www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
A
possible
cause
of
epistaxis:
increased
masked
hypertension
prevalence
in
patients
with
epistaxis
夽
Baran
Acar
a,∗,
Bunyamin
Yavuz
b,
Erdem
Yıldız
a,
Selcuk
Ozkan
a,
Mehmet
Ayturk
a,
Omer
Sen
c,
Onur
Sinan
Deveci
aaKeciorenTrainingandResearchHospital,DepartmentofOtorhinolaryngology,Ankara,Turkey bMedicalParkAnkaraHospital,DepartmentofCardiology,Yenimahalle,Turkey
cKeciorenTrainingandResearchHospital,DepartmentofCardiology,Ankara,Turkey
Received23October2015;accepted15January2016 Availableonline18April2016
KEYWORDS
Maskedhypertension; Epistaxis;
Spontaneous
Abstract
Introduction:Epistaxis and hypertension are frequent conditions in the adult population. Maskedhypertensionisdefinedasaclinicalconditioninwhichapatient’sofficebloodpressure levelis<140/90mmHg,buttheambulatoryorhomebloodpressurereadingsareinthe hyper-tensiverange.Manystudieshaveprovedthathypertensionisoneofthemostimportantcauses ofepistaxis.Theprevalenceofthisconditioninpatientswithepistaxisisnotwelldefined.
Objective: This study aimed to evaluate the prevalence ofmasked hypertensionusing the resultsofofficebloodpressuremeasurementcomparedwiththeresultsofambulatoryblood pressuremonitoring.
Methods:Sixtypatientswithepistaxisand60controlsubjectswereenrolledinthestudy.All patientswithepistaxisandcontrolswithouthistoryofhypertensionunderwentphysical exami-nation,includingofficebloodpressuremeasurement,ambulatoryorhomebloodpressure,and measurementofanthropometricparameters.
Results:Meanagewassimilarbetweentheepistaxisgroupandthecontrols---21---68years(mean 42.9)fortheepistaxisgroupand18---71years(mean42.2)forthecontrolgroup.Atotalof20 patients(33.3%)intheepistaxisgroupand7patients(11.7%)inthecontrolgroup(p=0.004) hadmaskedhypertension.Night-timesystolicbloodpressurewassignificantlyhigherinpatients withepistaxisthaninthecontrolgroup(p<0.005).However,nosignificantdifferencewasfound indaytimesystolicbloodpressurebetweenthecontrolgroupandthepatientswithepistaxis (p=0.517).
夽 Pleasecitethisarticleas:AcarB,YavuzB,YıldızE,OzkanS,AyturkM,SenO,etal.Apossiblecauseofepistaxis:increasedmasked
hypertensionprevalenceinpatientswithepistaxis.BrazJOtorhinolaryngol.2017;83:45---9. ∗Correspondingauthor.
E-mail:[email protected](B.Acar).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.01.007
Conclusion:This study demonstrates increasedmasked hypertensionprevalencein patients withepistaxis.Wesuggestthatallpatientswithepistaxisshouldundergoambulatoryorhome bloodpressuretodetectmaskedhypertension,whichcouldbeapossiblecauseofepistaxis. © 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Hipertensão mascarada; Epistaxe; Espontânea
Umapossívelcausadeepistaxe:maiorprevalênciadehipertensãomascaradaem pacientescomepistaxe
Resumo
Introduc¸ão:Epistaxeehipertensãosãocondic¸õesfrequentesnapopulac¸ãoadulta.Hipertensão mascaradaédefinidacomoumacondic¸ãoclínicaemqueoníveldapressãoarterialdopaciente noconsultórioé<140/90mmHg,masasleiturasdapressãoarterialambulatorialouemcasa, seencontramnafaixahipertensiva.Muitosestudosdemonstraramqueahipertensãoéumadas causasmaisimportantesdeepistaxe.Aindanãoestádevidamentedefinidaaprevalênciadessa condic¸ãoempacientescomepistaxe.
