ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Has
the
median
nerve
involvement
in
rheumatoid
arthritis
been
overemphasized?
Rajalingham
Sakthiswary
a,∗,
Rajesh
Singh
baUniversitiKebangsaanMalaysiaMedicalCentre(UKMMC),DepartmentofMedicine,Cheras,Malaysia
bMonashUniversityMalaysia,JeffreyCheahSchoolofMedicineandHealthSciences,DepartmentofOrthopaedics,BandarSunway,
Malaysia
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received18September2015 Accepted5July2016
Availableonline30September2016
Keywords:
Mediannerve Rheumatoidarthritis Carpaltunnelsyndrome
a
b
s
t
r
a
c
t
Rheumatoidarthritis(RA)isawellandwidelyrecognizedcauseofcarpaltunnelsyndrome (CTS).Intherheumatoidwrist,synovialexpansion,jointerosionsandligamentouslaxity resultincompressionofthemediannerveduetoincreasedintracarpalpressure.We evalu-atedthepublishedstudiestodeterminetheprevalenceofCTSandthecharacteristicsofthe mediannerveinRAanditsassociationwithclinicalparameterssuchasdiseaseactivity, dis-easedurationandseropositivity.Atotalof13studiesmettheeligibilitycriteria.Pooleddata from8studieswithrandomselectionofRApatientsrevealedthat86outof1561(5.5%) sub-jectshadCTS.SubclinicalCTS,ontheotherhand,hadapooledprevalenceof14.0%(30/215). ThecrosssectionalareaofthemediannerveoftheRApatientswithoutCTSweresimilarto thehealthycontrols.Thevastmajorityofthestudies(8/13)disclosednosignificant relation-shipbetweenthemediannervefindingsandtheclinicalorlaboratoryparametersinRA.The linkbetweenRAandthemediannerveabnormalitieshasbeenoveremphasizedthroughout theliterature.TheprevalenceofCTSinRAissimilartothegeneralpopulationwithoutany correlationbetweenthemediannervecharacteristicsandtheclinicalparametersofRA.
©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
O
envolvimento
do
nervo
mediano
na
artrite
reumatoide
tem
sido
excessivamente
valorizado?
Palavras-chave:
Nervomediano Artritereumatoide Síndromedotúneldocarpo
r
e
s
u
m
o
Aartritereumatoide(AR)éumacausabemeamplamentereconhecidadesíndromedotúnel docarpo(STC).Nopunhoacometidopelaartritereumatoide,aexpansãosinovial,aserosões articulareseafrouxidãoligamentarresultamemcompressãodonervomedianodecorrente doaumentoda pressão intracarpal.Avaliaram-se os estudospublicados para determi-naraprevalênciadeSTCeascaracterísticasdonervomedianonaAResuaassociac¸ão comparâmetros clínicos, como a atividadee durac¸ão da doenc¸ae a soropositividade.
∗ Correspondingauthor.
E-mail:[email protected](R.Sakthiswary). http://dx.doi.org/10.1016/j.rbre.2016.09.001
Preencheramoscritériosdeelegibilidade13estudos.Osdadosagrupadosdosoitoestudos comselec¸ãoaleatóriadepacientescomARrevelaramque86de1.561(5,5%)indivíduos tin-hamSTC.Poroutrolado,aSTCsubclínicateveumaprevalênciacombinadade14%(30/215). Aáreadesec¸ãotransversadonervomedianodospacientescomARsemSTCfoisemelhante àdecontrolessaudáveis.Agrandemaioriadosestudos(8/13)nãoapresentourelac¸ão signi-ficativaentreosachadosnonervomedianoeosparâmetrosclínicosoulaboratoriaisnaAR. Aligac¸ãoentreaAReasanormalidadesdonervomedianofoiexcessivamentevalorizada emtodaaliteratura.AprevalênciadeSTCnaARésemelhanteàdapopulac¸ãoemgeral, semqualquercorrelac¸ãoentreascaracterísticasdonervomedianoeosparâmetrosclínicos daAR.
