VIEWS AND REVIEWS DOI: Xxxxxxxxxxxxxxxxxxxxx
Treatment of neuromyelitis optica:
an evidence based review
Tratamento da neuromielite óptica: uma revisão baseada em evidências
Douglas Sato1,2, Dagoberto Callegaro2, Marco Aurélio Lana-Peixoto3, Kazuo Fujihara4, on behalf of Brazilian
Committee for Treatment and Research in Multiple Sclerosis (BCTRIMS)
Neuromyelitis optica (NMO) is an inlammatory dis-ease of the central nervous system (CNS) characterized by severe optic neuritis (ON) and transverse myelitis (TM)1.
Aquaporin-4 (AQP-4) antibody, also known as NMO-IgG, an autoantibody exclusively detected in the sera of NMO, is di-rected against AQP-4, a water channel richly expressed on foot processes of astrocytes in the CNS2,3. In most series of
1 Department of Neurology, Tohoku University Graduate School of Medicine, Sendai, Japan;
2 Department of Neurology, Faculty of Medicine, University of São Paulo (USP), São Paulo SP, Brazil;
3 CIEM Multiple Sclerosis Research Center, Federal University of Minas Gerais Medical School, Belo Horizonte MG, Brazil;
4 Department of Multiple Sclerosis Therapeutics, Tohoku University Graduate School of Medicine, Sendai, Japan.
Correspondence: Douglas Sato; Department of Neurology; Tohoku University Graduate School of Medicine; 1-1, Seiryomachi, Aobaku; 980-8574 Sendai Miyagi - Japan; E-mail: [email protected]
Conflict of interest: There is no conflict of interest to declare. Received 29 August 2011; Accepted 05 September 2011
ABSTRACT
Neuromyelitis optica (NMO) is an inflammatory disease of the central nervous system characterized by severe optic neuritis and transverse myelitis, usually with a relapsing course. Aquaporin-4 antibody is positive in a high percentage of NMO patients and it is directed against this water channel richly expressed on foot processes of astrocytes. Due to the severity of NMO attacks and the high risk for disability, treat-ment should be instituted as soon as the diagnosis is confirmed. There is increasing evidence that NMO patients respond differently from patients with multiple sclerosis (MS), and, therefore, treatments for MS may not be suitable for NMO. Acute NMO attacks usually are treated with high dose intravenous corticosteroid pulse and plasmapheresis. Maintenance therapy is also required to avoid further attacks and it is based on low-dose oral corticosteroids and non-specific immunosuppressant drugs, like azathioprine and mycophenolate mofetil. New therapy strategies using monoclonal antibodies like rituximab have been tested in NMO, with positive results in open label studies. However, there is no controlled randomized trial to confirm the safety and efficacy for the drugs currently used in NMO.
Key words: neuromyelitis optica, therapy, aquaporin 4, plasmapheresis, steroids, azathioprine, mycophenolic acid, monoclonal antibodies, mitoxantrone, cyclophosphamide, interferon-beta.
RESUMO
Neuromielite óptica (NMO) é uma doença inflamatória do sistema nervoso central caracterizada por grave neurite óptica e mielite transver-sa, com um curso usualmente recorrente. O anticorpo contra aquaporina-4 é positivo em grande porcentagem dos pacientes com NMO e se liga a este canal de água altamente expresso nos processos pediosos dos astrócitos. Devido à gravidade dos ataques de NMO e ao elevado risco de incapacidade, o tratamento deve ser instituído tão logo o diagnostico seja confirmado. Existem evidências crescentes de que pa-cientes com NMO respondem de forma diferente dos papa-cientes com esclerose múltipla (EM) e, portanto, os tratamentos utilizados na EM podem não ser adequados para NMO. Os quadros agudos de NMO são tratados com pulsos de corticosteroides em altas doses e plasmafé-rese. O tratamento de manutenção também deve ser instituído para evitar ataques subsequentes e é baseado em corticosteroides orais em baixas doses ou imunossupressores, como a azatioprina e o micofenolato mofetil. Novas estratégias de tratamento utilizando anticorpos monoclonais como rituximab têm sido avaliadas para NMO, com resultados positivos em estudos abertos. Entretanto, não existem estudos clínicos controlados, randomizados, para confirmar a segurança e eficácia dos tratamentos atualmente utilizados na NMO.
Palavras-Chave: neuromielite óptica, terapia, aquaporina 4, plasmaferese, esteróides, azatioprina, ácido micofenólico, anticorpos monoclonais, mitoxantrona, ciclofosfamida, interferon-beta.
NMO, more than half of cases are positive for AQP-4 antibody. In 2006, Wingerchuk et al.4 proposed the revised diagnostic
diagnostic criteria for multiple sclerosis (MS); (3) serum posi-tivity for AQP-4 antibody.
NMO treatment has two main objectives: one is to con-trol the inlammatory damage in acute attacks and the other one is a maintenance treatment to avoid relapses. he former is based on high dose intravenous corticosteroids and plas-mapheresis5; the latter is based on low-dose corticosteroids
and immunossupressants6,7. Additionally, there is evidence
that AQP-4 antibody titers are reduced in patients without relapses under immunosuppressant treatment8,9. Although
NMO attacks are related to severe disability, there are some evidences that NMO patients remain neurologically stable between them, without evidence of progressive deterioration like in MS1. herefore, it is crucial that treatment is started as
early as possible to avoid new relapses and further disability. For this review, the English-language literature was system-atically searched using Pubmed (National Library of Medicine) with the keywords neuromyelitis optica, and treatment was accessed on 20th July 2011, resulting in 394 articles. All articles
available had the abstract analyzed and full article review was performed once considered relevant. Additional articles refer-enced in bibliographies from these articles were also reviewed. Case reports that revealed further insights into NMO, not iden-tiied in case series analyzed, were included in this review.
