REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
Official Publication of the Brazilian Society of Anesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Comparison
of
the
effect
of
sevoflurane
and
propofol
on
oxygenation
during
gradual
transition
to
one-lung
ventilation
Ays
¸e
Karci
a,∗,
Seden
Duru
a,
Hasan
Hepa˘
gus
¸lar
a,
Lügen
C
¸iftc
¸i
b,
Osman
Yilmaz
caDepartmentofAnesthesiologyandReanimation,MedicalSchool,DokuzEylulUniversity, ˙Izmir,Turkey bDepartmentofAnesthesiology,StateHospital,Denizli,Turkey
cDepartmentofLaboratoryAnimalScience,MedicalSchool,DokuzEylulUniversity,Inciralti, ˙Izmir,Turkey
Received16January2013;accepted22March2013 Availableonline11October2013
KEYWORDS
One-lungventilation; Gradualtransition; Sevofluranepropofol
Abstract
Background: Itisknownthathypoxicpulmonaryvasoconstrictionincreasesasaresultof inter-mittent regional hypoxic challenges. The aim of thisstudy was to compare the effects of sevoflurane andpropofolonoxygenationandshuntfractionduringone-lungventilationina novelmodelofhypoxicpreconditioningbeforeone-lungventilation.
Methods:SixteenWistar-albinoratswere anesthetizedintra-peritoneallybeforevenous and arterial cannulationsandtracheotomized. The animals were randomlyallocated to receive eithersevoflurane2%or10mg/kg/hpropofolinfusionandventilatedwith100%oxygenatan inspiratoryrateof80breaths/minfor30min.Threecyclesofone-lungventilationandtwo-lung ventilationwereperformedandone-lungventilationwascontinuedfor15min.Arterialblood gassampleswereobtainedasfollows:aftercannulationandtracheotomy,following30minof treatmentwithsevofluraneorpropofol,andatthe5thand15thminofone-lungventilation. Results:ThePaO2levelswerehigherandshuntfractionswerelowerinratsreceivingpropofol
comparedtoratstreatedwithsevofluranebutthedifferencewasnotsignificant;thetwogroups werecomparableintermsofPaCO2.
Conclusions: ThesimilareffectsofsevofluraneandpropofolonPaO2duringone-lungventilation
followinghypoxicpreconditioningmaybeduetoothercausesbesidetheinhibitionofhypoxic pulmonaryvasoconstriction.Gradualtransitiontoone-lungventilationisanoveltechniquefor preconditioningexperimentsforone-lungventilation.
© 2013SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mail:[email protected](A.Karci).
Introduction
During one-lung ventilation (OLV), the operated lung not onlyremainsatelectatic,butalsohypoperfusedbecauseof
0104-0014/$–seefrontmatter©2013SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
hypoxicpulmonaryvasoconstriction(HPV),which isa pro-tectivemechanismthatdivertspulmonarybloodflowaway from the lung regions with low alveolar oxygen tensions to better ventilated areas of the lung, and reduces the intrapulmonaryshuntandsystemichypoxia.1---3 Inorderto
maximizeHPVin thenon-ventilated lung, repeated inter-mittentcycles of deflation---inflation to the lung (hypoxic preconditioning(HP)) arerecommended duringthe initia-tionofonelungventilation.4---6
Althoughitisgenerallyacceptedthatvolatileanesthetics inhibit HPV and may promote hypoxemia in a dose-dependentmannerduringOLV,2,7,8 IVanesthetics including
propofol,inhibitHPVtoasmalldegree.8,9
Theoverallobjectiveofthepresentstudywasto deter-mine the efficacy of HP using a new model of ‘gradual transition’toOLVasdefinedinapreviousstudy,7beforethe
initiationofOLVandtocomparetheeffectsofsevoflurane andpropofolduringtheprocedure.
Materials
and
methods
Theanimalswerehandledinaccordancewiththeprinciples oflaboratory animalcare andalltheexperimental proce-dureswereapproved bythe ResearchCommissionfor the CareandUse ofLaboratoryAnimalsofSchoolofMedicine, DokuzEylulUniversity.
Sixteen Wistar-albino rats (weighing 312---382g) were anesthetized by intraperitoneal injection of ketamine (40mg/kg)andxylazine(5mg/kg)priortovenousand arte-rialcannulations.