©2016ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Beyondthejoints,rheumatoidarthritis(RA)maypresentwith extra-articular manifestations such as pulmonary fibrosis,
subcutaneousnodules and peripheralneuropathy in up to
10–20%ofpatients.1Thewrististhemostfrequentlyaffected jointinRAwithcarpaltunnelsyndrome(CTS)asapotential sequelae.Intherheumatoidwrist,synovialexpansion,joint erosionsandligamentouslaxityresultinlossofcarpaltunnel heightandincreasedcarpaltunnelpressure.Thiscontributes
to impaired axonal transport, compression of the median
nerveandvesselsintheperineuriumcausingmediannerve ischemia.2,3Theotherplausibleculpritmechanismsthathave beenimplicatedinrheumatoidneuropathyaredrugtoxicity, vasculitisandamyloidosis.4
Carpal tunnelsyndrome(CTS) isbyand large aclinical diagnosis,althoughelectrophysiologicaltests(nerve conduc-tionstudies[NCS],electromyography[EMG])andsonographic
assessment of the median nerve may be useful to
sup-portthediagnosis,detectsubclinicalCTSandruleoutother abnormalities.5Unfortunately,theneuropathicpaininRAis oftenoverlookedandmistakenforarthriticpain.6
Hartetal.wasthefirst todescribeneuropathyinRAin year1957.7Sincethen,severalelectrophysiologicaland sono-graphicstudieshaveexaminedthemediannerveinRAwith variable findings.Thepurposeofthis systematicreview, is therefore,tosummarize theresultsofthesestudiesand to determineinRAtheprevalenceofCTS,characteristicsofthe mediannerveanditsassociationwiththeclinicalparameters suchasdiseaseactivity,diseasedurationandseropositivity.
Methods
Searchstrategy
We searched the literature for clinical studies on median nerve inRA usingthe followingdatabases:Science Direct, Pubmed/Medline,Ovid,ISIWebofKnowledge,EBSCOand Sco-pus.These searchterms used were “rheumatoidarthritis”, “mediannerve,”“carpaltunnelsyndrome”and“neuropathy”. Toensurecompleteness,wewentthroughpapersnotonlyon CTSexplicitlybutalsoonlessspecificconditionsthatmight encompassthemediannerve/CTSlikeperipheralneuropathy.
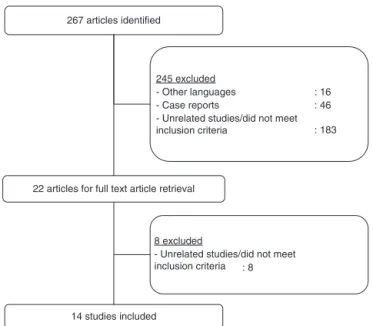
267 articles identified
245 excluded
: 16 - Other languages
: 46 - Case reports
- Unrelated studies/did not meet inclusion criteria : 183
8 excluded
: 8 - Unrelated studies/did not meet inclusion criteria 22 articles for full text article retrieval
14 studies included
Fig.1–Thealgorithmforselectionofstudiesinthis systematicreview.
Theabstractsofthestudieswerescrutinizedfor appropriate-nessbeforeretrievingthefulltextofthearticles.Wesearched thebibliographiesofallrelevantpublishedarticlestoavoid missingother relevantstudies.Fig.1summarizesthe algo-rithmusedforselectionofthestudies.Ethicsapprovalwas notrequiredforthissystematicreviewastherewasno recruit-mentofsubjectsorresearchintervention.
Selectioncriteria
Inclusioncriteria
The search was further refined to achieve a high level of homogeneityacrosstheselectedstudies.Weappliedatime restrictiontostudiespublishedfromyear1980onwards.We includedstudiesaboutRAwhich:
1. examinedthemediannervecharacteristics(sonographic and/orelectrophysiological),
2. wereaboutCTS,
Exclusioncriteria
We excluded case reports and review articles. Studies on peripheralneuropathywhichdidnotprovidespecificdataon themediannervewerenotconsideredeither.
Dataextraction
Thefollowingdatawereextractedfromallstudiesincludedin thissystematicreview:studydesign,studypopulation includ-ing the detailsofthe controlarm, samplesize, prevalence
of CTS in RA, median nerve characteristics in RA
(sono-graphicand electrophysiological), the relationship between themediannervecharacteristicsandtheclinicalparameters. Therelevantandespeciallysignificantstatisticalvalues(pand
rvalues)wererecorded.