LEVELS OF EVIDENCE
In this review, we used levels of evidence from the Agency for Health Care Policy and Research (also known as Agency for Healthcare Research and Policy)10 (Table 1) and the
recommen-dation grades published for use in clinical guidelines from the American College of Chest Physicians Task Force (Table 2)11. We
have classiied the available studies in NMO accordingly and provided the recommendations for each treatment (Table 3).
CORTICOSTEROIDS
Corticosteroids have been the mainstay treatment for NMO in both acute and maintenance phase. Methylprednisolone has been used since 1970 as a potent anti-inlammatory or im-munosuppressant agent in the treatment of a variety of diseas-es including those of hematologic, allergic, inlammatory, neo-plastic and autoimmune origin. In addition, it is also widely used in prevention and treatment of graft-versus-host disease following allogeneic bone marrow transplantation and acute spinal cord injury. Corticosteroids exert a wide array of physi-ologic efects including modulation of carbohydrate, protein and lipid metabolism, and maintenance of luid and electrolyte homeostasis. Moreover, cardiovascular, immunologic, muscu-loskeletal, endocrine and neurologic physiologic functions are inluenced by corticosteroids. herefore, not only the positive
efects can be observed, but also many adverse events can be originated from corticosteroids use. hese adverse events can be seen acutely like mood/psychic changes, luid retention with circulatory overload, hyperglycemia, hypokalemia and in-creased ocular pressure. Chronic corticosteroid use may pro-mote other side efects like hypertension, hirsutism, Cushing’s syndrome, hyperlipidemia, diabetes mellitus, gastrointestinal hemorrhage, aseptic necrosis and bone fractures.
he mechanism of action of corticosteroids is not com-pletely understood, but many of their genomic functions orig-inate from regulation of gene expression subsequent to bind-ing speciic intracellular receptors and translocation into the nucleus12. More recently, there have been observed evidences
that corticosteroids in high doses, as used in high dose intra-venous methylprednisolone (HIMP), have signiicant non-ge-nomic efects, which may explain the rapid clinical response after infusion. hese efects are probably mediated by a direct efect on cellular membranes and mitochondrial function, in-ducing a reduction of adenosine-5’-triphosphate production and promoting cellular apoptosis. Furthermore, HIMP also reduces the mitogen-induced increase of cytoplasmic calci-um concentration and inhibits cation cycling across the plas-ma membrane with only a miniplas-mal efect on intracellular protein synthesis. he genomic and non-genomic efects may explain the positive efects of corticosteroids in NMO, induc-ing a reduction of inlammation, apoptosis of leukocytes, sup-pression of migration of polymorphonuclear leukocytes and reversal of increased capillary permeability.
Although the clinical eicacy of corticosteroids have been established in meta-analysis evaluating the treatment of neuroimmunological diseases13, only few clinical studies
have rigorously investigated the eicacy and safety of cor-ticosteroids in NMO. Consequently, the current practice of corticosteroids use in NMO is mainly based on few open-la-bel studies and personal experience on treating other CNS autoimmune diseases.
he irst open-label study in NMO evaluated the treatment of seven newly diagnosed NMO patients with long-term pred-nisone and azathioprine, with a follow-up every two months for at least 18 months6. Patients had no relapses during the
ob-servation period, and Expanded Disability Status Scale (EDSS) reduced from a mean of 8.2 at baseline to 4 at 18 months. A subsequent study reviewed related 25 patients with NMO who met the 1999 Wingerchuk’s criteria and identiied nine patients with long-term use of corticosteroid monotherapy7. he
Another evidence that corticosteroids are useful to pre-serve normal nerve function in NMO is a retrospective study on NMO patients with optic neuritis relapse, which correlat-ed the number of relapses, early corticosteroids intervention and a loss in retinal nerve iber layer thickness (RNFLT)14. he
overall RNFL was thinner in patients in the NMO group than in the MS (63.84 vs. 84.28 μm). he frequency of the ON
re-lapses and the time for beginning the treatment with HIMP signiicantly afected the preservation of the RNFLT.
PLASMAPHERESIS
Plasmapheresis (PE) has been used as an alternative ther-apy for autoimmune diseases when HIMP is not efective. PE
Table 1. Classification of evidence levels10.
Ia Evidence obtained from meta-analysis of randomized controlled trials
Ib Evidence obtained from at least one randomized controlled trial
IIa Evidence obtained from at least one well-controlled study without randomization
IIb Evidence obtained from at least one other type of well-designed quasi-experimental study
III Evidence obtained from well-designed, non-experimental descriptive studies; such as comparative studies, correlation studies and case control studies
IV Evidence obtained from expert committee reports or opinions and/or clinical experience of respected authorities
Table 2. Grading recommendations11.
