Braz. j. . vol.80 número2
Texto
Imagem
Documentos relacionados
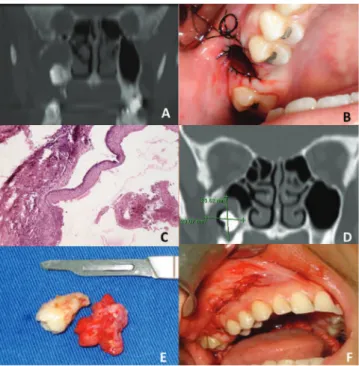
The aim of this study was to evaluate the viabili- ty of the cell block technique as an auxiliary method for the diagnosis of maxillary bone lesions with a cystic
Ultrasound revealed a cystic mass with a possible diagnosis of a branchial cyst along the left jugulo-carotid chain with an inflammatory aspect; computed
Contrast-enhanced axial (A) and coronal (B) computed tomography of the paranasal sinus, showing a voluminous mass in the right nasal cavity that extended as far as the
Computed tomography (CT) evidenced a lesion with soft tissue consistency at the ethmoid, right maxillary sinus, and nasal cavity, showing erosion of the lamina papyracea,
In view of the problem studied, the aim of this study was to perform an analysis of the area relative to the maxillary sinuses; that is, the height and width of the sinus cavity,
Figure 2 - Computed tomography scan of the chest showing an extensive mediastinal lesion (arrow) in contact with the right tracheal wall and causing anterior deviation
They demonstrated an expansive lesion, with heterogeneous enhancement by contrast, positioned in the center of the right maxillary sinus, with accentuated enlargement
9 Preoperative coronal section computed tomography highlighting the right sphenoid heterogeneous opaci fi cation with signs of remodeling in the wall of the sphenoid sinus and