Results
Atotalof13studies.6,8–19mettheeligibilitycriteria.Majority ofthestudies(12/13)werecross-sectional,andtherewere5 case-controlstudies.9,10,12,13,18Thecontrolsemployedbythe studieswereeitherhealthyindividuals9,10,13,18orRApatients withoutsymptomsofCTS.9Studysamplesizesvariedfrom 2314to107016subjects.Twoofthestudies11,14dealtwith sub-clinicalCTSi.e.conductedamongsubjectswithoutsignsand symptomsofCTS.Tables1and2highlightthefindingsofthe selectedstudies.
PrevalenceofCTSinRA
Inmoststudies,thediagnosisofCTSwasbasedona combi-nationofsymptoms(paraesthesia,tinglingsensation,painat themediannerveinnervatedarea),signs(positiveTinel’sor Phalentest)andelectrophysiologicalfindings.Theexact diag-nosticcriteriaanddefinitionofCTSusedacrossthestudies werequitediverse.Hammeretal.12definedCTSbasedona palm-to-wristmediansensorynerveactionpotential(SNAP) onsetlatencyof>2.0msorabsenceofSNAPandmediandistal motorlatencyof>4.9mswhereasSimetal.18definedCTSas apalmtowristmediannervelatencyoflessthan50%.The prevalenceofCTSinRArangedfrom3.5%16to22.8%.17Pooled datafrom8studies6,8,9,13,15–17,19withrandomselectionofRA patientsrevealedthat86outof1561(5.5%)subjectshadCTS. SubclinicalCTS,ontheotherhand,hadapooledprevalence of14.0%(30/215)(Table2).
SonographicfindingsofthemediannerveinRA
Cross-sectionalarea (CSA) ofthe mediannerve was deter-mined using ultrasound scan in 3of the studies.11–13 Two outof3ofthesestudies12,13wereofcase–controldesignwith healthyindividualsascontrols.Hammeretal.11investigated RApatientswithoutsignsandsymptomsofCTS.TheCSAof thebilateral mediannerve oftheRApatients withoutCTS weresimilartothehealthycontrols.Themean(standard devi-ation)oftherightmediannerveinasymptomaticRApatients was8.3(1.5)mm2whereasfortheleftmediannervewas8.3 (1.4)mm2.11TheCSAofthemediannerveinCTSpatientswere significantlyhigherwithamedianof15.7mm2(11.1–21.8).12
ElectrophysiologicalfindingsofthemediannerveinRA
Electrophysiologicalassessmentofthemediannervewas car-riedoutin10/136,8–10,12,14–16,18,19ofthestudies.Detailsofthe NCS intermsofthe mediannerve velocity,amplitude and latencywereprovidedonlyby2studiesi.e.Lanzilloetal.10 andCalderetal.15Theformerstudyreportedthatthemedian nervesensoryconductionvelocitywasreducedby25.2%along thedistalnervesegmentin57.5% ofRApatientscompared
to the general population. The amplitude of the sensory
responseswassignificantlyreducedatthewristandelbow in 17.5% and 5%ofpatients, respectively. Distal latencyto the abductorpollicisbrevismusclewassignificantlyslower in10%ofthepatientswhereasthemaximumvelocityfrom
the elbowto the wrist was prolonged by 12% in almost a
quarterofthesubjects.Calderetal.,10foundthatthemedian nerveSNAPamplitudewassignificantlylowerintheRAand handosteoarthritisgroupscomparedtothehealthycontrols (p<0.05) but there were no appreciable differences in the mediannerveSNAPconductionvelocityandlatencybetween theRApatientsandthehealthycontrols.Itisnoteworthythat thisstudyhadanextremelysmallsamplesizewithonly8RA patients.