Recommendation Description Methodological quality of supporting evidence Implications Grade 1A Strong recommendation,
high-quality evidence
RCTs without important limitations or
overwhelming evidence from observational studies
Strong recommendation, can apply to most patients in most circumstances without reservation Grade 1B Strong recommendation,
moderate-quality evidence
RCTs with important limitations (inconsistent results, methodological flaws, indirect or imprecise) or exceptionally strong evidence from observational studies
Strong recommendation, can apply to most patients in most circumstances without reservation
Grade 1C Strong recommendation, quality or very low-quality evidence
Observational studies or case series Strong recommendation, but may change when higher quality evidence becomes available Grade 2A Weak recommendation,
high-quality evidence
RCTs without important limitations or
overwhelming evidence from observational studies
Weak recommendation, best action may differ depending on circumstances or patients or societal values
Grade 2B Weak recommendation, moderate-quality evidence
RCTs with important limitations (inconsistent results, methodological flaws, indirect or imprecise) or exceptionally strong evidence from observational studies
Weak recommendation, best action may differ depending on circumstances or patients or societal values
Grade 2C Weak recommendation, quality or very low-quality evidence
Observational studies or case series Weak recommendation, other alternatives may be equally reasonable
RCT: Randomized controlled trial.
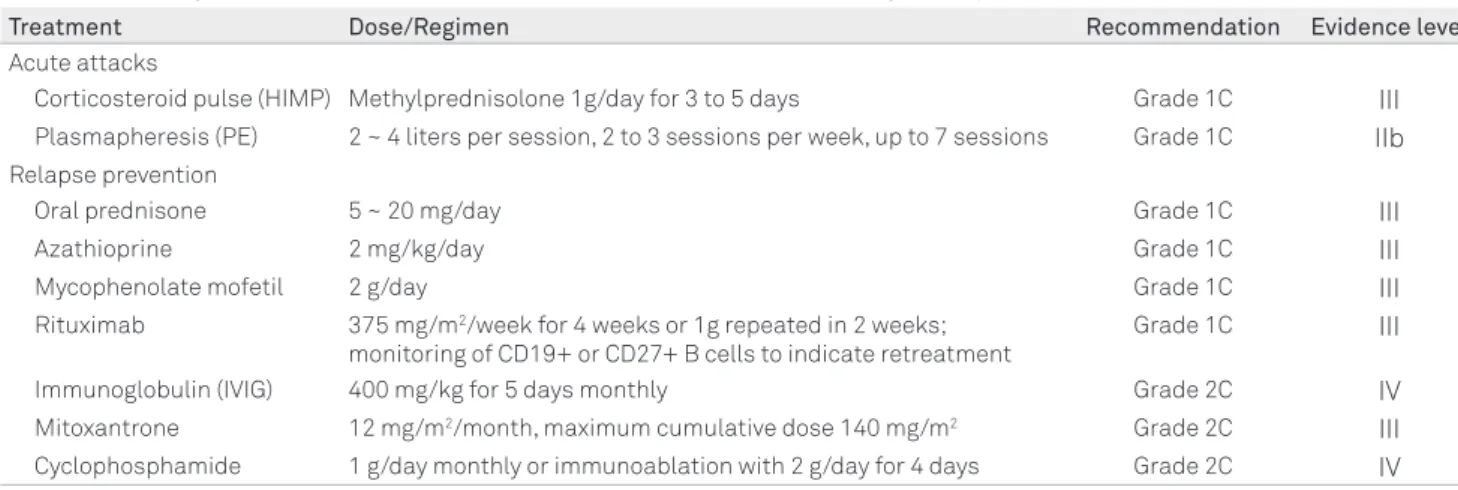
Table 3. Summary of treatments and recommendation levels used for neuromyelitis optica.
Treatment Dose/Regimen Recommendation Evidence level
Acute attacks
Corticosteroid pulse (HIMP) Methylprednisolone 1g/day for 3 to 5 days Grade 1C III
Plasmapheresis (PE) 2 ~ 4 liters per session, 2 to 3 sessions per week, up to 7 sessions Grade 1C IIb
Relapse prevention
Oral prednisone 5 ~ 20 mg/day Grade 1C III
Azathioprine 2 mg/kg/day Grade 1C III
Mycophenolate mofetil 2 g/day Grade 1C III
Rituximab 375 mg/m2/week for 4 weeks or 1g repeated in 2 weeks; monitoring of CD19+ or CD27+ B cells to indicate retreatment
Grade 1C III
Immunoglobulin (IVIG) 400 mg/kg for 5 days monthly Grade 2C IV
Mitoxantrone 12 mg/m2/month, maximum cumulative dose 140 mg/m2 Grade 2C III Cyclophosphamide 1 g/day monthly or immunoablation with 2 g/day for 4 days Grade 2C IV
is an extracorporeal blood puriication technique designed to remove antibodies, complement, cytokines and chemok-ines from the plasma. he quick removal of these substances may reduce further damage and interrupt the advancement of lesions faster than immunosuppressive agents, as autoan-tibodies can persist for several weeks in the circulation. It has been largely used for the treatment of thrombotic thrombo-cytopenic purpura, myasthenia gravis, chronic inlammatory demyelinating polyneuropathy, Waldenstrom macroglobu-linemia and Guillain-Barré syndrome15. MS, NMO, acute
dis-seminated encephalomyelitis, Lambert-Eaton myasthenic syndrome, paraproteinemic polyneuropathy and cryoglobu-linemic polyneuropathy are some other neurological condi-tions sometimes treated with apheresis16. Due to the success
in other immune mediate diseases, PE is used in NMO tak-ing into consideration that there is evidence that NMO is an autoantibody-mediated disease with complement activation and PE has the potential to remove humoral immune prod-ucts from systemic circulation17.