Objetivo:EsseestudoteveporobjetivoavaliaraprevalênciadeHMcomousodosresultados demensurac¸õesdapressãoarterialnoconsultório,emcomparac¸ãocomosresultadosdaMAPA.
Método: Paraoestudo,foramrecrutados60pacientescomepistaxee60indivíduospara cont-role.Todosospacientescomepistaxeeoscontrolessemhistóricodehipertensãopassarampor examefísico,inclusivedeterminac¸ãodapressãoarterialnoconsultório,MAPAemensurac¸ão dosparâmetrosantropométricos.
Resultados: Amédia deidade foisimilar entreogrupo comepistaxeeos controles:de 21 a68 (média 42,9)anospara ogrupo comepistaxe, ede18 a71 (média 42,2)anospara o grupocontrole.Nototal,20pacientes(33,3%)nogrupocomepistaxee7pacientes(11,7%)no grupocontrole(p=0,004)apresentaramhipertensãomascarada.A pressãoarterialsistólica noturna foisignificantemente maisalta empacientescomepistaxe, em comparac¸ãocomo grupocontrole(p<0,005).No entanto,nãofoi observadadiferenc¸asignificante napressão arterialsistólicaobtidaduranteodiaentreogrupocontroleeospacientescomepistaxe(p= 0,517).
Conclusão:O presente estudo demonstra maior prevalência de hipertensão mascarada em pacientescomepistaxe.Sugerimosquetodosospacientescomepistaxedevamser submeti-dosàmonitorac¸ãodapressãoarterialcaseiraouemconsultóriocomoobjetivodedetectar hipertensãomascarada,quepodeserumacausapossíveldeepistaxe.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Bleeding in the nasal cavity caused by mucosa injury or vascular pathology as a resultof coagulation disorders is knownasepistaxis.1 Epistaxis is oneofthe mostcommon
ear---nose---throat (ENT) emergencies that require hospital admission,butis rarelylife threatening.Epistaxis ismore commoninmenthaninwomen,anditsfrequencyincreases withage.1,2Theincidenceofepistaxisisnotexactlyknown,
but it is approximately 7---60% of the population. Epis-taxis can be post-traumatic, iatrogenic (nasal surgery or endoscopic procedures), and spontaneous, resulting from possible causative factors, including local nasal factors (inflammation and infection), medications, and systemic factorssuchascoagulationdisorders,alcoholism,hereditary hemorrhagictelangiectasia,andhypertension.1,2
Thenosehasarichvascularsupply,withsubstantial con-tributions from the internal carotid artery (ICA) and the externalcarotidartery(ECA).TheECAsystemsuppliesblood to the nose via the facial and internal maxillary arter-ies. The ICA contributes to nasal vascularity through the ophthalmic artery.3 Kiesselbach’splexus or Little’sarea is
an anastomoticnetworkof vesselslocatedin theanterior cartilaginous septum. Many of the arteries supplying the septum have anastomotic connections at this site. More than 90% of bleedings occur in the anterior region and arise fromLittle’sarea, where Kiesselbach’splexus forms on the septum.3 The posterior epistaxis, which is usually
Hypertensionisamajorcauseofspontaneousepistaxis. Patients with epistaxis commonly present with elevated blood pressure.Epistaxis ismore commoninhypertensive patients,perhapsowingtovascularfragilityfromthe long-standingdisease.4However,epistaxispatientswithnormal
bloodpressurearenotwellinvestigatedformasked hyper-tension(MH).