Correlationbetweenthemediannervecharacteristicsand theclinicalparameters
Across the studies, the most frequently assessed clinical parameter was disease duration (9/13 studies)6,8,11,13–18 as comparedtodiseaseactivity(4/13studies).6,8,9,13Apartfrom
the above mentioned, the following clinical and
labora-tory parameters were commonly analyzed by the selected
studies; age, height, weight, medications, rheumatoid fac-tor(RF),erythrocytesedimentationrate(ESR)andC-reactive
protein (CRP). Approximately half of these studies were
designed to compare the patients’ characteristics between RApatientswithandwithoutCTS13,16 orwithand without neuropathy.6,8,17,18Thevastmajorityofthestudies(8/13) dis-closednosignificantrelationshipbetweenthemediannerve involvementandclinicalorlaboratoryparametersinRA. How-ever,Karadagetal.13andBiswasetal.6revealedasignificant associationbetweendiseasedurationandtheoccurrenceof CTS (p=0.036)andneuropathy(p=0.001),respectively. Like-wise,2studiesfoundthatagewassignificantlyhigheramong RApatientswithCTS13andperipheralneuropathy.18
Discussion
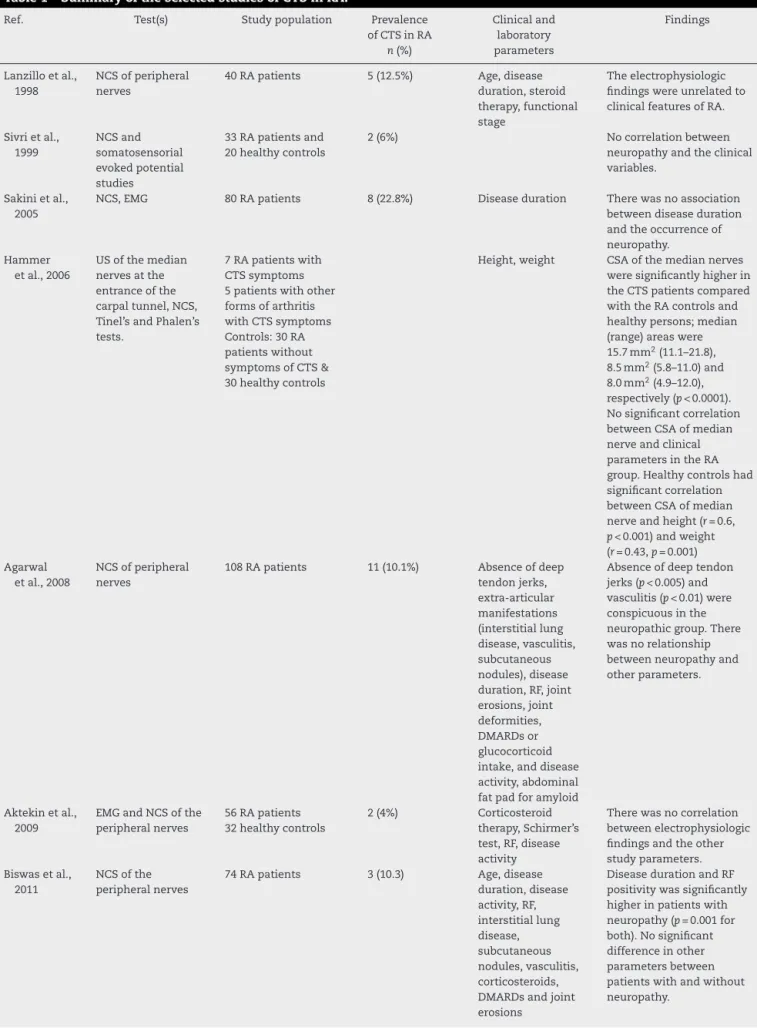
Table1–SummaryoftheselectedstudiesofCTSinRA.
Ref. Test(s) Studypopulation Prevalence
ofCTSinRA n(%)
Clinicaland laboratory parameters
Findings
Lanzilloetal., 1998
NCSofperipheral nerves
40RApatients 5(12.5%) Age,disease
duration,steroid therapy,functional stage
Theelectrophysiologic findingswereunrelatedto clinicalfeaturesofRA.
Sivrietal., 1999
NCSand somatosensorial evokedpotential studies
33RApatientsand 20healthycontrols
2(6%) Nocorrelationbetween
neuropathyandtheclinical variables.
Sakinietal., 2005
NCS,EMG 80RApatients 8(22.8%) Diseaseduration Therewasnoassociation
betweendiseaseduration andtheoccurrenceof neuropathy.