PE is often prescribed using at least ive plasma exchange sessions to achieve a suicient antibody removal. he rate of extravascular to intravascular equilibration is approximately one to two percent per hour, then ive separate exchanges over seven to ten days are required to remove 90% of the to-tal initial body immunoglobulin levels18. In order to be most
efective, PE has to be associated with appropriate immuno-suppressant therapy, avoiding new immunoglobulin produc-tion. If antibody production is not properly blocked, addi-tional PE sessions may be required.
PE is an invasive therapeutic procedure and carries some complications. In NMO, it is usually performed using 5% al-bumin replacement, so complications from fresh frozen plas-ma infusion are avoided. Reported adverse efects have been hypotension, dyspnea/pulmonary edema due to luid over-load, citrate induced hypocalcaemia, coagulation abnormali-ties, infection and catheter related issues. As PE can also pro-mote removal from serum of drugs such as azathioprine and cyclophosphamide; it is advisable that these drugs are ad-ministered following apheresis sessions19.
here is some evidence from some case series that PE is efective for acute relapse treatment in NMO patients who did not respond satisfactorily to HIMP5,17,20,21. Moreover,
clini-cal response seems to be related to the early initiation of treat-ment20 and it may be observed quickly once PE sessions are
started5. A review from the American Academy of Neurology
about PE in neurological diseases indicates that there is Class II evidence that PE is probably efective to treat fulminant CNS diseases, including NMO22. However, the randomized
study which provided such evidence included 22 patients with various CNS demyelinating diseases, like MS, ADEM, Marburg’s disease, but only four patients with acute myelitis and two patients with NMO23. Other small case series have
reported positive results with double membrane iltration
plasmapheresis (instead of centrifugation technique)24 and
PE used as rescue therapy 25.
he Guidelines on the use of therapeutic apheresis in clinical practice from the American Society for Apheresis published in 201026 considered that PE for NMO is accepted
as second line therapy, as it may be helpful in recovery from acute attacks, although it does not prevent further relapses.
For long-term treatment, there is only a small case-series study (n=4) indicating that PE is efective not only for acute management, but also intermittent PE may be worthwhile for selected cases where long-term immunosuppressant treatment have failed21.
AZATHIOPRINE
Azathioprine is a DNA synthesis inhibitor, as it is converted to a purine analogue, with interference in the purines synthe-sis (adenine and guanine). It inhibits the proliferation of cells, especially lymphocytes. he clinical efects are usually not seen before three to six months after initiation of therapy. It is a rea-sonably well-tolerated drug used for autoimmune diseases and organ transplantation either alone or in combination. It has been approved as adjunctive therapy in prevention of re-jection of kidney transplants and for the management of active rheumatoid arthritis27. Additionally, many of-label uses have
been reported, such as adjunct in prevention of solid organ transplants rejection, steroid-sparing agent for corticosteroid-dependent Crohn’s disease and ulcerative colitis, dermatomy-ositis/polymyositis, MS and other autoimmune diseases.
Common adverse events reported with azathioprine in-clude: fever, malaise, nausea, vomiting, leukopenia, thrombo-cytopenia, hepatoxicity, myalgia, and infections. It is reported a slight higher risk of developing cancer27. herefore, periodic
monitoring of patients with hematological (complete blood count with diferential and platelets), liver function tests, bili-rubin and continuous surveillance for clinical signs of cancer are required.
More recently, there is increasing evidence to evaluate thiopurine methyltransferase enzyme activity before initiat-ing azathioprine therapy28. hiopurine methyltransferase
en-zyme is involved in the metabolism of azathioprine and may determine the clinical response to thiopurines. Patients with intermediate or low thiopurine methyltransferase activity may be at risk for increased myelosuppression, sometimes life-threatening. herefore, careful monitoring and dose ad-justments may be required for these patients.
As previously described, the irst study included seven newly diagnosed NMO patients with long-term combination of corticosteroids and azathioprine with positive results6.
patients began prednisone tapering very slowly until they have achieved a dose of 10 mg/day and azathioprine doses of 75 to 100 mg/day. Another study observed that suspension of azathioprine was followed by increase in AQP-4 antibody levels and clinical attacks in some patients, together with the interruption of corticosteroid in two patients or the main-tenance of low-dose corticosteroid treatment (5 mg/day)9. A
retrospective study with 36 Brazilian NMO patients analyzed those who used azathioprine alone or in combination with corticosteroids and provided similar indings of reduction in disability and relapse rates29. hese results may indicate
that combination therapy may be required in some patients. However, there are no multicenter controlled studies to pro-vide class I eicacy epro-vidence of this therapeutic regimen, and side efects may limit the use in some patients.
