www.rpped.com.br
REVISTA
PAULISTA
DE
PEDIATRIA
ORIGINAL
ARTICLE
Prevalence
and
factors
associated
with
the
co-occurrence
of
health
risk
behaviors
in
adolescents
Anísio
Luiz
da
Silva
Brito
a,∗,
Carla
Meneses
Hardman
b,
Mauro
Virgílio
Gomes
de
Barros
aaUniversidadedePernambuco(UPE),Recife,PE,Brazil
bUniversidadeFederaldeSantaCatarina(UFSC),Florianópolis,SC,Brazil
Received21October2014;accepted27February2015
Availableonline28August2015
KEYWORDS
Riskbehaviors; Adolescent; Epidemiology
Abstract
Objective: Toanalyzetheprevalenceandfactorsassociatedwiththeco-occurrenceofhealth riskbehaviorsinadolescents.
Methods: Across-sectionalstudy wasperformedwithasampleofhighschoolstudentsfrom statepublicschoolsinPernambuco,Brazil(n=4207,14---19yearsold).Datawereobtainedusing aquestionnaire.Theco-occurrenceofhealthriskbehaviorswasestablishedbasedonthesum offivebehavioralriskfactors(lowphysicalactivity,sedentarybehavior,lowconsumptionof fruits/vegetables,alcoholconsumptionandtobaccouse).Theindependentvariableswere gen-der,agegroup,timeofdayattendingschool,schoolsize,maternal education,occupational status,skin color,geographicregionandplaceofresidence. Datawereanalyzed by ordinal logisticregressionwithproportionaloddsmodel.
Results: Approximately10%ofadolescentswerenotexposedtohealthriskbehaviors,while 58.5%reportedbeingexposedtoatleasttwohealthriskbehaviorssimultaneously.Therewas ahigherlikelihoodofco-occurrenceofhealthriskbehaviorsamongadolescentsintheolder agegroup,withintermediatematernaleducation(9---11yearsofschooling),andwhoreported livinginthedriest(semi-arid)regionofthestateofPernambuco.Adolescentswhoreported havingajobandlivinginruralareashadalowerlikelihoodofco-occurrenceofriskbehaviors. Conclusions: Thefindingssuggestahighprevalenceofco-occurrenceofhealthriskbehaviors inthisgroupofadolescents,withahigherchanceinfivesubgroups(olderage,intermediate maternaleducation,theonesthatreportednotworking,thoselivinginurbanareasandinthe driestregionofthestate).
©2015SociedadedePediatriadeS˜aoPaulo.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-license(https://creativecommons.org/licenses/by/4.0/).
DOIoforiginalarticle:http://dx.doi.org/10.1016/j.rpped.2015.02.002
∗Correspondingauthor.
E-mail:[email protected](A.L.S.Brito).
PALAVRAS-CHAVE
Comportamentosde risco;
Adolescente; Epidemiologia
Prevalênciaefatoresassociadosàsimultaneidadedecomportamentosderiscoà saúdeemadolescentes
Resumo
Objetivo: Analisaraprevalênciaeosfatoresassociadosàsimultaneidadedecomportamentos deriscoàsaúdeemadolescentes.
Métodos: Estudotransversalfeitocomamostrarepresentativadeestudantesdoensinomédio daredepúblicaestadualdePernambuco(n=4.207,14---19anos).Osdadosforamobtidos medi-antequestionário.Asimultaneidadedecomportamentosderiscoàsaúdefoideterminadapelo somatóriodaexposic¸ãodosadolescentesacincocomportamentosderisco(baixonívelde ativi-dadefísica,comportamentosedentário,consumoocasionaldefrutas/hortalic¸as,consumode bebidasalcoólicasetabagismo).Asvariáveisindependentesforamsexo,faixaetária,turno, portedaescola, escolaridadematerna, situac¸ãoocupacional,cordapele,região geográfica elocalderesidência.Osdadosforamanalisadospormeioderegressãologísticaordinalcom modelodeoddsproporcionais.
Resultados: Aproximadamente10%dosadolescentesnãoestavamexpostosacomportamentos derisco, enquanto58,5%apresentaram doisoumaiscomportamentosdeformasimultânea. Verificou-seelevac¸ãodasimultaneidadedecomportamentosderiscocomaumentodafaixa etária,comescolaridadematernaintermediária(9---11anosdeestudo)eresidêncianaRegião Semiárido.Adolescentesquereferiramtrabalhareaquelesqueresidiamemárearural apre-sentarammenorchancedesimultaneidadedecomportamentosderisco.
