Oral Pathology
Anne Caroline Costa Oenning(a) Elena Riet Correa Rivero(b) Maria Cristina Marino Calvo(c) Maria Inês Meurer(b)
Liliane Janete Grando(b)
(a)Postgraduate Program in Dentistry, Federal University of Santa Catarina, Florianópolis, SC, Brazil.
(b)Department of Pathology, Federal University of Santa Catarina, Florianópolis, SC, Brazil. (c)Department of Public Health, Federal
University of Santa Catarina, Florianópolis, SC, Brazil.
Corresponding author: Liliane Janete Grando
E-mail: [email protected]
Received for publication on Dec 19, 2011 Accepted for publication on May 09, 2012
Evaluation of the cell block technique
as an auxiliary method of diagnosing
jawbone lesions
Abstract: This study investigated the viability of the cell block technique as an auxiliary method of diagnosing jawbone lesions. Thirty-three clini-cally diagnosed jawbone lesions with a cystic appearance were subject-ed to aspiration. The aspiratsubject-ed material was processsubject-ed by the cell block technique, and the lesions were biopsied and treated. Cytological indings (cell block) and histopathology analyses (gold standard) were compared by the chi-square test. There were associations between cysts and choles-terol crystal clefts, between keratocystic odontogenic tumors (KOT) and epithelial cells, and between KOT and parakeratin. The occurrence of cholesterol crystal clefts in cell block slides was correlated with cystic le-sions, and the parakeratin presence was a KOT indicator. The cell block technique proved to be fast, easy-to-handle, and low-cost, making it an attractive auxiliary method for the preliminary diagnosis of jawbone le-sions.
Descriptors: Biopsy, Needle; Jaw Cysts; Odontogenic Tumors.
Introduction
Several disease entities, of both odontogenic and non-odontogenic origin, may affect the maxillomandibular complex. These lesions can exhibit similar clinical and imaging appearances associated with a wide range of histopathological and behavior features.1
In most cases of bone lesions, a biopsy and histopathological analysis are necessary to establish the inal diagnosis.1 Biopsy may be a complex
procedure at some maxillomandibular sites, and some systemic condi-tions could contraindicate the procedure. The search for new, less-inva-sive techniques which could eventually replace biopsy and simplify the diagnostic process would beneit both professionals and patients.1-3
As-piration is recommended in submucosal lesions or in those cases where a very thin layer of cortical bone persists.1 The collected material should
irst be visually examined, with a special focus on color and consistency. However, this material is frequently discarded without being properly re-ferred for laboratory analysis.1
The cell block technique is a histological approach, often used in medical pathology,which consists of aspirating the lesion with the use of an 18-gauge needle followed by laboratory processing.2 The aspirated
material is centrifuged, parafin-embedded, cut, stained, and histologi-cally analyzed. The great advantage of cell blocks in these cases is the Declaration of Interests: The authors
decrease in cell dispersion.2
The aim of this study was to evaluate the viabili-ty of the cell block technique as an auxiliary method for the diagnosis of maxillary bone lesions with a cystic aspect.
Methodology
This study was approved by the Human Research Ethics Committee of the authors’ institution (ap-proval number 145/08). Sampling included patients with intrabony jaw lesions with a clinical recom-mendation of aspiration, and being cared for at the Stomatology Ambulatory at the University Hospital, and at the Dental Clinic of the Federal University of Santa Catarina . All participants were volunteers who were informed about the study and were asked to sign an informed consent agreement.
Clinical procedures
All the patients underwent clinical and imaging examinations. The aspirations were performed in the same session, immediately after the examination or during the biopsy procedure. An 18-gauge needle coupled to a 20-mL syringe was inserted into the le-sion at its maximum luctuation or at the “papyrus crackling” consistency point. The aspirated material was analyzed macroscopically, and the syringe was immediately packaged in an ice-cooled container and referred to the Oral Pathology Laboratoryfor processing. An incisional or excisional biopsy was later performed according to the clinical indication for each case. The treatment prescribed followed pre-established protocols by the respective services.
Laboratory procedures
The material was removed from the syringe, transferred to a test tube, and centrifuged at 1500 rpm for 20 min. The pellet obtained after cen-trifugation was transferred to absorbent paper and ixed in a 10% formaldehyde solution for 24 h. Af-ter that, the maAf-terial was sequentially processed as follows:
• dehydration,
• diaphanization,
• impregnation, and
• embedment in parafin.