RITUXIMAB
Rituximab is a chimeric monoclonal antibody against the protein CD20, which is primarily found on the surface of B cells and it has the property to eliminate B cells selectively. Rituximab binds to the antigen on the cell surface, activat-ing complement-dependent B cell cytotoxicity. It also binds to human Fc receptors, mediating cell killing through an an-tibody-dependent cellular toxicity. Rituximab is used in the treatment of many lymphomas, leukemias, transplant re-jection and some autoimmune disorders. Besides the clini-cal studies with rituximab, another evidence that B cells and AQP-4 antibody are closely related to NMO pathogenesis is a case report of a Japanese NMO patient with hypogammaglob-ulinemia secondary to carbamazepine who reported no re-lapses during the lowered IgG levels, but who had no attacks relapsed later when the hypogammaglobulinemia resolved in association with the normalization of CD19+ cells30.
he irst published open label study included eight patients in the USA, where rituximab was well tolerated, and positive response was observed in all patients with signiicant relapse reduction (2.6 relapse/patient/year to 0) and recovery of neu-rologic function measured by EDSS from 7.5 to 5.531. Rituximab
was administered in four infusions of 375 mg/m2, administered
once per week, and B cells were monitored with CD19 marker by low cytometry. In the retreatment, the regimen used was 1,000 mg administered two weeks apart. However, one patient who did not receive the repeated course of rituximab when planned had an attack, indicating that treatment requires re-peated infusions in order to CD19+ cells remain undetectable. A report of three Japanese NMO cases who received rituximab also observed positive results, with a remarkable reduction in the annualized relapse rate ( from 5.0 in the pre-treatment to 0.6 in the post-treatment), but the decrease in EDSS was not so signiicant ( from 8.7 in the pre-treatment to 8.0 post-treat-ment), maybe indicating that, although the drug was efective
to control the inlammatory response, the irreversible dam-age had already been established32. Another study described
two NMO cases treated with rituximab33. It was observed a
good clinical response in one patient, but the other one have experienced relapses after the treatment, indicating that not all patients respond so well. A possible explanation for the oc-currence of relapses following initiation of rituximab in some NMO patients is the transient increase in AQP-4 antibody ti-ters and of B cell activating factor levels, which is observed for two weeks following the initial infusion34. Posterior reversible
encephalopathy syndrome after rituximab infusion in NMO have been reported35, but this syndrome has been reported
in NMO patients independent of rituximab36, so this may be a
relapse related to rituximab initiation rather than a new treat-ment complication.
Another study retrospectively analyzed 25 NMO patients identiied in seven centers from USA and Europe35. It was
ob-served a marked reduction in the attacks and improvement in disability. he study had the two regimen of rituximab used in pre-vious studies analyzed together (four infusions of 375 mg/m2,
ad-ministered once per week, and 1,000 mg adad-ministered two weeks apart). he median follow-up was 19 months, and the mean post-treatment relapse rate dropped from 1.7 to 0. Disability has improved in 80% of patients, but two patients died during the study period, one due to a brainstem relapse and the oth-er due to suspected septicemia. he study indicated a prom-ising treatment option, but, like the traditional chemother-apies, it may expose patients to severe infections. Another retrospective study in the USA has also revealed that ritux-imab treatment was associated with reduction of relapses and stabilization or improvement of disability36.
A study with eight European patients evaluated the clini-cal response and AQP-4 antibody titers with diferent treat-ments, measured by a luorescence immunoprecipitation as-say using an extract from cells transfected with EGFP-tagged human AQP-4 M1 and M23 isoforms9. Four patients received
rituximab and the reduction of CD19+ cells was correlated with a reduction of AQP-4 antibody titers and positive clini-cal response. he study also identiied that relapses were pre-ceded or paralleled by reoccurrence of CD19+ cells and an in-crease up to three-fold in the AQP-4 antibody. Another group has also conirmed clinical eicacy of rituximab in 10 NMO patients in Europe, but there was no correlation with AQP-4 antibody levels37.
Recently, the results of an open-label study with Korean NMO patients were reported with positive results38. Induction
therapy was basically the same of previous studies, followed by maintenance therapy with repeated rituximab infusions (375 mg/m2, once) when the frequency of CD27+ memory B
in the mean relapse rate from 2.4 to 0.3 while receiving ritux-imab over 24 months. Seventy percent of patients became relapse-free over 24 months, and disability either improved or stabilized in great majority of patients. One patient con-tinued to have relapses despite rituximab treatment and was switched to mitoxantrone hydrochloride, and another patient had three relapses during treatment, but two relapses were associated with delayed retreatment. AQP-4 antibody levels declined signiicantly following treatment with rituximab, consistent with the clinical response and the efect on memo-ry B cells. he most common infusion-related reactions, not-ed in 40% of patients during the irst infusion, were transient hypotension and mild to moderate lu-like symptoms, such as a febrile sense, headache and skin rash. Less than half of patients experienced at least one infection episode during the study period, but there were no serious infection. here was no decline in serum total IgG titers, and no patient became seropositive for the JC virus over the 24 months.
MITOXANTRONE
Mitoxantrone hydrochloride is an anthracenedione used as an antineoplastic agent for prostate cancer and acute non-lymphocytic leukemia in adults. It has been approved for MS treatment, including secondary progressive MS, based on the evidence that it has reduced progression in MS patients with failure in other treatment regimens. It also reduces the clini-cal relapse rate and MRI outcomes in relapsing-remitting MS patients, and it is helpful on patients with clinical worsening conditions. However, the potential toxicity of this drug limits its use, and patients should be monitored periodically for car-diac, liver and kidney function39.
Considering the successful use in MS, mitoxantrone has been evaluated in NMO patients, but the case series have been very limited. In a study, ive NMO patients received monthly intravenous infusions of mitoxantrone hydrochlo-ride, 12 mg/m2, for six months, followed by three additional
treatments every three months40. During the two years
peri-od of treatment, two patients had a relapse within the initial ive months of treatment (one severe and one moderate), and improvement was seen clinically and on magnetic resonance images in four patients. One patient had a reversible decrease in cardiac ejection fraction. In another study, there were three patients who received mitoxantrone9. Unfortunately, the
re-sponse was variable, from reduction of relapse rate in one pa-tient to increased relapse rate in two papa-tients.
