financial resources to cover the cost of equipment and the laboratory’s services generally. The relative absence of these conditions, however, does not mean that it is impossible to carry out clinical chemistry in these areas. What it means is that we are having to return to the drawing board and redesign instruments and sys- tems, to rethink our chemistry.
In most of the developing countries there appear to be four strata of medical care, either already in being or in the process of consolidation :
l First, at the strictly local level there is
the dispensary serving a small group of people and manned by a person comparable to the Chinese “barefoot doctor” with perhaps six months of medical training.
l Second, there is the community hospi-
tal, with up to 50 beds, where minor surgery might be carried out, which has either a
Mitchell l SIMPLIFIED LABORATORY INSTRUMENTS 213
doctor or more highly trained “barefoot”- type doctor in charge.
b Third, there is the district, area, or central hospital, which is relatively sophis- ticated and capable of carrying out the major medical needs of the community.
l Finally, there is the teaching hospital,
which has a high degree of sophistication. At the level of the local dispensary, it is not likely that laboratory facilities would be needed, but from the community hospital upward, to one degree or another they should definitely be available.
It is at the level of the community hospi- tal that we have given the problem most thought. Here only the very basic necessities are likely to be required: a refrigerator, for general purposes and for keeping vaccines, etc. ; a very simple microscope for the detection of parasites; simple culture facili- ties: and, finally, a simple calorimeter for the measurement of hemoglobin, urea, protein, bilirubin, and glucose.
The World Health Organization has indicated an urgent need for a suitable simple calorimeter, for which rough speci- fications have been drafted by hematologists and clinical chemists. Such a calorimeter should, if possible, cost less than US$lOO.OO, consume a minimum amount of electricity, be sturdy, have a reasonable guarantee of trouble-free operation for up to five years, and be capable of operation in extremes of heat and humidity and in dusty atmo- spheres.
The instruments that are currently in use in the circumstances envisaged are entirely unsuitable. Most often they are found to be broken down and totally out of working order. They usually have a barrier-layer light-detector cell which might last as few as seven days in a humid atmosphere; they have a rheostat which either rots in a humid atmosphere or becomes clogged with dust in desert conditions. The gelatin filter is also highly vulnerable to tropical humidity and temperatures. They have an electric bulb which consumes a considerable amount of
power, has a relatively short life, and is difficult to change because of the realign- ment necessary. The galvanometer has a pivot which can easily rust or break.
It should be possible to design an instrument that eliminates all these draw- backs. The question of their elimination had never arisen in the past, which is reason alone for us not to have furnished any concrete solutions heretofore.
It has been said that the Lovibond (Tintometer) system might provide the answer. In this system the colored test solution is compared by eye with colored glasses of graded densities mounted on rotatable discs. For
various
reasons, how- ever, this approach cannot be recommended as a lasting answer to the problems being considered. One of the main disadvantages is that, except in hemoglobinometry, it is difficult to ensure that “like” colors are being compared; moreover, measurement is step-wise and not continuous.A grey wedge instrument-still using the human eye for balancing-is slightly better. It has a continuous scale instead of the stepped operation of the colored glass instrument. Such a calorimeter has
been
found suitable in the past for the measure- ment of hemoglobin, and indeed it would still be favored by many if the cost of modern labor were not such as to make the price of the glass grey wedges prohibitive. Efforts to replace the wedges by photo- graphic film giving a similar effect have,somewhat
surprisingly, indicated an evengreater cost.
Figure 1. The need for a simple calorimeter to measure hemoglobin, urea, protein, bilirubin,
and
glucose may be answered by the battery-o#erated
monochromatic
absor@tiometer. Inexpensive, easy
to ofierate, and trouble-free in terms of maintenance, it
ismade to hold up the adverse climatic
conditions such as heat, humidity,
and dust.
since the LED
operates
by flashing,
the
current
consumption
from
its integral
battery is so small that battery life is almost
the
same
as normal
shelf
life.
The
instrument
is simple to operate and suitable
for
use in
adverse
climatic
conditions.
Encapsulation
of electronic
and
optical
parts
would
ensure
that,
apart
from
a
catastrophe,
it should
remain
functional
almost indefinitely.