Three-micrometer-thick sections were obtained and stained with haematoxylin-eosin (H&E). The cell block slides were analyzed by light microscopy (Axiostar Plus; Carl Zeiss, Oberkochen, Germany) for evaluation of the presence of epithelial cells, acute and chronic inlammatory cells, keratin, and cholesterol crystal clefts. This evaluation was per-formed by a calibrated examiner, irst independently and later by consensus with an oral pathologist. The biopsied tissues were subjected to routine processing for the histopathological diagnosis of the lesions.
Statistical analysis
From the cell block data and histopathology analyses, a database was created with the SPSS soft-ware package (“Statistical Package for the Social Sciences” for Windows, version 16.0, SPSS Inc., Chicago, IL, USA). The chi-square test was used to check the occurrence of variable associations at a 5% signiicance level.
Results
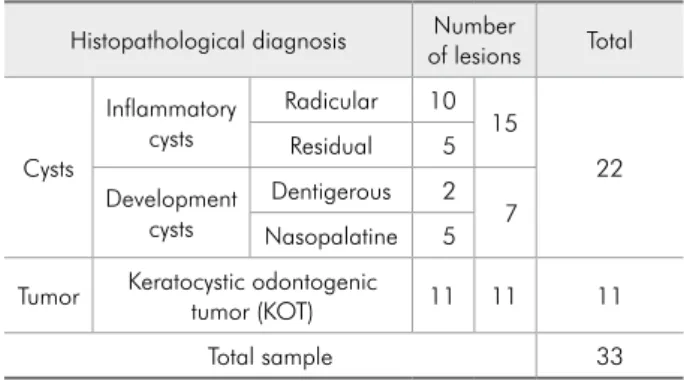
The inal sample consisted of 33 patients, 20 (60.6%) male and 13 (39.4%) female, with a mean age of 41 years, ranging from 9 to 73 years. The complete proile of the sample is shown in Table 1.
The data for the association of cell block features with histopathological diagnosis are shown in Table 2. There was a statistically signiicant association between cystic lesions and cholesterol crystal cleft occurrence, between KOT and epithelial cell rence, and between KOT and parakeratin occur-rence.
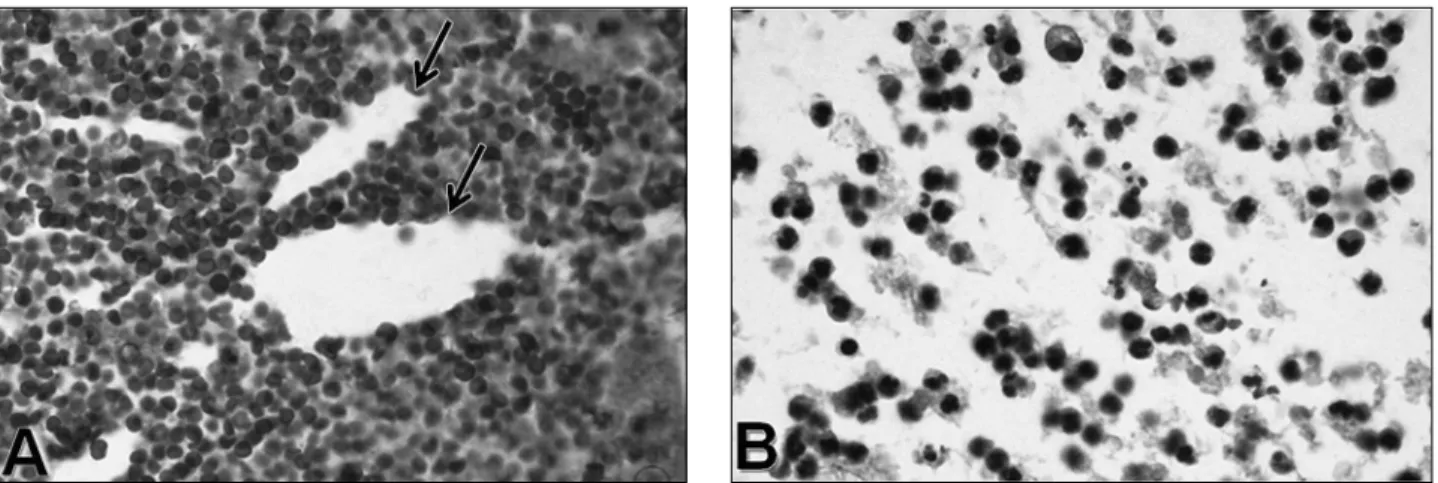
All KOT cases (n = 11) included in this study
Table 1 - Description of the lesion sample.