Conclusões: Osachadosindicamumaaltaprevalênciadeexposic¸ãosimultâneaa comportamen-tosderiscoàsaúdenessegrupodeadolescentes.Identificaram-secincosubgruposdemaior chancedeexposic¸ão(faixaetáriamaisalta,escolaridadematernaintermediária,aquelesque referiramnãotrabalhar,residiremáreaurbanaenaRegiãoSemiárido).
©2015SociedadedePediatriadeS˜aoPaulo.PublicadoporElsevierEditoraLtda.Esteéumartigo OpenAccesssobalicençaCCBY(https://creativecommons.org/licenses/by/4.0/deed.pt).
Introduction
Over the past decades, exposure tohealth risk behaviors hasbecome one ofthe most widely investigatedsubjects instudieswithyoungpopulations.1,2The interestin inves-tigationsfocusingonthissubjectcanbeexplained,atleast inpart,bythefactthatsuchbehaviorscanbeestablished andincorporated intothelifestyleat an earlyage,3,4and duetotheirconnectionwithbiologicalriskfactors5andthe presenceofestablishedmetabolicorcardiovasculardisease (CVD).6
The prevalence of co-occurrence of health risk behav-iorsinadolescentshasbeendescribedinseveralstudies.7---17 However, it was observed that the studies developed in Brazil, except for the survey performed by Farias Júnior etal.,15 reliedonveryspecific samples:laboratoryschool students17 and day-shiftstudents frompublic schoolsin a cityfromsouthernBrazil.16Therefore,theresultsofthese studiescannotbeextrapolatedtootherregionsofthe coun-tryduetosocioeconomicandculturalcontrasts,whichare knowntodifferentiatetheexposuretohealthriskbehaviors, asreportedbyNahasetal.18
Epidemiologicalsurveysontheco-occurrenceofhealth riskbehaviorsinadolescentsandtheirassociatedfactorscan helptoidentifyriskgroups andtomonitorthehealth lev-elsofthispopulation,whichcansupportthedevelopment ofpublicpoliciestopromotehealth,usingearlier interven-tionstrategiestopreventthesehabits.Thus,theaimofthis
studywastoanalyzetheprevalenceandfactorsassociated withco-occurrenceofhealthriskbehaviorsinadolescents.
Method
This isa secondaryanalysisof datafroma cross-sectional epidemiological survey,school-basedand statewide(state of Pernambuco, Brazil), called ‘‘Lifestyle and health risk behaviors inadolescents: fromprevalence study to inter-vention’’. The research protocol was approved by the InstitutionalReviewBoardofHospitalAgamenonMagalhães, incompliancewiththestandardsestablishedinResolutions 196and251bytheNationalHealthCouncil.
Thetargetpopulation,estimatedat352,829individuals, according to data from the Education and Culture Secre-tariatoftheStateofPernambuco,consistedofhigh-school studentsenrolledinpublicschools,aged14---19years.The following parameterswere usedtocalculate sample size: 95%confidenceinterval;samplingerrorof3%points; preva-lenceestimatedat50%(thisoptionwaschosenbasedonthe multiple factorsanalyzed in thestudy), andthe effectof sampledesign,establishedatfourtimestheminimum sam-plesize.Basedontheseparameters,thecalculatedsample sizewas4217students.
area[ZonadaMata],arid[Agreste],semi-arid[Sertão]and semi-arid regionoftheSaoFranciscoriver[Sertão doSão Francisco]),schoolsizeandshift(daytime/nighttime).The regional distribution was analyzed based on the number of students enrolled in each of the 17 GEREs (Gerências RegionaisdeEnsino--- RegionalEducationAdministration). Schoolswereclassifiedaccordingtothenumberofstudents enrolledinhighschool,accordingtothefollowingcriteria: small---lessthan200students;medium---200---499students, andlarge---500studentsormore.Studentsenrolledinthe morningandafternoonperiodsweregroupedintoasingle category (daytime students). All students in the selected classeswereinvitedtoparticipate.