MYCOPHENOLATE MOFETIL
Mycophenolate mofetil has been largely used for the treatment of several autoimmune diseases. It has a selective
cytostatic efect on T and B lymphocytes. It is an inhibitor of inosine monophosphate dehydrogenase, which inhibits de novo guanosine nucleotide synthesis, required for
prolifera-tion of T and B lymphocytes. It has been used for prevenprolifera-tion of organ transplants rejection and autoimmune diseases, like myasthenia gravis and systemic lupus erythematosus.
In 2006, a case report described a NMO patient success-fully treated with mycophenolate mofetil 2 g/day who had no relapses over the following two years associated with clinical improvement41. Another study analyzed retrospectively 24
patients treated with mycophenolate mofetil (median dose of 2 g/day) with median treatment duration of 27 months. Patients had reduction in relapse rates (median annualized rate dropped from 1.28 to 0.09) and 91% of patients had sta-bilization or improvement of disability. In this study, six pa-tients (25%) reported adverse events, which included head-ache, constipation, easy bruising, anxiety, hair loss, diarrhea and abdominal pain, and low white blood cell counts that re-quired discontinuation42.
CYCLOPHOSPHAMIDE
Cyclophosphamide is an alkylating agent that prevents cell division by cross-linking DNA strands and decreasing DNA synthesis. It is a cell cycle phase nonspeciic agent and has immunosuppressant activity. Cyclophosphamide is a prodrug that must be metabolized to active metabolites in the liver. It has been used in the treatment of many neopla-sias and some autoimmune diseases, like severe rheumatoid disorders, Wegener’s granulomatosis, myasthenia gravis, MS, systemic lupus erythematosus, autoimmune hemolytic ane-mia and idiopathic thrombocytopenic purpura.
However, most studies are based on open-label studies or case series. In MS, the largest study from the Canadian Co-operative Multiple Sclerosis Study Group with 168 pa-tients failed to demonstrate clinical eicacy of cyclophosph-amide43. Another study has indicated some beneicial efects
of cyclophosphamide in young MS patients, excluding those with primary progressive MS. In this study, the responsive pa-tients received repeated cyclophosphamide infusions in a bi-monthly basis after the induction phase44. Common adverse
events of cyclophosphamide include: alopecia, fertility issues, nausea and vomiting, anorexia, diarrhea, mucositis, acute hemorrhagic cystitis or urinary ibrosis, anemia, leukopenia (dose-related with recovery from seven to ten days after ces-sation) and thrombocytopenia.
rituximab45. However, another case report indicated a
fail-ure of monthly cyclophosphamide pulse (1,000 mg/m2) for
six months, although NMO relapses were controlled with rituximab46.
INTERFERON BETA
he therapy using interferon beta has been used in MS treatment in routine practice for over 15 years. However, in-terferon beta is not currently recommended for NMO pa-tients and there are some evidences that it also may be even harmful, increasing the relapse rates47. Other Japanese
stud-ies reported MS patients with good response to interferon beta therapy, compared with NMO patients who experienced increased relapse rate after interferon beta treatment48,49.
Similarly, a series of 25 NMO patients from France were re-ported to experience relapses following treatment with inter-feron beta50. Additionally, there is a case report of a Caucasian
NMO patient from United Kingdom51, suggesting that this
deleterious response to interferon beta is probably not inlu-enced by racial diferences.
OTHER THERAPIES AND FUTURE PERSPECTIVES
Eculizumab is a humanized monoclonal IgG antibody that binds to complement protein C5, preventing cleavage into C5a and C5b. Eculizumab inhibits the subsequent for-mation of terminal complex C5b-9 or membrane attack com-plex. It is currently under investigation for NMO in an
open-label phase I clinical trial at a single center with 14 patients52.
Eculizumab has already been shown to be efective in parox-ysmal nocturnal hemoglobinuria53. Each patient will receive
eculizumab at a dose of 600 mg each week for four weeks, then 900 mg at the ifth week, and 900 mg every two weeks for 48 weeks.
Anecdotal reports have been published using intrave-nous immunoglobulin54, glatiramer acetate55, but replication
of these indings needs to be validated by other studies in a larger number of patients.
Other monoclonal antibodies used in MS treatment have been tried in NMO patients refractory to established treat-ments, like natalizumab, but NMO patients seem to not re-spond to these therapies (personal communication with Dr Anu Jacob, he Walton Centre, Liverpool UK, unpublished).
FINAL REMARKS
he use of corticosteroids and other immunosuppres-sant drugs for NMO treatment has been based on case re-ports or small series of cases rather than in double-blinded randomized studies. his does not mean that these drugs are not efective, but that higher levels of evidence of their efec-tiveness are still lacking. As NMO is a very severe and inca-pacitating CNS disorder, its treatment has to be decided on the basis of clinical judgment, physicians’ experience, case series and extrapolation from management of other autoim-mune conditions while clinical trials are not yet available to provide physicians with options grounded on stronger scien-tiic support.
1. Wingerchuk DM, Hogancamp WF, O’Brien PC, Weinshenker BG. The clinical course of neuromyelitis optica (Devic’s syndrome). Neurology 1999;53:1107-1114.
2. Lennon VA, Wingerchuk DM, Kryzer TJ, et al. A serum autoantibody marker of neuromyelitis optica: distinction from multiple sclerosis. Lancet 2004;364:2106-2112.