The galvanometer
has always
been an
integral
part of any photoelectric
colori-
meter, and a problem
in the past has been
the corrosion
of the pivot mechanism.
The
taut band movement
now available
for use
in the MONA
is much more robust, and the
entire
mechanism
can be sealed against
humidity
and dust.
On the basis of our
discussions
with
actual and potential
users in many coun-
tries,
it
would
appear
that
such
an
instrument
need basically measure, only five
substances-namely,
hemoglobin,
urea,
protein,
bilirubin,
and glucose. (If it is also
to be used in developed
countries,
choles-
terol might be added to the list.) Simple and
robust
chemistries
are selected compatible
with the single wavelength
emitted
by the
LED, with no loss of accuracy.
A calorimeter
is of little
value
if the
simplicity
of its use cannot be extended
to
the collection
of blood from the patient.
A
syringe should be avoided if at all possible.
Disposable
syringes
are costly,
and
the
Mitchell l SIMPLIFIED LABORATORY INSTRUMENTS 215
the conditions being considered.
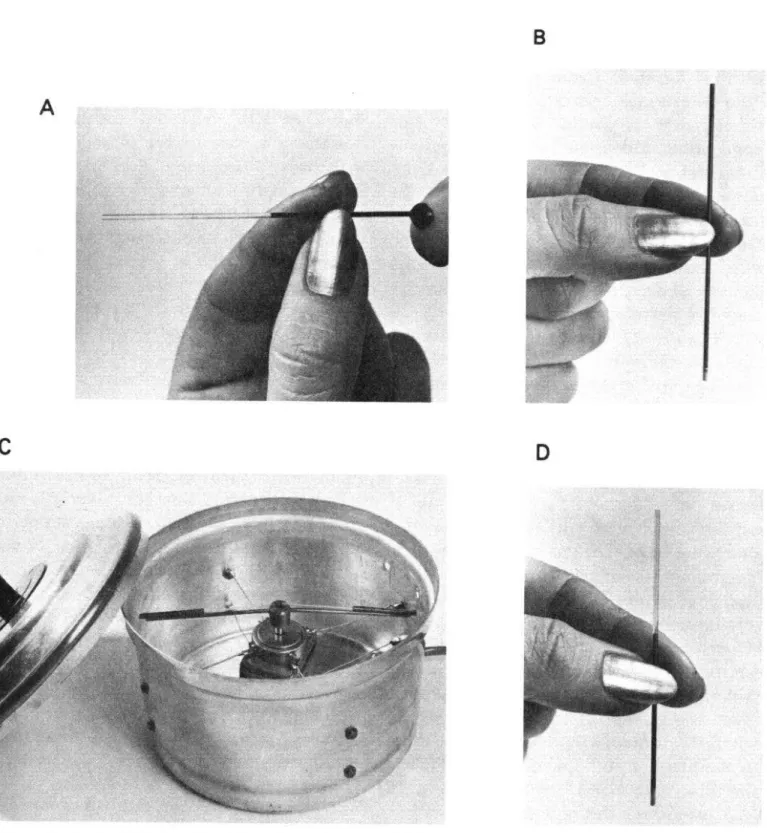
An interesting answer developed at the Clinical Research Center has been termed “the swizzlestick technique,” and it is so simple that it could have very wide application. Blood is collected in capillary tubes such as those used for hematocrit deter - minations (Figure 2-A); 100 or 200 ~1 can be taken in this way from a prick in a finger, ear, or heel. One end of the tube is sealed with plasticine (Figure 2-B), as for the hematocrit determination, and the tubes are placed in a simple centrifuge (Figure 2-C), which can easily be made out of a saucepan and a 12-volt motor. After the samples have been centrifuged (Figure 2-D), the meniscus of the serum in the tube is made level with the end of the capillary, if necessary, by gently plugging with additional plasticine.