Weusedclustersamplingintwostages,usingtheschool and class as the primary and secondary sampling units, respectively. In thefirststage, we performed therandom selection of the schools, aiming to include at least one schoolofeachsizebyGERE.Inthesecondstage,203classes wererandomlyselectedamongthoseexistingintheschools selectedinthefirststage.
Datacollectionwasperformedusinganadaptedversion of the Global School-Based StudentHealth Survey (GSHS) questionnaire.Thistoolhadbothfaceandcontentvalidity evaluatedbyexperts(researchersexperiencedin perform-ing epidemiological studies focused on health behaviors), andhaditsindicatorsofco-occurrencevalidityand repro-ducibilitytested inapilotstudy.Consistencyindicatorsof test---retestmeasurerangedfrommoderatetohigh(kappa coefficient=0.52---1.00)19---21formostitems.Thetest---retest reproducibilitycoefficients(kappacoefficient)ofthe meas-uresusedinthisstudywere:0.86forphysicalactivity;0.66 fortheconsumptionoffruits;0.77fortheconsumptionof vegetables;0.76foralcoholconsumption;0.62fortobacco use,and0.74forsedentarybehavior.
Data collection was carried out from April toOctober 2006.Thequestionnaireswereappliedintheclassroom.The studentswereadvisedbytwopreviouslytrainedapplicators, whichclarifiedandassisted infillingoutthedata.All stu-dentswereinformedthattheirparticipationwasvoluntary and that the questionnaires did not containany personal identification.Studentswerealsoinformedthattheycould leave thestudy atany stageof datacollection. Apassive informedconsentformwasusedtoobtain thepermission of parents for students younger than 18 years to partic-ipate in the study. Participants aged 18 or older signed theterm,indicating theiragreementtoparticipatein the study.
The dependent variable (co-occurrence of health risk behaviors)wasobtainedfromthesumoffiveriskbehaviors: low level of physical activity (<300min/week);sedentary behavior (>4h/day); occasional consumption of fruits and vegetables(<onceaday);alcoholconsumption(having con-sumed alcohol in the last 30 days), and smoking (having smoked in the last 30 days). These factors were chose becausetheyarelifestylemodifiablefactorsthatappearto bemorestronglyassociatedwithnon-communicablechronic diseases, and represent the highest global burden of dis-ease and mortality worldwide.22 Sedentary behavior was included becauseit is treatedasa distinctbehavior from lowlevelsofphysicalactivity,andithasahighprevalence inthepopulation,inadditiontobeinganimportantimpact onadolescent health.23 Informationregardingthe
descrip-tionofthesevariablescanbefoundinpreviousstudies.19---21 The obtainedresponses resulted in an outcome withzero (no risk factor present) to five identified risk behaviors. Subsequently,foranalysispurposes,theoccurrenceofrisk behaviors was divided in four categories (0, 1, 2, ≥3). The independent variables were: gender; age (14---16 or 17---19 years); school shift (daytime or nighttime); school size (small, medium or large); maternal education (low: ≤8;intermediate:9---11,orhigh:≥12years);occupational status (working/not working); ethnicity (Caucasian/non-Caucasian);geographicregion(metropolitan,forestareaor semi-arid)andplaceofresidence(urbanandrural).
The data tabulation procedure was carried out in a databasecreated withtheEpiDataEntrysoftware(version 3.1).To performthe analysis,Stata software (version10) wasused.Inthebivariateanalysis,thechi-squaretestwas usedforheterogeneityandfortrendtodeterminethe preva-lenceofco-occurrenceofhealthriskbehaviorsbycategories oftheindependentvariables.
To evaluatepossible associationsbetween independent and dependent variables, an analysis of ordinal logistic regressionwasperformedwithaproportionaloddsmodel. Theassumptionofproportionalitywasassessedbythe like-lihoodratiotest,andthesignificanceofcoefficients,bythe Wald test. Analyses werecarried out in twostages: first, bymakingsimpleregressionsoftheindependentvariables in relation tothe outcome. Then,a multivariate analysis wasperformedtodeterminewhetherthedemographicand school-relatedfactorswereassociatedornotwiththe out-come. Allindependent variablesentered the multivariate modelatthesamelevelofanalysisandwereexcludedby stepwisemethodwithbackwardelimination,usingap-value <0.2asanexclusioncriterionofvariablesduringthe mod-eling stages. These results are shown as odds ratios and respectiveconfidenceintervals.