Histopathological diagnosis of lesionsNumber Total
Cysts
Inflammatory cysts
Radicular 10 15
22
Residual 5
Development cysts
Dentigerous 2 7 Nasopalatine 5
Tumor Keratocystic odontogenic tumor (KOT) 11 11 11
showed parakeratin in cell block preparations (Fig-ure 1A). Among 22 cystic lesions, 15 (68.2%) re-vealed the presence of cholesterol crystal clefts (Fig-ure 2A). These clefts were also found in one KOT case that showed an intense inlammation upon his-topathological examination. Epithelial cells result-ing from desquamation were found in 7 KOT cases (Figure 1B) and in a nasopalatine duct cyst.
Discussion
Biopsy may be complex at some maxilloman-dibular sites, such as the manmaxilloman-dibular ramus and condylar lesions, due to the dificulty of surgical ac-cess.4-6 Systemic conditions either contraindicate
bi-opsy or render it dificult. In these cases, aspiration
could be indicated to verify the absence or presence of blood or liquid inside a mandibular lesion, to al-low for an evaluation of the coloration, consistency, and amount of the material extracted.1 Fine-needle
aspiration cytology (FNAC) is a valuable resource, especially to differentiate malignant from benign le-sions.3,7 However, the use of this technique for jaw
lesions is not unanimously accepted.2,3,7-9 In this
study, the biopsies were performed with thicker-gauge needles, followed by the processing of the aspirated material by the cell block technique, with the goal of decreasing cell dispersion and providing a larger amount of material for analysis.
The occurrence of inlammatory cells was an expected inding in aspirations of inlammatory
Cell block feature Histopathological diagnosis Feature occurrence Total p-value
Yes No
Chronic inflammation Cysts 20 2 22 0.1514
KOT 7 4 11
Acute inflammation Cysts 19 3 22 0.6321
KOT 8 3 11
Cholesterol crystal clefts Cysts* 15 7 22 0.0046*
KOT 1 10 11
Epithelial cells Cysts 1 21 22 0.0010*
KOT* 7 4 11
Parakeratin Cysts 0 22 22 < 0.0001*
KOT* 11 0 11
* Statistically significant.
Table 2 - Association between histopathological diagnosis and cellular features detected by cell block, comparing cystic lesions with KOT.
origin, since leukocyte transmigration toward the radicular and residual cyst epithelium is common.1
Nonetheless, a statistically signiicant association between the occurrence of inlammatory cells and the lesions in this study was not found. Other au-thors,8 upon examining maxillary aspirates through
FNAC, found a large quantity of inlammatory cells in radicular cysts, in addition to ibromyxoid tissue and epithelial cells. Despite the lack of statistical relevance, probably due to the small sample in our study, in a comparison of cytological slides of radic-ular cysts (Figure 2B) with those of residual cysts, inlammatory cells were found to be more abundant in the former. This can be explained by the continu-ous contact of the lesion with bacterial components from the tooth root canal, presenting devitalized pulp.
A statistically signiicant association between cysts and cholesterol crystal clefts was found. Cho-lesterol crystal clefts have been reported in the lu-men and/or inlammatory cyst capsule.10 Epithelial
cell occurrence showed a statistically signiicant association with KOTs. Such indings can be ex-plained by the high epithelial proliferation rate of these tumors, which is responsible for the growth mechanism of these lesions.11,12 The smooth junction
between the thin epithelium and the connective tis-sue of the capsule12 may also be a likely source of
stimulation for the desquamation process.
All KOTs (n = 11) showed parakeratin. In cyto-logical indings by August et al.,8 only one out of
3 KOTs analyzed showed keratin. However, these authors used a fast staining method or immediate ixation in ethanol without centrifugation and em-bedment, which generated an inevitable loss of ma-terial for analysis, due to the typical cell dispersion of these materials. Radhika et al.13 stated that, when
liquid is aspirated from extensive lesions, its centrif-ugation can improve diagnosis due to the concentra-tion of lesion-typical cells.