The femoral veinwas then cannulatedwitha polyeth-ylene tube for infusion of the agents; the same cannula was also used to infuse saline continuously at a rate of 3mLkg−1h−1. The femoral artery on the other side was
similarly cannulated to measure the blood pressure and monitorthearterialbloodgases.Followingtracheotomy,a 16-gauge cannula wasinserted into the trachea and con-nected immediately to the mechanical ventilator (Kent
ScientificPressure-controlled Ventilator)and the animals
were allowed to ventilate in a pressure-controlled mode withaninspiredoxygenfraction(FIO2)of100%,anda
respi-ratoryrateof 60breaths/min. Toeliminate artifacts from spontaneousbreathing movements, paralysis was induced with0.1mg/kgrocuroniumbromide.
Followinga15-minstabilizationperiod,bloodwas with-drawnformeasurementofarterialbloodgasses.Theanimals wererandomly allocatedto receive either 2%sevoflurane throughacalibratedvaporizer(GroupS;n=8)or10mg/kg/h propofolinfusion(GroupP;n=8)for30minafterthe stabi-lizationperiod.Attheendof30min,thetrachealcannula waspushedforwardanditwasconfirmed thatthetipwas inthebronchus,thelungwasventilatedfor1minandthat
thecannulawaspulledbackfortwo-lungventilation(TLV). The animalswereventilatedwithaninspiredoxygen frac-tion(FIO2)of100%,andarespiratoryrateof80breaths/min
duringthisperiod.TheratsweresubjectedtoOLVfollowing threecyclesof1-minOLVand1-minTLV.Thisprocedurewas performedinalltheanimalsbeforetheinvestigations com-menced.Arterialbloodgaseswerecollectedatthe5thand 15thminutesofOLVandtheshuntfractionwascalculated.
Theshuntfractionwascalculatedusingtheformula:
Qs
Qt
(shuntfraction)=(5.8×RI)+6.7,whereRIwastherespiratoryindex.
(a)RI= PAO2−PaO2 PaO2
(b)PAO2=([PB−PH2O]×FIO2)−PaCO2
PB=barometric pressure (760mmHg at sea level); PH2O=partialpressureofwater(47mmHg);PAO2=alveolar
partialpressureofoxygen,PaO2=arterialpartialpressureof
oxygen,PaCO2=arterialpartialpressureofcarbondioxide,
FIO2=inspiratoryoxygenfraction.
We used the method suggested by Koessler et al. and Peyton et al.10,11 The calculation was
done with the formula where RI (Respiratory Index)={[(PB−PH2O)×FIO2]−PaCO2−PaO2}/PaO2.
Statisticalanalyses
Allthe resultswereexpressed asmeans±standard devia-tion.The scattered parameterswere expressedby theSE values. The SPSS 11.0 for Windowswas used for the sta-tisticalanalyses.TheKolmogorov---Smirnovtestwasusedto evaluatetheintergroupdifferences.
The statistical tests were carried out with the signifi-cancelevelsetatp<0.05.
Results
The intermittent cycles of deflation---inflation before OLV werestudiedin16ratsallocatedrandomlytotreatmentwith sevofluraneinhalationorpropofolinfusion.
There wereno significant differences in the blood gas analysis and shunt fraction among the protocol groups, eitherattheendofstabilizationperiod,oraftertreatment withsevofluraneorpropofol.
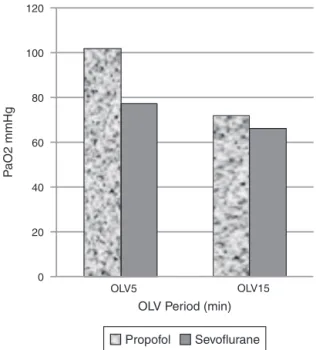
Following 30min of anesthesia, marked decreases in arterial oxygen tensions (mean±SE) were observed in the propofol and sevoflurane groups 5min after the onset of OLV (101.48±12.37 and 77.08±6.17, respectively). The decrease was 29% and 38% in the propofol and the sevoflurane groups, respectively, and this decrease was not significant between the groups (p=0.074).After15min,the decreaseinoxygenationwas more pronounced (mean 71.65±5.39 [57.90---103.10] and 66.01±4.19[56.50---100.08]).Consistently,thePaO2values werehigherin thepropofolgroupfor thedurationof OLV (Fig.1).
120
100
80
60
40
20
0
OLV5 OLV15
OLV Period (min)
P
aO2 mmHg
Sevoflurane Propofol
Figure1 Time-relatedchangesinarterialpartialpressureof oxygenduringone-lungventilation.