After selecting the variables that would comprise the regression model, we tested the existence of possible collinearitybetween thegeographicregion(metropolitan, forest area or semi-arid region) and place of residence (urban and rural) covariates, and no linear association (variance inflation factor (VIF)values <10) wasidentified betweenthesetwovariables.
Results
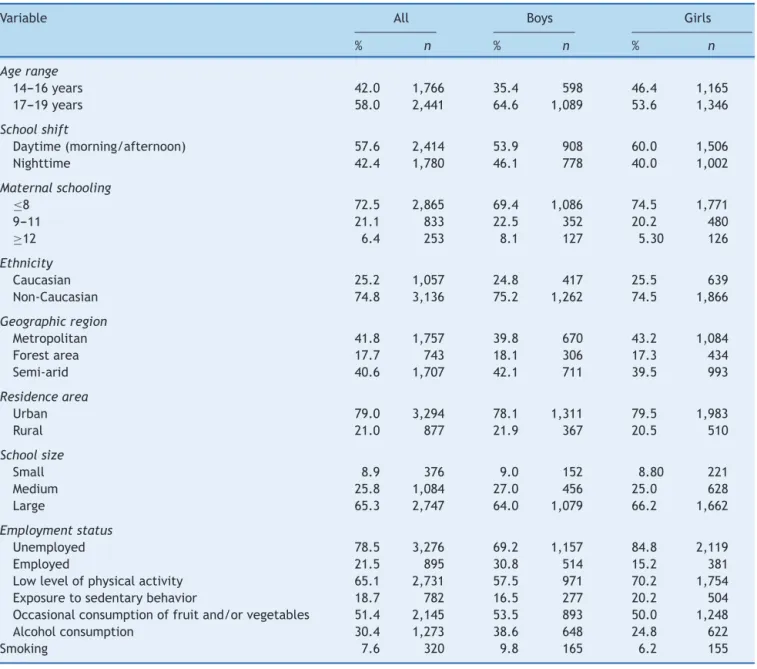
Ofthetotalofadolescentsattendingtheselectedclassesin 76assessedschools(4269),55refusedtoparticipateinthe study,andsevenwereexcludedduetoincompleteor incon-sistentdatainthequestionnaire.Thefinalsampleconsisted of4207adolescents(59.8%girls),agedbetween14and19 years(mean16.8years,SD=1.4).Othersample characteris-ticsareshowninTable1.Amongtheanalyzedvariablesin thestudy,withtheexceptionofmaternaleducation(6.1%), therateofunansweredquestionsdidnotexceed2.0%.
Table1 Samplecharacteristicsbygender.
Variable All Boys Girls
% n % n % n
Agerange
14---16years 42.0 1,766 35.4 598 46.4 1,165
17---19years 58.0 2,441 64.6 1,089 53.6 1,346
Schoolshift
Daytime(morning/afternoon) 57.6 2,414 53.9 908 60.0 1,506
Nighttime 42.4 1,780 46.1 778 40.0 1,002
Maternalschooling
≤8 72.5 2,865 69.4 1,086 74.5 1,771
9---11 21.1 833 22.5 352 20.2 480
≥12 6.4 253 8.1 127 5.30 126
Ethnicity
Caucasian 25.2 1,057 24.8 417 25.5 639
Non-Caucasian 74.8 3,136 75.2 1,262 74.5 1,866
Geographicregion
Metropolitan 41.8 1,757 39.8 670 43.2 1,084
Forestarea 17.7 743 18.1 306 17.3 434
Semi-arid 40.6 1,707 42.1 711 39.5 993
Residencearea
Urban 79.0 3,294 78.1 1,311 79.5 1,983
Rural 21.0 877 21.9 367 20.5 510
Schoolsize
Small 8.9 376 9.0 152 8.80 221
Medium 25.8 1,084 27.0 456 25.0 628
Large 65.3 2,747 64.0 1,079 66.2 1,662
Employmentstatus
Unemployed 78.5 3,276 69.2 1,157 84.8 2,119
Employed 21.5 895 30.8 514 15.2 381
Lowlevelofphysicalactivity 65.1 2,731 57.5 971 70.2 1,754
Exposuretosedentarybehavior 18.7 782 16.5 277 20.2 504
Occasionalconsumptionoffruitand/orvegetables 51.4 2,145 53.5 893 50.0 1,248
Alcoholconsumption 30.4 1,273 38.6 648 24.8 622
Smoking 7.6 320 9.8 165 6.2 155
Low level of physical activity
Occasional consumption of fruit/vegetables
Alcohol consumption
Sedentary behavior exposure
Smoking
Risk behaviors (RBs) 80
65.157.5
70.2
51.453.550.0
38.6
30.4 24.8
18.7
9.8 6.2 7.6 16.5
20.2 All
Males
Females 70
60
50
40
30
%
20
10
0
Figure1 Prevalenceofhealthrisk behaviorsinhigh-school adolescentsinthestateofPernambuco,Brazil,2006.