Hammer etal.,2006
USofthemedian nervesatthe entranceofthe carpaltunnel,NCS, Tinel’sandPhalen’s tests.
7RApatientswith CTSsymptoms 5patientswithother formsofarthritis withCTSsymptoms Controls:30RA patientswithout symptomsofCTS& 30healthycontrols
Height,weight CSAofthemediannerves weresignificantlyhigherin theCTSpatientscompared withtheRAcontrolsand healthypersons;median (range)areaswere 15.7mm2(11.1–21.8), 8.5mm2(5.8–11.0)and 8.0mm2(4.9–12.0), respectively(p<0.0001). Nosignificantcorrelation betweenCSAofmedian nerveandclinical parametersintheRA group.Healthycontrolshad significantcorrelation betweenCSAofmedian nerveandheight(r=0.6, p<0.001)andweight (r=0.43,p=0.001) Agarwal
etal.,2008
NCSofperipheral nerves
108RApatients 11(10.1%) Absenceofdeep tendonjerks, extra-articular manifestations (interstitiallung disease,vasculitis, subcutaneous nodules),disease duration,RF,joint erosions,joint deformities, DMARDsor glucocorticoid intake,anddisease activity,abdominal fatpadforamyloid
Absenceofdeeptendon jerks(p<0.005)and vasculitis(p<0.01)were conspicuousinthe neuropathicgroup.There wasnorelationship betweenneuropathyand otherparameters.
Aktekinetal., 2009
EMGandNCSofthe peripheralnerves
56RApatients 32healthycontrols
2(4%) Corticosteroid
therapy,Schirmer’s test,RF,disease activity
Therewasnocorrelation betweenelectrophysiologic findingsandtheother studyparameters. Biswasetal.,
2011
NCSofthe peripheralnerves
74RApatients 3(10.3) Age,disease
duration,disease activity,RF, interstitiallung disease, subcutaneous nodules,vasculitis, corticosteroids, DMARDsandjoint erosions
Table1– (Continued)
Ref. Test(s) Studypopulation Prevalence
ofCTSinRA n(%)
Clinicaland laboratory parameters
Findings
Calderetal., 2012
NCSofthe peripheralnerves, sensorymapping (SM),vibratoryand currentperception thresholds(VPTand CPT)ofthe2ndand 5thdigits
7womenwithRA 9healthywomen 11womenwith handOA
AllSNAPamplitudeswere significantlylowerforthe handOAandhandRA groupscomparedwiththe healthygroup(p<0.05).No groupdifferenceswere foundforSNAPconduction velocities,SM,VPT,and CPT.
Karadag etal.,2012
Katzhanddiagram, BostonCTS questionnaire, PhalenandTinel tests.
USofwristjoints andcarpaltunnel grayscaleandpower Doppler.
Patientswith mediannerveCSA between10.0and 13.0mm2were evaluatedwith electromyography (EMG)
100RApatients 45healthycontrols
18(18%) Age,gender,body massindex,disease duration,goiter, diseaseactivity, HAQ-DI,ESR,CRP, CTSglobal assessment,CTS symptomduration, Bostonsymptom severityscore, Bostonfunctional status
InRAgroupwithCTS:age (57[36–73]vs.50[24–76], p=0.041),historyofDM (35.3%vs.6.0%,p<0.001), diseaseduration(108 [12–396]monthsvs.72 [6–360]months,p=0.036), HAQ-DIscore(1.93 [0.75–2.87]vs.1.13[0–2.75], p=0.013),CTSpatient globalscore(52[1–97]vs.25 [0–91],p=0.001),Boston symptomseverity(2.81 [1.18–4.17]vs.2.0[1.0–4.01], p=0.01)andfunctional statusscores(3.37[1.37–5.0] vs.2.25[1.0–5.0],p=0.008) wereelevatedcomparedto patientswithoutCTS. Simetal.,
2014
NCS,Neuropathic SymptomsScale (NSS)
30RApatientswith symptomsof peripheral neuropathy
7(23.3%) Age,anti-CCP,the typeofmedication, diseaseduration, functionalstatus, neuropathic symptoms,ESR,CRP
Themeanagesofthe patientswithandwithout peripheralneuropathywere 69.4and56.5years, respectively(p<0.05).