3. Pittock SJ, Weinshenker BG, Lucchinetti CF, Wingerchuk DM, Corboy JR, Lennon VA. Neuromyelitis optica brain lesions localized at sites of high aquaporin 4 expression. Arch Neurol 2006;63:964-968.
4. Wingerchuk DM, Lennon VA, Pittock SJ, Lucchinetti CF, Weinshenker BG. Revised diagnostic criteria for neuromyelitis optica. Neurology 2006;66:1485-1489.
5. Watanabe S, Nakashima I, Misu T, et al. Therapeutic efficacy of plasma exchange in NMO-IgG-positive patients with neuromyelitis optica. Mult Scler 2007;13:128-132.
6. Mandler RN, Ahmed W, Dencoff JE. Devic’s neuromyelitis optica: a prospective study of seven patients treated with prednisone and azathioprine. Neurology 1998;51:1219-1220.
7. Watanabe S, Misu T, Miyazawa I, et al. Low-dose corticosteroids reduce relapses in neuromyelitis optica: a retrospective analysis. Mult Scler 2007;13:968-974.
8. Takahashi T, Fujihara K, Nakashima I, et al. Anti-aquaporin-4 antibody is involved in the pathogenesis of NMO: a study on antibody titre. Brain 2007;130:1235-1243.
9. Jarius S, Aboul-Enein F, Waters P, et al. Antibody to aquaporin-4 in the long-term course of neuromyelitis optica. Brain 2008;131: 3072-3080.
10. United States Department of Health and Human Services. Agency for Health Care Policy and Research (AHCPR). Acute pain management: operative or medical procedures and trauma. Clinical practice guideline No 1, AHCPR publication No 92-0023. Rockville, MD: AHCPR; 1993.
11. Guyatt G, Gutterman D, Baumann MH, et al. Grading strength of recommendations and quality of evidence in clinical guidelines: report from an American College of Chest Physicians task force. Chest 2006;129:174-181.
12. Gold R, Buttgereit F, Toyka KV. Mechanism of action of glucocorticosteroid hormones: possible implications for therapy of neuroimmunological disorders. J Neuroimmunol 2001;117:1-8.
13. Brusaferri F, Candelise L. Steroids for multiple sclerosis and optic neuritis: a meta-analysis of randomized controlled clinical trials. J Neurol 2000;247:435-442.
14. Nakamura M, Nakazawa T, Doi H, et al. Early high-dose intravenous methylprednisolone is effective in preserving retinal nerve fiber layer thickness in patients with neuromyelitis optica. Graefes Arch Clin Exp Ophthalmol 2010;248:1777-1785.
15. Clark WF, Rock GA, Buskard N, et al. Therapeutic plasma exchange: an update from the Canadian Apheresis Group. Ann Intern Med 1999;131:453-462.
16. Balogun RA, Kaplan A, Ward DM, et al. Clinical applications of therapeutic apheresis. J Clin Apher 2010;25:250-264.
17. Yoshida H, Ando A, Sho K, et al. Anti-aquaporin-4 antibody-positive optic neuritis treated with double-filtration plasmapheresis. J Ocul Pharmacol 2010;26:381-385.
18. Keller AJ, Urbaniak SJ. Intensive plasma exchange on the cell separator: effects on serum immunoglobulins and complement components. Br J Haematol 1978;38:531-540.
19. Sutton DM, Nair RC, Rock G. Complications of plasma exchange. Transfusion 1989;29:124-127.
20. Keegan M, Pineda AA, McClelland RL, Darby CH, Rodriguez M, Weinshenker BG. Plasma exchange for severe attacks of CNS demyelination: predictors of response. Neurology 2002;58:143-146.
21. Miyamoto K, Kusunoki S. Intermittent plasmapheresis prevents recurrence in neuromyelitis optica. Ther Apher Dial 2009;13:505-508.
22. Cortese I, Chaudhry V, So YT, Cantor F, Cornblath DR, Rae-Grant A. Evidence-based guideline update. Plasmapheresis in neurologic disorders: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology 2011;76:294-300.
23. Weinshenker BG, O’Brien PC, Petterson TM, et al. A randomized trial of plasma exchange in acute central nervous system inflammatory demyelinating disease. Ann Neurol 1999;46:878-886.
24. Munemoto M, Otaki Y, Kasama S, et al. Therapeutic efficacy of double filtration plasmapheresis in patients with anti-aquaporin-4 antibody-positive multiple sclerosis. J Clin Neurosci 2011;18:478-480.
25. Wang KC, Wang SJ, Lee CL, Chen SY, Tsai CP. The rescue effect of plasma exchange for neuromyelitis optica. J Clin Neurosci 2011;18:43-46.
26. Szczepiorkowski ZM, Winters JL, Bandarenko N, et al. Guidelines on the use of therapeutic apheresis in clinical practice-evidence-based approach from the Apheresis Applications Committee of the American Society for Apheresis. J Clin Apher 2010;25:83-177.
27. Carroll W, Fujihara K. Neuromyelitis optica. Curr Treat Options Neurol 2010;12:244-255.
28. Higgs JE, Payne K, Roberts C, Newman WG. Are patients with intermediate TPMT activity at increased risk of myelosuppression when taking thiopurine medications? Pharmacogenomics 2010;11:177-188.