45
40
35
30
25
20
15
10
5
0
10.210.9
0 RBs 1 RBs
Risk behaviors (RBs)
2 RBs ≥3 RBs
9.7 31.3
29.9
37.4 34.8
39.2
24.4 21.1
19.0 32.1
%
All
Males
Females
Table2 Prevalenceofco-occurrenceofhealthriskbehaviorsaccordingtodemographic,socioeconomic,school-relatedand regionaldivisionvariablesinhigh-schooladolescentsfromPernambuco,2006.
Variables Co-occurrenceofhealthriskbehaviors(RBs)
0RBs 1RBs 2RBs ≥3RBs p-value
% n % n % n % n
Demographicfactors
Gender
Male 10.9 180 29.9 491 34.8 571 24.4 400 <0.083
Female 9.7 240 32.1 794 39.2 968 19.0 470
Age
14---16years 10.5 183 32.2 560 38.3 666 19.0 331 0.028
17---19years 9.9 237 30.6 730 36.8 876 22.7 540
Maternalschooling
≤8years 9.9 277 32.3 907 38.8 1,091 19.0 535 0.008
9---11years 11.2 92 28.6 234 33.5 274 26.7 219
≥12years 11.2 28 26.5 66 35.7 89 26.5 66
Ethnicity
Caucasian 8.8 91 33.8 350 35.4 366 22.0 227 0.732
Non-Caucasian 10.6 326 30.4 934 38.1 1172 20.9 644
Geographicregion
Metropolitan 12.0 207 32.0 551 35.3 609 20.7 356 <0.001
Forestarea 9.5 69 33.7 246 40.6 296 16.2 118
Semi-arid 8.6 144 29.5 493 38.1 637 23.8 397
Residencearea
Urban 10.1 328 30.8 994 36.6 1181 22.5 728 0.009
Rural 9.9 86 33.7 292 40.4 350 15.9 138
School-relatedfactors
Schoolshift
Daytime 10.6 252 31.5 749 36.6 870 21.3 507 0.522
Nighttime 9.7 168 31.1 541 38.4 669 20.8 363
Schoolsize
Small 10.6 39 27.7 102 39.4 145 22.3 82 0.085
Medium 11.0 117 35.6 378 35.2 374 18.2 193
Large 9.8 264 30.1 810 38.0 1023 22.1 596
Socioeconomicfactors
Employmentstatus
Unemployed 9.6 308 31.5 1017 37.8 1219 21.1 682 0.209
Employed 12.5 109 30.2 263 36.0 313 21.3 186
In the bivariate analysis, we observed that the pro-portionofadolescentssimultaneously exposedtothreeor more risk behaviors was statistically higher among older students (17---19 years),adolescents withhigher maternal education,studentslivingintheurbanareaandthosewho livedinthesemi-aridregionwhencomparedtotheirpeers (Table2).
Table3 showstheresults oftheordinallogistic regres-sionanalysisfortheco-occurrenceofhealthriskbehaviors accordingtodemographicandschool-relatedfactors.Inthe adjusted analysis, it wasobserved that age,occupational status, maternal education, geographic region and place of residence were statistically associated with higher co-occurrenceofhealthriskbehaviors.
Itwasverifiedthatolderadolescents(17---19years)had a17%higherchanceofsimultaneousexposuretomorethan
threehealthriskbehaviorswhencomparedtoyoungerones. Studentswhoreportedworkinghada14%lowerchanceof havingmore than threerisk behaviorswhen compared to thosewhodidnotwork.Ontheotherhand,adolescentswho reportedmotherswithintermediateeducation(9---11years) had a 21% higher chance of having co-occurrence of risk behaviors,comparedtothosewhoreportedlowermaternal education(≤8years).