The phenomenon of MH is defined asa clinical condi-tioninwhichapatient’sofficebloodpressure(BP)levelis <140/90mmHg,buttheambulatoryorhomeBPreadingsare inthehypertensiverange.4ThehighprevalenceofMH
sug-geststhenecessityformeasuringout-of-officeBPinpersons withapparently normal or well-controlledoffice BP.5 The
prevalenceofMHinthegeneralpopulationcouldbeashigh as10%.However,dataobtainedfromseveralcross-sectional studies have demonstrated large differences,with preva-lencerates ranging froma low of 8% toa high of 49%.6,7
Hypertension by 24h ambulatory blood pressure monitor-ing (ABPM) is definedwhen themean daytimesystolicBP is equal toor greater than 135mmHg or when the mean daytimediastolicBPisequal toor greaterthan85mmHg, according to the seventh report of the 2003 US Hyper-tensionJointNationalCommitteeandEuropeanSocietyof Hypertension.8
ThisstudyaimedtoevaluatetheprevalenceofMHusing ABPMamongpatientswithepistaxis.
Methods
Thisprospectivestudy includedthereview ofthemedical chartsofpatientswithmild,moderate,orsevereepistaxis that wastreated medically or surgically between Decem-ber2012andJanuary2015.Allsubjectsgavetheirinformed consent. The study protocol has been approved by the ethics committee of the Kecioren Hospital (approval No. 185-09.01.2013).
Atotalof120patientsparticipatedinthestudy.Patients were separated into two groups: the epistaxisgroup and thecontrolgroupthatdidnotpresentwithepistaxis.Both groups included 60 patients,and eachgroup had40 male and 20 female patients. Patients’ age ranged from 21 to 68 years (mean 42.9) for the epistaxis group and 18 to 71 years (mean 42.2) for the control group. The inclu-sion criterion was spontaneous epistaxis (without trauma ornasalsurgery)withnormalofficeBPandwithoutknown hypertension.Theexclusioncriteriaincludedchronic liver disease, chronic kidney disease, or coagulopathy, aswell as patients who were taking anti-thrombotic drugs, had nasaltrauma,hadundergonenasalsurgery,orhadprevious hypertension.
Afterpatients’BPwasmeasuredandactivenosebleeding wasstoppedbymedicalorsurgicalmanagement,laboratory parametersoftheCBC,INR,andAPTTtestswerestudied, echocardiography in the cardiology clinic was conducted, anda24hBPMdevice(Holterdevice)wasappliedtoeach patient.
NormalofficeBPwasdefinedas<140/90mmHg.MHwas definedasapatient’sofficeBPlevelof<140/90mmHgand ABPMparametersin the hypertensive range(24h average BP≥130/80mmHgand/ordaytimeaverage≥135/85mmHg and/ornight-timeaverage≥120/70mmHg).
76
74
72
70
68
66
64
62
60
58
56
Control group Epistaxis group
All diast BP Day diast BP Night diast BP
Figure1 Dayandnightdiastolicbloodpressures(BP)were significantlyhigherfortheepistaxisgroup.
Statisticalanalysis
Continuous parametric and nonparametric data are pre-sented as the mean±standard deviation (SD) or as the median(range),respectively.Non-continuousvariablesare presentedaspercentages.Categoricalvariableswere com-paredwithPearson’schi-squaredtest.Continuousvariables werecomparedwithStudent’st-testandMann---WhitneyU tests.SPSSv.15.0wasusedforstatisticalanalyses.
Results
A total of 60 patients with epistaxis and 60 control sub-jectswereenrolledinthestudy.Themeanagewassimilar betweentheepistaxisgroupandthecontrols:21---68years (mean42.9)fortheepistaxisgroupand18---71years(mean 42.2)for the control group. Nosignificant difference was found in the demographic features and laboratory and transthoracic echocardiography parameters between the groups.
130
125
120
115
110
105
100
Control group Epistaxis group
All sist BP Day sist BP Night sist BP
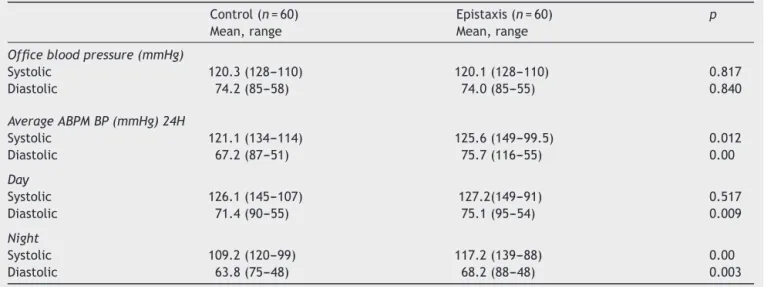
Table1 Officebloodpressure,24hambulatorybloodpressure,andtheircomparisonforthecontrolandepistaxisgroups.