41.62±2.05, respectively), and 15min (38.27±2.36; 47.54±2.54, respectively). Consequently, the pH values decreased and the difference between the groups was significant at 5min (7.41±0.3 and 7.34±0.02; p=0.022, respectively)(Fig.2).The differencewasnot apparentat theendof15min(7.38±0.2and7.31±0.02;p=0.052).
After gradual transition to OLV, the Qs/Qt did not
showasignificantdifference, dependingontheanesthetic agent.Thepulmonaryshuntfraction(Qs/Qt)increasedfrom
28.53±1.91to42.67±3.87intheratstreatedwith propo-fol;theincreasewasfrom40.61±7.25to53.72±4.20inthe sevofluranegroupin5minofOLV.TheQs/Qtchangefrom5to
7.44
7.42
7.4
7.38
7.36
7.28
7.26
OLV5 PLV15
OLV Period (min) 7.32
7.33 7.34
pH
Sevoflurane Propofol
Figure2 Timerelatedchangesinarterialpartialpressureof arterialpHduringone-lungventilation.*p<0.05propofol anes-thesiacomparedtosevofluraneanesthesia.
15minofOLV(57.31±3.53and61.18±4.20inthepropofol andthesevofluranegroups,respectively)wasnotsignificant betweenthetwoanestheticregimens.
Discussion
Thepresentstudyhasshownthatsevofluraneandpropofol atthedosesused,hadsimilareffectsonarterialoxygenation andshuntfractionduringOLVintheratmodelofHP.
Inpreviousanimalstudies,it wasconcludedthat inter-mittenthypoxiaincreasestheHPVandthattheresultshave importantimplicationsfortheconductofHPVexperiments andinterpretationofblood-gaschangesduringOLV.4---6
Sim-ilarly, Singh et al.12 demonstrated for the first time that
preconditioningwithalowdoseofcobaltwasadvantageous inprotectingthelungandthebrainbyattenuatinghypobaric hypoxia-inducedoxidativeinjury.Inanattempttoincrease thetolerancetohypoxemiathatwoulddevelopduringOLV, weexamined theeffectofan uniquemodelfor precondi-tioning,namely‘gradualtransition’toOLV.
HP is defined as a rapid and reversible pro-adaptive responsetomild hypoxicexposure that protectsthe cells from subsequent hypoxic or ischemic insult, and it is reported tooccur in two temporally distinct phases, the earlyandthelatephases.Hypoxicprotectionbyearly pre-conditioningoccurswithinminutes,peaksinaboutanhour, andlasts forabout 4h.13 Therefore,forthefirsttime,we
usedthreeconsecutive1-minOLVandTLVcyclesbeforea longerperiodofOLVinordertoallowthetissuestoadapt totheforthcoming hypoxemia.Inan animal model of HP, Shuklaetal.14 demonstratedthatacuteexposureto
hypo-barichypoxialedtoanincreaseinthelungwatercontent, total protein and albumin leakage in lavage fluids. How-ever,whentheanimalswereexposedtohypoxia afterHP, asignificant decreaseinthelungwatercontentaswellas theserumtotalproteinandalbuminleakagewasobserved. ThepreviousadaptationinducedbyHPresultedinincreased tolerancetolethalhypoxia.
The effect of sevoflurane and propofol with regard to oxygenation and shunt fraction during OLV following preconditioning was also investigated. Despite numerous reports15,16 about the decrease of oxygenation and the
increase of shunt fraction due to inhibition of HPV with inhalational anesthetics agents, some17---19 have indicated
the opposite. Glasser et al.2 concluded that attenuation
of HPV is not a general characteristic of all inhalational anesthetics.Furthermore,intheirclinicalinvestigation,Abe etal.9 demonstrated that propofol improved the
oxygen-ationand shunt fraction during OLV comparedto volatile anesthetics.Accordingtoourresultsinratsreceiving propo-folorsevoflurane,thedecreaseinarterialoxygenationwas paralleltotheincreaseinshuntfractionamongtransitionto OLV,butthegroupsdidnotdifferinthisrespect.Although the PaO2 values (Fig. 1) were higher and the shunt
frac-tionswerelowerinthepropofolgroupcomparedtotherats treatedwithsevoflurane,thedifferencebetweenthegroups neverreachedasignificantlevel.OLVcausedanincreasein PaCO2,whichwasaccompaniedbyanadequatedecreasein
Weproposetworeasonsfortheresultsofourstudy.First, asDeConno etal.20 recentlydescribed,thevolatile
anes-theticsevofluranehasanimmunomodulatoryroleinpatients undergoingOLVwithasignificantdecreaseininflammatory mediators. Their analysis has shown an almost exponen-tialincreaseininflammatorymediatorsincorrelationwith theOLVtimeinthepropofolgroup.Interestingly,a signif-icant correlation wasobserved between CRP and theOLV timein thepropofolgroup,thiswasclearlyattenuatedin thesevoflurane group. Secondly, since hypoxicprotection byearlypreconditioning occurswithinminutes,13 we used
1-mincyclesofdeflationandinflation.However,recently, Duan et al.21 used a protocol in which the rats inhaled
hypoxic air mixture for 5min followed by 10min of air inhalation.Themethodologicaldifferencesbetweenthetwo studiesmayexplainthediscrepancybetweentheresults.