Leeetal., 2015
EMG,NCS,Phalen’s andTinel’stests
1070RApatients 37(3.5%) CRP,disease duration
Therewasnostatistically significantcorrelation betweenCTSoccurrence anddurationofRAandCRP levels.
EMG,electromyography;NCS,nerveconductionstudies;RF,rheumatoidfactor;ESR,erythrocytesedimentationrate;CRP,C-reactiveprotein; CTS,carpaltunnelsyndrome;RA,rheumatoidarthritis;HAQ-DI,HealthAssessmentQuestionnaire–disabilityindex;OA,osteoarthritis;DMARD, diseasemodifyingantirheumaticdrug.
14.0%waswithinthereportedrangeinthegeneralpopulation of7–16%.24
Inhealthyindividuals,themeanCSAofthemediannerve atthelevelofentranceintothecarpaltunnel,whichhasthe highestdiagnosticsensitivityandspecificityforCTS,hasbeen foundto bebetween 7.0±1.0mm2 and 10.2±2.5mm2.25–27
ThemeanCSAofthemediannerveinRApatientswithout
signsandsymptomsofCTSweresimilartohealthycontrols. Thislendscredencetothenotionthatthechronic inflamma-toryprocessesinRAdonotaffectthesizeofthemediannerve despitethecloseproximitybetweenthemediannerveand thewristjoint.However,Yagcietal.28hadcontradicting find-ingsofRApatientshavinglargerCSAofthemediannerve despiteabsence ofclinicalandneurophysiological evidence ofCTS.
No firm conclusions can be made on the
electrophysi-ological changes of the median nerve in RA owing to the
paucityofstudiesinthisregardandtheconflictingfindings oftheexistingstudies.AlthoughLanzilloetal.15revealedthat morethanhalfofRApatientswithoutsymptomsofCTShad reducedmediannervesensoryconductionvelocityalongthe distalnerve segment,this study failedtodemonstrate any correlationbetweentheclinicalparametersofRAandthe elec-trophysiologicalfindings.Ofnote,thisstudyhadthedrawback ofnothavingacontrolarmandtherefore,comparisonwas madewithdatafromotherpublishedstudies.
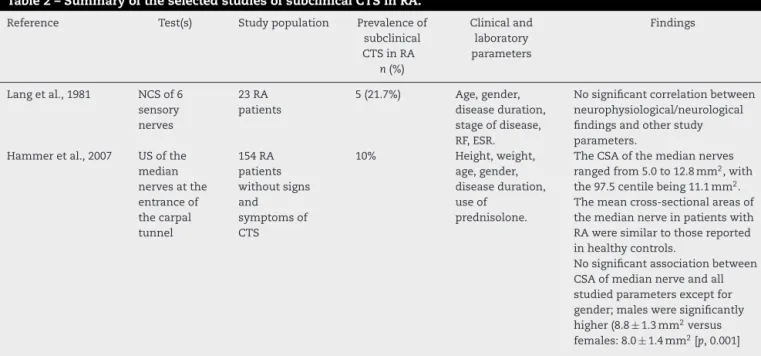
Table2–SummaryoftheselectedstudiesofsubclinicalCTSinRA.
Reference Test(s) Studypopulation Prevalenceof
subclinical CTSinRA
n(%)
Clinicaland laboratory parameters
Findings
Langetal.,1981 NCSof6 sensory nerves
23RA patients
5(21.7%) Age,gender, diseaseduration, stageofdisease, RF,ESR.
Nosignificantcorrelationbetween neurophysiological/neurological findingsandotherstudy parameters.
Hammeretal.,2007 USofthe median nervesatthe entranceof thecarpal tunnel
154RA patients withoutsigns and symptomsof CTS
10% Height,weight,
age,gender, diseaseduration, useof
prednisolone.
TheCSAofthemediannerves rangedfrom5.0to12.8mm2,with the97.5centilebeing11.1mm2. Themeancross-sectionalareasof themediannerveinpatientswith RAweresimilartothosereported inhealthycontrols.