Control(n=60) Epistaxis(n=60) p
Mean,range Mean,range
Officebloodpressure(mmHg)
Systolic 120.3(128---110) 120.1(128---110) 0.817
Diastolic 74.2(85---58) 74.0(85---55) 0.840
AverageABPMBP(mmHg)24H
Systolic 121.1(134---114) 125.6(149---99.5) 0.012
Diastolic 67.2(87---51) 75.7(116---55) 0.00
Day
Systolic 126.1(145---107) 127.2(149---91) 0.517
Diastolic 71.4(90---55) 75.1(95---54) 0.009
Night
Systolic 109.2(120---99) 117.2(139---88) 0.00
Diastolic 63.8(75---48) 68.2(88---48) 0.003
Twentypatients(33.3%)intheepistaxisgroupandseven patients (11.7%) in the control group (p=0.004) had MH. Figs. 1 and 2 show the systolicand diastolic BP levels in theepistaxisand control groups. The officeBP and ABPM parametersarepresentedinTable1.
DaytimediastolicBP, 24h systolicand diastolicBP,and nighttimesystolicanddiastolicBPweresignificantlyhigher inpatientswithepistaxisthaninthoseinthecontrolgroup. However,nosignificantdifferencewasfoundinthedaytime systolicBPbetweenthecontrolgroupandthepatientswith epistaxis(p=0.517).
Discussion
To the best of the authors’ knowledge, this study is the firsttoinvestigateMHprevalenceinpatientswithepistaxis. ThestudyshowsincreasedMHprevalence inpatientswith epistaxis.
Epistaxisandhypertensionarefrequentconditionsinthe adultpopulation.Therelationshipbetweenthelevelof arte-rialpressureandtheincidenceofepistaxisinpatientswith hypertensionisanissue thatappearsfrequentlyinclinical practice.
Despiteoverthypertensionrepresentingthemajorcause of spontaneous epistaxis, no study has yet evaluatedthe relationship between MH and epistaxis. Compared with other measures, the 24h ABPMis more valuable for pre-dictingprognosis,asitmoreaccuratelyassessestheriskof cardiovasculardiseasethanmeasurementsofBPmade dur-ingclinicorofficevisits,andABPMisalsocloselyrelatedto damageofthetargetorgan.9
Onlya limitednumber ofABPMstudies have examined patients with epistaxis. The probable reason is that if a patient presents with normal office BP, hardly any oto-laryngologistwouldperformABPM.10 Recentstudiesonthe
management of patients with epistaxis and hypertension donotmentiontheprevalenceofMHinepistaxispatients, andonly recommendtheuseofABPMor homemonitoring devicesforamoreaccuratediagnosticofMH.11
For the purpose of this study, patients with epistaxis withnohistoryof hypertensionweredeliberately chosen. This studyfound ahighprevalence ofMH inpatientswith epistaxis.MHwaspresentin20(33.3%)patientsinthe epis-taxis group and in seven (11.7%) patients in the control group. Page et al. showedthat serious spontaneous epis-taxis could also be the presenting sign of an underlying overt hypertension in about 43% of patients with no his-tory ofhypertension.12 Thisfindingcouldbeattributedto
theselection of patients,asPage etal.included patients withserious epistaxisonly. Comparing the present results withthose in the available literature, it can be hypothe-sized thatMH ismore prevalentinpatients withepistaxis thaninthosewithout.Basedontheseresults,more large-scalestudiesthatincludesubjectsfromthewholespectrum of patients with epistaxis and arterial hypertension are needed.