The swizzlestick itself (Figure 2-E), consists of a handle fastened to a small stainless steel platform on which is also attached a small stainless steel wire measur- ing probe whose diameter is slightly smaller than that of the capillary tube and whose volume corresponds exactly to the amount of serum required for the assay. The capillary is placed on the measuring probe of the swizzlestick (Figure 2-F) and pressed down to the plate. A small drop of serum equal in volume to that of the probe gathers on the plate, and the whole swizzlestick is now placed in the reaction tube (Figure 2-G), into which the appropriate amount of diluent or reagent has previously been placed. The stick is swizzled in order to mix the contents of the tube and then with- drawn. The capillary can be cut shorter and its contents used for several determinations. The diameter and length of the wire probe can be varied to cover volumes from 5 to 20 1.11 at least (Figure 2-H).
The precision and accuracy of the dilution have been shown to be equal to, or better than, those obtained using some of the best micropipettes, and an inexperienced laboratory worker has no difficulty in obtaining excellent results.
The calorimeter and blood collection system described should be suitable in the context of medical care in the remotest of areas. It is hoped that a use for them will be found at all levels, but in the district hospital a higher degree of sophistication will also be necessary. For this purpose, simple sturdy instruments for automation on a limited scale are required. The cost of installing and maintaining the type of equipment which is commonly used in developed countries can be prohibitive, and again, operability under adverse climatic conditions is not usually a feature of its design.
Electricity supply is an extremely impor- tant consideration. Even if the frequency is right for a particular instrument, the voltage variation can cause problems, and long and frequent interruptions in service are likely to occur. There is therefore much to be said for standardizing on a supply of 12 volts DC. Vehicles with 6- or 12-volt batteries are in use in most of the developing countries, and a 12-volt accumulator can always be charged from hospital electric power source (albeit erratic), an automo- bile, or even a manually or wind-driven generator. The components of modern electronic instruments operate on low voltages, and few items of laboratory equipment-even the complicated ones- require a high-voltage supply.
A
D
Figure 2. A simplified
method for the collection of blood samfiles uses cafi’llary tubes. After the
patient’s finger has been picked
(A), one end of the tube
issealed with plasticine (B). Following
centrifugation
in an adapted saucepan (C), the level
of
the serum in the tube is adjusted with
additional plasticine (0).
dealt with in a way similar
to the swizzle-
microscopes
for use in such circumstances
stick-type
approach,
the counting
done in a
has almost certainly
not yet been designed.
very simple rugged Coulter-type
instrument.
One can envisage an extremely
inexpensive
One of the main
tasks of pathology
in
prefocused
instrument
that would
afford
developing
countries
is the detection
and
just sufficient
magnification
for the pur-
identification
of parasites,
for
which
a
poses required,
with
plastic
lenses
to
6
Mitchell
lSIMPLIFIED LABORATORY
INSTRUMENTS
217
E
Unfortunately, development of the right efficient supply of the simple hardware and instruments and the right techniques is chemicals required and of the manpower perhaps the smallest and easiest task in the competent to use them. These deficiencies overall introduction of laboratory facilities can be bridged only through the whole- on a truly worldwide basis. The major hearted cooperation of the international problems lie in the training of staff and in organizations and associations existing in the establishment of an organized and the respective branches of pathology.
ACKNOWLEDGMENTS
Thanks are due to the team at the Clinical Research Center responsible for the developments reported. This includes Mr. S. Pocock of the Center’s Division of Bioengineering, Dr. S. S. Brown, and Messrs. A. Renshaw, J. R. Rideout, and M. Snook.
SCHISTOSOMIASIS ON THE INCREASE’
The debilitating disease of schistosomiasis, already affecting 200 million people in more than 70 countries, is on the increase throughout the world. A report to the Twenty-ninth World Health Assembly declared: “Schistosomiasis is spreading and its severity is increasing. Although direct mortality from infection is low, the importance of the disease lies in the sheer size of the epi- demiologic phenomenon.” As the human population grows, the problem intensifies on two counts-increased excretal pollution of water, and the extension of land areas placed under irrigation for agricultural purposes. In addition, the creation of man-made lakes contributes to spread of the disease.
Since no one drug has so far proven effective and efforts to develop a vaccine have not yet succeeded, existing control meas- tires concentrate on killing the snail hosts, preventing contact with infected water through the provision of alternative domestic supplies, and improving sanitary facilities.
A resolution approved by the Assembly in committee called on WHO to expand its activities in this field and urged those countries in which schistosomiasis is or could become endemic to undertake specific measures to prevent its spread.