Nosignificantassociationbetween CSAofmediannerveandall studiedparametersexceptfor gender;malesweresignificantly higher(8.8±1.3mm2versus females:8.0±1.4mm2[p,0.001]
NCS,nerveconductionstudies;RF,rheumatoidfactor;ESR,erythrocytesedimentationrate;CTS,carpaltunnelsyndrome;RA,rheumatoid arthritis.
scores were higher among the RA patients with CTS, the
remaining studies were not in agreement with the above
findings.However,numerousstudieswhichinvestigatedthe extra-articular manifestations of RA, in general, identified thefollowing factorsas predictorsin thisregard:high dis-easeactivity,smoking,antinuclearantibodiesandrheumatoid nodules.29,30
Thestudies includedinthissystematicreviewwere not withouttheirindividuallimitations.Inparticular,manyhad a small sample size, hence limiting the statistical power. Many of the studies did not fully control for confounding
factors of CTS such as occupation, the presence of
dia-betesmellitusandhypothyroidism.DefinitionofCTSvaried substantiallyacrossthestudies.MisclassificationasCTS, par-ticularlyamongstudiesthatdiagnosedCTSsolelybasedon symptoms,wasanotherpotentialsourceoferror.
Inconclusion,thenexusbetweenRAandthemediannerve
abnormalitiesorCTShasbeenoveremphasized throughout
theliterature.Basedonthissystematicreview,asubstantial bodyofresearchsuggeststhattheprevalenceofCTSinRA issimilartothegeneralpopulationwithoutanycorrelation betweenthemediannervefindingsandtheclinical parame-tersofRA.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
Theauthorwould liketothankthelibrariansof“Universiti KebangsaanMalaysia”fortheirassistanceinretrievingthefull textofthearticles.
r
e
f
e
r
e
n
c
e
s
1.TuressonC,O’FallonWM,CrowsonCS,GabrielSE,Matteson EL.Occurrenceofextraarticulardiseasemanifestationsis associatedwithexcessmortalityinacommunitybased cohortofpatientswithrheumatoidarthritis.JRheumatol. 2002;29:62–7.
2.ShapiroJS.Thewristinrheumatoidarthritis.HandClin. 1996;12:477–98.
3.AmirfeyzR,GozzardC,LeslieIJ.Handelevationtestfor assessmentofcarpaltunnelsyndrome.JHandSurgBr. 2005;30:361–4.
4.GoldingDN.Rheumatoidneuropathy.BrMedJ.1971;2:169. 5.BlandJD.Carpaltunnelsyndrome.CurrOpinNeurol.
2005;18:581–5.
6.BiswasM,ChatterjeeA,GhoshSK,DasguptaS,GhoshK, GangulyPK.Prevalence,types,clinicalassociations,and determinantsofperipheralneuropathyinrheumatoid patients.AnnIndianAcadNeur.2011;14:194–7. 7.HartFD,GoldingJR,MackenzieDH.Neuropathyin
rheumatoiddisease.AnnRheumDis.1957;16:471–80. 8.AgarwalV,SinghR,WiclafChauhanS,TahlanA,AhujaCK,
GoelD,etal.Aclinical,electrophysiological,andpathological studyofneuropathyinrheumatoidarthritis.ClinRheumatol. 2008;27:841–4.
9.AktekinLA,GozlukayaH,BodurH,BormanP,KozO. Peripheralneuropathyinrheumatoidarthritispatients:an electroneurophysiologicalstudy.TurkJRheumatol. 2009;24:62–6.
10.CalderKM,MartinA,LydiateJ,MacDermidJC,GaleaV, MacIntyreNJ.Sensorynerveactionpotentialsandsensory perceptioninwomenwitharthritisofthehand.JNeuroeng Rehabil.2012;9:27.
11.HammerHB,HaavardsholmEA,KvienTK.Ultrasonographic measurementofthemediannerveinpatientswith rheumatoidarthritiswithoutsymptomsorsignsofcarpal tunnelsyndrome.AnnRheumDis.2007;66:825–7. 12.HammerHB,HovdenIA,HaavardsholmEA,KvienTK.
mediannerveinpatientswitharthritisandcarpaltunnel syndrome.Rheumatology(Oxford).2006;45:584–8. 13.KaradagO,KalyoncuU,AkdoganA,KaradagYS,BilgenSA,
OzbakirS,etal.Sonographicassessmentofcarpaltunnel syndromeinrheumatoidarthritis:prevalenceandcorrelation withdiseaseactivity.RheumatolInt.2012;32:2313–9.