The literature shows that FNAC, with or with-out cell block association, is a valuable diagnostic technique for other jaw lesions, such as giant-cell lesions and ameloblastomas.13-17 However, it is
im-portant to emphasize that cytology is more complex than histology in maxillary lesions,15 and that
fur-ther studies should be developed on this matter so that a better understanding of the cytological fea-tures of these lesions can be achieved.
Conclusion
A preliminary diagnosis of cystic lesions and KOTs can be conducted by the cell block technique. The occurrence of cholesterol crystal clefts in cell block slides suggests cystic lesions. The presence of parakeratin in the cytological analysis is highly sug-gestive of KOT, eliminating the need for incisional biopsy in the therapeutic planning for these lesions.
References
1. Rivero ERC, Grando LJ, Menegat F, Claus JDP, Xavier FM. Cell block technique as a complementary method in the clini-cal diagnosis of cyst-like lesions of the jaw. J Appl Oral Sci. 2011 May-Jun;19(3):269-73.
2. Karnachow PN, Bonin RE. Cell block technique for fine needle aspiration biopsy. J Clin Pathol. 1982 Jun;35(6):688. 3. Günhan Ö, Dog˘an N, Celasun B, S¸engün O, Önder T, Finci
R. Fine-needle aspiration cytology of oral cavity and jaw bone lesions – a report of 102 cases. Acta Cytol. 1993 Mar- Apr;37(2):135-41.
4. Zadik Y, Aktas¸ A, Drucker S, Nitzan DW. Aneurysmal bone cyst of mandibular condyle: A case report and review of the literature. J Craniomaxillofac Surg. 2011 Nov 25; [Epub ahead of print]. Available from: http://www.sciencedirect.com/sci-ence/article/pii/S1010518211002551.
5. Pace C, Holt D, Payne M. An unusual presentation of an ectopic third molar in the condylar region. Aust Dent J. 2010 Sep;55(3):325-7.
6. Sembronio S, Albiero AM, Zerman N, Costa F, Politi M. Endoscopically assisted enucleation and curettage of large mandibular odontogenic keratocyst. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009 Feb;107(2):193-6. 7. Santos APC, Sugaya NN, Pinto Junior DC, Lemos Junior CA.
Fine needle aspiration biopsy in the oral cavity and head and neck region. Braz Oral Res. 2011 Apr;25(2):186-91. 8. August M, Faquin CW, Ferraro N, Kaban L. Fine-needle
aspiration biopsy of intraosseous lesions. J Oral Maxillofac Surg. 1999 Nov;57(11):1282-6.
9. Baykul T, Colok G, Gunhan O. The value of aspiration cytol-ogy in cystic lesions of the maxillofacial region. Eur J Dent. 2010 Jan;4(1):1-5.
10. Koseoglu BG, Atalay B, Erdem MA. Odontogenic cysts: a clinical study of 90 cases. J Oral Sci. 2004 Dec;46(4):253-7. 11. Shear M. The aggressive nature of odontogenic keratocyst; is
it a benign cystic neoplasm? Part 2: Proliferation and genetic studies. Oral Oncol. 2002 Jun;38(4):323-31.
12. Bhargava D, Deshpande A, Pogrel MA. Keratocyst odonto-genic tumour (KCOT) - a cyst to a tumor. Oral Maxillofac Surg. 2011 Nov 11; [Epub ahead of print]. Available from: http://www.springerlink.com/content/6676558313067151/. 13. Radhika S, Nijhawan R, Das A, Dey P. Ameloblastoma of the
mandible: diagnosis by fine-needle aspiration cytology. Diagn Cytopathol. 1993;9(3):310-3.
14. Castro WH, Filho EC, de Souza PE, Gomez RS. Immunocy-tochemistry of fine-needle aspirates from central giant cell granuloma. Br J Oral Maxillofac Surg. 1998 Aug;36(4):301-3. 15. Gunhan O, Finci R, Celsaun B, Demiriz M. A case of am-eloblastoma diagnosed by fine-needle aspiration cytology. J Nihon Univ Sch Dent. 1989 Dec;31(4):565-9.
16. Stamatakos MM, Houston CGD, Fowler LCGB, Boyd ME, Solanki CPH. Diagnosis of ameloblastoma of the maxilla by fine needle aspiration: a case report. Acta Cytol. 1995 Jul-Aug;39(4):817-20.