29. Bichuetti DB, Lobato de Oliveira EM, Oliveira DM, Amorin de Souza N, Gabbai AA. Neuromyelitis optica treatment: analysis of 36 patients. Arch Neurol 2010;67:1131-1136.
30. Tanaka Y, Kimura K, Kawachi I, Inuzuka T. No relapse of neuromyelitis optica during drug-induced B-lymphopenia with hypogammaglobulinemia. Neurology 2010;75:1745-1747.
31. Cree BA, Lamb S, Morgan K, Chen A, Waubant E, Genain C. An open label study of the effects of rituximab in neuromyelitis optica. Neurology 2005;64:1270-1272.
32. Imamura H, Tanaka M, Kitagawa N, et al. Trial of rituximab in three patients with neuromyelitis optica. Rinsho Shinkeigaku 2009;49: 457-462.
33. Capobianco M, Malucchi S, di Sapio A, et al. Variable responses to rituximab treatment in neuromyelitis optica (Devic’s disease). Neurol Sci 2007;28:209-211.
34. Nakashima I, Takahashi T, Cree BA, et al. Transient increases in anti-aquaporin-4 antibody titers following rituximab treatment in neuromyelitis optica, in association with elevated serum BAFF levels. J Clin Neurosci 2011;18:997-998.
35. Jacob A, Weinshenker BG, Violich I, et al. Treatment of neuromyelitis optica with rituximab: retrospective analysis of 25 patients. Arch Neurol 2008;65:1443-1448.
36. Bedi GS, Brown AD, Delgado SR, Usmani N, Lam BL, Sheremata WA. Impact of rituximab on relapse rate and disability in neuromyelitis optica. Mult Scler 2011:Epub May 26.
37. Pellkofer HL, Krumbholz M, Berthele A, et al. Long-term follow-up of patients with neuromyelitis optica after repeated therapy with rituximab. Neurology 2011;76:1310-1315.
38. Kim S-H, Kim W, Li XF, Jung I-J, Kim HJ. Repeated treatment with rituximab based on the assessment of peripheral circulating memory B cells in patients with relapsing neuromyelitis optica over 2 years. Arch Neurol 2011:Epub July 11.
39. Goodin DS, Arnason BG, Coyle PK, Frohman EM, Paty DW. The use of mitoxantrone (Novantrone) for the treatment of multiple sclerosis: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology 2003;61: 1332-1338.
40. Weinstock-Guttman B, Ramanathan M, Lincoff N, et al. Study of mitoxantrone for the treatment of recurrent neuromyelitis optica (Devic disease). Arch Neurol 2006;63:957-963.
41. Falcini F, Trapani S, Ricci L, Resti M, Simonini G, de Martino M. Sustained improvement of a girl affected with Devic’s disease over 2 years of mycophenolate mofetil treatment. Rheumatology 2006;45:913-915.
42. Jacob A, Matiello M, Weinshenker BG, et al. Treatment of neuromyelitis optica with mycophenolate mofetil: retrospective analysis of 24 patients. Arch Neurol 2009;66:1128-1133.
43. The Canadian cooperative trial of cyclophosphamide and plasma exchange in progressive multiple sclerosis. The Canadian Cooperative Multiple Sclerosis Study Group. Lancet 1991;337: 441-446.
44. Weiner HL, Mackin GA, Orav EJ, et al. Intermittent cyclophosphamide pulse therapy in progressive multiple sclerosis: final report of the Northeast Cooperative Multiple Sclerosis Treatment Group. Neurology 1993;43:910-918.
45. Mok CC, To CH, Mak A, Poon WL. Immunoablative cyclophosphamide for refractory lupus-related neuromyelitis optica. J Rheumatol 2008;35:172-174.
46. Birnbaum J, Kerr D. Optic neuritis and recurrent myelitis in a woman with systemic lupus erythematosus. Nat Clin Pract Rheumatol 2008;4:381-386.
47. Warabi Y, Matsumoto Y, Hayashi H. Interferon beta-1b exacerbates multiple sclerosis with severe optic nerve and spinal cord demyelination. J Neurol Sci 2007;252:57-61.
48. Shimizu Y, Fujihara K, Kubo S, et al. Therapeutic efficacy of interferon beta-1b in Japanese patients with optic-spinal multiple sclerosis. Tohoku J Exp Med 2011;223:211-214.
49. Uzawa A, Mori M, Hayakawa S, Masuda S, Kuwabara S. Different responses to interferon beta-1b treatment in patients with neuromyelitis optica and multiple sclerosis. Eur J Neurol 2010; 17:672-676.
50. Papeix C, Vidal JS, de Seze J, et al. Immunosuppressive therapy is more effective than interferon in neuromyelitis optica. Mult Scler 2007;13:256-259.
51. Palace J, Leite MI, Nairne A, Vincent A. Interferon beta treatment in neuromyelitis optica: increase in relapses and aquaporin 4 antibody titers. Arch Neurol 2010;67:1016-1017.
52. Mayo Clinic. An open label study of the effects of eculizumab in neuromyelitis optica (http://clinicaltrials.gov/ct2/show/ NCT00904826).
53. Hillmen P, Young NS, Schubert J, et al. The complement inhibitor eculizumab in paroxysmal nocturnal hemoglobinuria. N Engl J Med 2006;355:1233-1243.
54. Bakker J, Metz L. Devic’s neuromyelitis optica treated with intravenous gamma globulin (IVIG). Can J Neurol Sci 2004;31:265-267.