The onsetofOLVis characterizedbydevelopmentofa significantintrapulmonaryshuntthroughthecollapsedlung withthe potentialfor intraoperative hypoxemia. Absence of afurther decrease in oxygenationor increase in shunt fractionfrom5to15minofOLVmayindicatethatthe maxi-mumHPVwasreachedin5min.Thesefindingsareconsistent withobservationsmadebyChenetal.4whoreportedthat
themaximumHPVwasreachedattheinitiationofhypoxia andnofurtherincreasewasobservedwithrepeatedhypoxia episodes.Conversely,Marshalland Marshall15 showedthat
inthepresenceofmethyleneblue,thereisahypoxic pul-monaryvasoconstrictorresponse,whichispotentiatedwith time.Pirloetal.5foundthatrepeated(2---4times)
intermit-tenthypoxic challenges toalobe of thelung potentiated andfinallymaximizedthelobarHPV.Thus,puttingasidethe questionofthetime-alonefactor,intermittenthypoxiahas beenreportedtoincreaseHPVinaquantitativemanner.
Abe et al.9 concluded that propofol improved
oxy-genation duringsingle-lung ventilation (OLV)compared to volatile anesthetics. There is a possibility, however, that oxygenationduringOLVmayimprovewithtime.Accordingly, Ishikawaetal.22showedthatafterstartingOLV,meanPaO
2
rapidlydecreasedandgraduallyincreasedthereafter. The ventilation technique is important if we are to decreasethe incidence of hypoxemia during OLV.Thus, a careful ventilatory strategy was adopted in this study in order to avoid additional stress factors to the inflamma-tory responsetriggered by OLV.It has been reportedthat pressure-controlledventilationinratsoffersadecelerating flow pattern, which results in a more homogenous distri-butionoftidalvolume,recruitsthepoorlyventilatedlung regionsandimprovesoxygenation.3,23Moreover,lungtrauma
isattenuatedwhenthepeakandplateautransalveolar air-waypressuresarecontrolled.3,24
Insummary,sevofluraneadministeredataconcentration of2%resultedincomparablechangesintheshuntfraction asdidpropofolinratsduringthe‘gradualtransition’toOLV. Similarly,PaO2,andPaCO2levelsdidnotdifferbetweenthe
groups.ChangesintheshuntfractionduringOLVmay prob-ablyresultfromsourcesotherthantheattenuationofthe HPVresponse.Hemodynamicchanges,pulmonaryperfusion and in particular, appropriate ventilatory strategies that preventalveolarcollapsemaybemoreimportantfor obtain-ingoptimalarterialoxygenationduringOLVthaneitherthe anestheticagentof choice or thepreconditioning maneu-vers.‘Gradual transition’toOLVin ratsisauniquemodel
for HP andourresultsindicatethat longerperiodsof OLV mayberequired.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.BeckDH,DoepfmerUR,SinemusC,BlochA,SchenkMR,KoxWJ. Effectsofsevofluraneandpropofolonpulmonaryshuntfraction duringone-lungventilationforthoracicsurgery.BrJAnaesth. 2001;86:38---43.
2.GlasserSA,DominoKB,LindgrenL,ParcellaP,MarshallC, Mar-shallBE.Pulmonarybloodpressureandflowduringatelectasis inthedog.Anesthesiology.1983;58:225---31.
3.Leite CF, CalixtoMC, Toro IF, Antunes E, Mussi RK. Charac-terizationofpulmonaryandsystemicinflammatoryresponses produced bylung re-expansion afterone-lung ventilation. J CardiothoracVascAnesth.2012;26:427---32.