Table3 Ordinallogisticregressionforco-occurrenceofhealthriskbehaviorsanddemographic,socioeconomic,school-related andregionaldivisionvariablesinhigh-schooladolescentsfromPernambuco,2006.
Variables Co-occurrenceofhealthriskbehaviors
CrudeOR 95%CI p AdjustedOR 95%CI p
Gender
Male 1 1
Female 0.90 0.80---1.00 0.060 0.91 0.81---1.03 0.140
Age
14---16years 1 1
17---19years 1.13 1.01---1.27 0.028 1.17 1.04---1.32 0.008
Maternalschooling
≤8years 1 0.004 1 0.009
9---11years 1.21 1.05---1.40 0.010 1.21 1.04---1.40 0.011
≥12years 1.26 0.99---1.60 0.058 1.21 0.95---1.55 0.121
Ethnicity
Caucasian 1 Excluded
Non-Caucasian 0.99 0.87---1.13 0.927
Geographicregion
Metropolitan 1 1
Forestarea 0.97 0.83---1.14 0.731 1.07 0.90---1.26 0.435
Semi-arid 1.27 1.13---1.44 <0.001 1.39 1.22---1.59 <0.001
Residencearea
Urban 1 1
Rural 0.83 0.73---0.95 0.008 0.78 0.68---0.91 0.001
Schoolshift
Daytime 1 Excluded
Nighttime 1.04 0.93---1.16 0.542
Schoolsize
Small 1 0.084 Excluded
Medium 0.76 0.61---0.94 0.013
Large 0.97 0.79---1.19 0.782
Employmentstatus
Unemployed 1 1
Employed 0.93 0.81---1.06 0.285 0.86 0.74---0.99 0.040
Discussion
The results of this study show that the prevalence of simultaneousexposuretohealthriskbehaviorsamong ado-lescentsfromthestateofPernambucowashigh,asobserved in similarstudies.8,10---12 Another important result wasthe identification of five significant factors associated to the higherco-occurrenceofthesebehaviors,namely:agerange, maternaleducation,geographicregion,workingstatus,and placeofresidence.
The results of thissurveyindicated that 58.5% of ado-lescentsweresimultaneouslyexposed totwoor morerisk behaviors, as observed in a study carried out in the city of João Pessoa, state of Paraiba.15 The importance of this finding lies in the fact that health problems can be caused by a set of aggregated risks behaviors, such as throatcancer,whichcanbeexplainedbythesimultaneous occurrence of two habits (smoking and alcohol consump-tion), as highlighted by the World Health Organization (WHO).24
Inthisstudy,simultaneousexposuretoahighernumberof healthrisk behaviorswashigheramongolderadolescents. As seen in theavailable studies, theprevalence of simul-taneous exposure to health risk behaviors increases with age.8,13,25 Thatcan be explained by thefact that adoles-cents acquire greater autonomy and social and economic independencewithage,26favoringaccesstoplacesthatsell alcoholicbeverages,cigarettesandotherdrugs.
Itwasalsoobservedthatadolescentswhoreported hav-ing a jobhad lower chancesof simultaneous exposure to ahighernumberof healthrisk behaviors, whencompared tothosewhodidnotwork.Inasociety whereyoung indi-vidualsfacegreatchallengestoenterthelabormarket,it ispossibletoassumethatyoungindividualswhoengagein somelaboractivityhavehigherself-esteem,autonomyand personal responsibility,characteristics that may favor the adoptionofhealthierbehaviors.
Adolescents who live in the semi-arid region of Pernambucoshoweda39%increaseinthechanceof simulta-neousexposuretoahighernumberofhealthriskbehaviors compared to their peers living in the metropolitan area. Comparativestudieswithanalysisofsimultaneousexposure tolifestylehabitsarescarce,makingthecomparisons impos-sible.However,Matsudo etal.28 carriedoutastudy inthe stateofSãoPaulo,observingthattheindividualswholived onthecoastweremoreactivethanthoselivinginthe coun-tryside.Thismayberelatedtothelowsupplyofleisureand physicalfacilitiesforphysicalactivitiesinthecountryside. Moreover,itmayberelatedtotheavailability,accessibility andqualityoffoodpreservationinthisregion,wherethere isanacknowledgedshortageofwaterresources, indispens-able for both the production and the processing of fresh food.