14.LangAH,KalliomakiJL,PuusaA,HalonenJP.Sensory neuropathyinrheumatoidarthritis:anelectroneurographic study.ScandJRheumatol.1981;10:81–4.
15.LanzilloB,PapponeN,CrisciC,diGirolamoC,MassiniR, CarusoG.Subclinicalperipheralnerveinvolvementin patientswithrheumatoidarthritis.ArthritisRheum. 1998;41:1196–202.
16.LeeKH,LeeCH,LeeBG,ParkJS,ChoiWS.Theincidenceof carpaltunnelsyndromeinpatientswithrheumatoid arthritis.IntJRheumDis.2015;18:52–7.
17.SakiniRA,Abdul-ZehraIK,Al-NimerMS.Neuropathic manifestationsinrheumatoidarthritis:aclinicaland electrophysiologicalassessmentinasmallsampleofIraqi patients.AnnSaudiMed.2005;25:247–9.
18.SimMK,KimDY,YoonJ,ParkDH,KimYG.Assessmentof peripheralneuropathyinpatientswithrheumatoidarthritis whocomplainofneurologicsymptoms.AnnRehabilMed. 2014;38:249–55.
19.SivriA,Guler-UysalF.Theelectroneurophysiologicalfindings inrheumatoidarthritispatients.ElectromyogrClin
Neurophysiol.1999;39:387–91.
20.AtroshiI,GummessonC,JohnssonR,OrnsteinE,RanstamJ, RosenI.Prevalenceofcarpaltunnelsyndromeinageneral population.JAMA.1999;282:153–8.
21.deKromMC,KnipschildPG,KesterAD,ThijsCT,BoekkooiPF, SpaansF.Carpaltunnelsyndrome:prevalenceinthegeneral population.JClinEpidemiol.1992;45:373–6.
22.DaleAM,Harris-AdamsonC,RempelD,GerrF,HegmannK, SilversteinB,etal.Prevalenceandincidenceofcarpaltunnel syndromeinUSworkingpopulations:pooledanalysisofsix prospectivestudies.ScandJWorkEnvironHealth.
2013;39:495–505.
23.GellN,WernerRA,FranzblauA,UlinSS,ArmstrongTJ.A longitudinalstudyofindustrialandclericalworkers: incidenceofcarpaltunnelsyndromeandassessmentofrisk factors.JOccupRehabil.2005;15:47–55.
24.FerryS,PritchardT,KeenanJ,CroftP,SilmanAJ.Estimating theprevalenceofdelayedmediannerveconductioninthe generalpopulation.BrJRheumatol.1998;37:630–5.
25.DuncanI,SullivanP,LomasF.Sonographyinthediagnosisof carpaltunnelsyndrome.AmJRoentgenol.1999;173:681–4. 26.WongSM,GriffithJF,HuiAC,LoSK,FuM,WongKS.Carpal
tunnelsyndrome:diagnosticusefulnessofsonography. Radiology.2004;232:93–9.
27.WongSM,GriffithJF,HuiAC,TangA,WongKS. Discriminatorysonographiccriteriaforthediagnosisof carpaltunnelsyndrome.ArthritisRheum.2002;46: 1914–21.
28.YagciI,AkdenizLeblebicierM,MansizKaplanB,Ozturk GokbakanD,AkyuzG.Sonographicmeasurementscanbe misleadingfordiagnosingcarpaltunnelsyndromeinpatients withrheumatoidarthritis.ActaReumatolPort.2016;41: 40–4.
29.Nyhall-WahlinBM,PeterssonIF,NilssonJA,JacobssonLT, TuressonC.Highdiseaseactivitydisabilityburdenand smokingpredictsevereextra-articularmanifestationsinearly rheumatoidarthritis.Rheumatology(Oxford).2009;48:416–20. 30.TuressonC,JacobssonL,BergstromU,TruedssonL,SturfeltG.