4.Chen L, Miller FL, Williams JJ, Alexander CM, Domino KB, MarshallC, etal. Hypoxic pulmonary vasoconstrictionis not potentiatedbyrepeatedintermittenthypoxiainclosedchest dogs.Anesthesiology.1985;63:608---10.
5.Pirlo AF, Benumof JL, Trousdale FR. Potentiation of lobar hypoxicpulmonaryvasoconstrictionbyintermittenthypoxiain dogs.Anesthesiology.1981;55:226---30.
6.BenumofJL.Intermittenthypoxiaincreaseslobarhypoxic pul-monaryvasoconstriction.Anesthesiology.1983;58:399---404.
7.C¸iftc¸L,Hepa˘gus¸larH,Do˘ganA,YılmazO,ElarZ.Theeffect ofgradualtransitiontoonelungventilationonoxygenationin rats.TurkiyeKlinikleriJAnestReanim.2010;8:6---13.
8.Von Dossow V, Welte M, Zaune U, et al. Thoracic epidural anesthesia combined withgeneral anesthesia: the preferred anesthetic technique for thoracic surgery. Anesth Analg. 2001;92:848---54.
9.Abe K, Shimizu T, Takashina M, Shiozaki H, Yoshiya I. The effectsofpropofol,isoflurane,andsevofluraneonoxygenation andshuntfractionduringone-lungventilation.AnesthAnalg. 1998;87:1164---9.
10.KoesslerMJ,FabianiR,HamerH,PittoRP.Theclinicalrelevance ofembolic eventsdetected bytransesophageal echocardiog-raphyduring cemented totalhiparthroplasty:a randomized clinicaltrial.AnesthAnalg.2001;92:49---55.
11.PeytonPJ,RobinsonGJB,McCallPR,ThompsonB.Noninvasive measurementofintrapulmonaryshunting.JCardiothoracVasc Anesth.2004;18:47---52.
12.SinghM,ShuklaD,ThomasP,SaxenaS,BansalA.Hypoxic pre-conditioningfacilitatesacclimatizationtohypobarichypoxiain ratheart.JPharmPharmacol.2010;62:1729---39.
13.DasguptaN,PatelAM,ScottBA,CrowderCM.Hypoxic precondi-tioningrequirestheapoptosisproteinCED-4inC.elegans.Curr Biol.2007;17:1954---9.
14.ShuklaD,SaxenaS,PurushothamanJ,etal.Hypoxic precon-ditioningwith cobaltameliorates hypobaric hypoxia induced pulmonaryedemainrat.EurJPharmacol.2011;656:101---9.
15.Marshall C, Marshall BE. Endothelium-derived relaxing fac-tor is not responsible for inhibition of hypoxic pulmonary vasoconstriction by inhalational anesthetics. Anesthesiology. 1990;73:441---8.
17.PruszkowskiO,DalibonN,MoutafisM,etal.Effectsofpropofol vssevofluraneonarterialoxygenationduringone-lung ventila-tion.BrJAnaesth.2007;98:539---44.
18.LesitskyMA,DavisS,Murray PA.Preservationofhypoxic pul-monary vasoconstriction during sevoflurane and desflurane anesthesia compared to the conscious state in chronically instrumenteddogs.Anesthesiology.1998;89:1501---8.
19.SchillingT,KozianA,KretzschmarM,etal. Effectsof propo-fol and desfluraneanaesthesia onthe alveolarinflammatory responsetoone-lungventilation.BrJAnaesth.2007;99:368---75 [Epub2007July9].
20.DeConnoE,SteurerMP,WittlingerM,etal.Anesthetic-induced improvementoftheinflammatoryresponsetoone-lung venti-lation.Anesthesiology.2009;110:1316---26.
21.DuanZ,ZhangL,LiuJ,XiangX,LinH.Earlyprotectiveeffect oftotalhypoxicpreconditioningonratsagainstsystemicinjury from hemorrhagicshockand resuscitation.JSurgRes. 2012: 12.
22.IshikawaS,OhmiS,NakazawaK,MakitaK.Continuous intra-arterialbloodgasmonitoringduringthoracicsurgery.JAnesth. 2000;14:119---23.
23.ArnoldTC,ZhangS,XiaoF,ConradSA,CardenDL.Pressure con-trolledventilationattenuateslungmicrovascularinjuryinarat modelofactivatedcharcoalaspiration.JToxicolClinToxicol. 2003;41:119---24.