Thepresentstudyusedmorecommonbutstrictercriteria forMH.Thecriteriaarejustifiedforuseinpatientswith epis-taxisbecauseofthehighprevalenceofMHinthesepatients. Moreover,thenighttimesystolicBPwassignificantlyhigher inpatientswithepistaxisthaninthosewithout.Thisfinding maypresentevidenceonthegreaterimportanceof noctur-nalhypertensioninthepathophysiologyofthedevelopment ofMHthanthesimplepresenceofdaytimeBP.Morestudies areneededfor abetterunderstandingofthe pathophysio-logyofMHdevelopment.
The mechanism of how MH could lead to epistaxis remainsunknown.Oneofthemechanismsmayberelatedto endothelialdysfunction.Astudyrevealedthatthepresence of MH is one of the independent determinants of cardio-vascular disease.6 Only a limited number of studies have
been conducted on how epistaxis influences MH or noc-turnalhypertension.Properbloodpressuremanagementis necessary for the prevention of persistent epistaxis from Kiesselbach’sareaintheclinicalsettingofemergencycare practice.13 Intheauthors’clinicalpractice,mostepistaxis
Conclusion
This study demonstrated that MH prevalence is higher in patientswithepistaxis.Itissuggestedthatallpatientswith epistaxisshouldundergoABPMtodetect MH,which could beapossiblecauseofepistaxis.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.VarshneyS,SaxenaRK.Epistaxis:aretrospectiveclinicalstudy. IndianJOtolaryngolHeadNeckSurg.2005;57:125---9.
2.ChaiyasateS,RoongrotwattanasiriK, FooananS,Sumitsawan Y. Epistaxis in Chiang Mai University. J Med Assoc Thai. 2005;88:1282---6.
3.VenettacciO,NettlefoldC,ChanL,DanielM,CurottaJ. Sub-labialpacking:anovelmethodofstoppingepistaxisfromLittle’s area.IntJPediatrOtorhinolaryngol.2013;77:1370---1.
4.SarhanNA, AlgamalAM. Relationship between epistaxisand hypertension:acauseandeffectorcoincidence?JSaudiHeart Assoc.2015;27:79---84.
5.Angeli F, Reboldi G, Verdecchia P. Masked hypertension: evaluation, prognosis, and treatment. Am J Hypertens. 2010;23:941---8.
6.TomiyamaM,HorioT, YoshiiM, TakiuchiS,KamideK, Naka-muraS,etal.Maskedhypertensionandtargetorgandamage
in treated hypertensive patients. Am J Hypertens. 2006;19: 880---6.
7.Hänninen MR, Niiranen TJ, Puukka PJ, Mattila AK, Jula AM. Determinants of masked hypertension in the general population: the Finn-Home study. J Hypertens. 2011;29: 1880---8.
8.ChobanianAV,Bakris GL,BlackHR, CushmanWC,Green LA, IzzoJLJr,etal.Theseventhreportofthejointnational com-mittee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. JAMA. 2003;289: 2560---72.
9.Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R, Germano G. Guidelines for the management of arterial hypertension:thetaskforce forthemanagement ofarterial hypertension of theEuropean Societyof Hypertension(ESH) andoftheEuropeanSocietyofCardiology(ESC).JHypertens. 2007;25:1105---87.
10.ManciaG,FagardR,NarkiewiczK,RedonJ,ZanchettiA,Böhm M,etal.TaskForceforthemanagementofarterial hyperten-sionoftheEuropeanSocietyofHypertensionandtheEuropean SocietyofCardiology.BloodPress.2014;23:3---16.
11.KikidisD,TsioufisK,PapanikolaouV,ZervaK,HantzakosA.Is epistaxisassociatedwitharterialhypertension?EurArch Otorhi-nolaryngol.2014;271:237---43.
12.PageC,BietA,LiabeufS,StrunskiV,FournierA.Serious spon-taneousepistaxisandhypertensioninhospitalizedpatients.Eur ArchOtorhinolaryngol.2011;268:1749---53.