On theother hand, adolescentswholiveinruralareas hada22%decreaseinthechanceofsimultaneousexposure toahighernumberofhealthriskbehaviorswhencompared tothoselivinginurbanareas.Thiscanbeexplainedbythe specificcharacteristicsofthetypesofactivitiescarriedout in rural areas, which require greater energy expenditure tobeperformed (e.g. extensive andfamilyfarming, live-stock, vegetal extractivism, mineral extractivism, etc.),29 inadditiontogreater accesstofoodssuch ascereals and derivatives(beans,riceandcorn)andtubers(potatoes, cas-savaand others),whichareessentiallyproductsof family agriculture,aswellastheloweraccesstoready-mademeals andindustrializedmixes.30
Thelackofsimilarstudiesmakesitdifficulttocompare thefindingsofthepresentstudy.Whatwasfoundinthe liter-aturewaslimitedtostudiesthatevaluatedtheassociation of thesefactorswithisolated exposuretoone or another riskybehavior. Similarstudiesavailable13---17 usedvery dif-ferent methodological procedures, particularly regarding the type, quantity and definition of characterizing risk variables.
The generalization ofthe resultsof thisstudy must be made with caution, as only adolescents attending public schoolswereincluded.Onecanassumethattheresultsare differentinsamplesofadolescentsattendingprivateschools andamongthosewhoarenotenrolledintheformal educa-tionalsystem.Ontheotherhand,thedecisiontonotinclude privateschoolsinthesamplingplanningwasduetothefact thatmorethan80%ofadolescentsfromPernambucowere enrolledinpublicschools.
Itisnoteworthythattheprevalenceshowninthisarticle disclosesascenarioobservedsometimeagoand,therefore, theinterpretationoftheseparametersshouldbemade care-fully,associalanddemographicchangesthathaveoccurred intheBraziliannortheastregionduringthisperiodmayhave affectedtheseindicators.Ontheotherhand,itisnot plausi-bletoassumethattheassociationsthatwereidentifiedand
reportedin this study would be differentdue topossible changesintheprevalenceofsomefactor.
Despitethegoodreproducibilitylevelsof thetool,one cannotruleoutthepossibilityofinformationbias,as adoles-centstendtooverestimateor,atothertimes,underestimate theexposuretoriskbehaviors.
However,thefindingsofthissurveyaddimportant evi-dencetotheavailablebodyofknowledgeontheprevalence and factors associated with co-occurrence of health risk behaviorsinadolescents. Additionally, thestudy was per-formed with a relatively large sample, representative of high-school students from public schools in the state of Pernambuco. It is believed that the evidence shown in this study may help identify more vulnerable subgroups, thuscontributingtodecision-makingandappropriate inter-vention strategy planning. Moreover, it can lead to the developmentofotherinvestigations.
Consideringthesefindings,itcanbeconcludedthatthere isa large portionof adolescentsexposed tosimultaneous healthriskbehaviors.Itwasalsoverifiedthatolder adoles-cents,withmothersofintermediateeducationallevelsand livinginthesemi-aridregionhadhigherchanceof simulta-neousexposuretoahighernumberofhealthriskbehaviors, thusconfiguringhigher-risksubgroups,whereasadolescents whoworkedandthoselivinginruralareaswerelesslikely tohavesimultaneousexposuretoahighernumberofhealth riskbehaviors.
Funding
Study supported with financial assistance from the Con-selhoNacionaldeDesenvolvimentoCientíficoeTecnológico (process486023/2006-0),Coordenac¸ãodeAperfeic¸oamento de Pessoal de Nível Superior (PROCAD-NF 178/2010) and Fundac¸ãodeAmparo à Ciênciae TecnologiadoEstadode Pernambucobygrantingofscholarships.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
The authors thank Conselho Nacional de Desenvolvi-mento Científico e Tecnológico (process 486023/2006-0), Coordenac¸ãodeAperfeic¸oamentodePessoaldeNível Supe-rior and Fundac¸ão de Amparo à Ciência e Tecnologia do Estado de Pernambuco for their financial support, which madeitpossibletoperformthepresentstudy.
References
1.WorldHeartFederation.Urbanizationand cardiovascular dis-ease:raisingheart-healthychildrenintoday’scities.Geneva: WorldHeartFederation;2012.
2.EisenmannJC.Physicalactivityandcardiovasculardiseaserisk factorsinchildrenandadolescents:anoverview.CanJCardiol. 2004;20:295---301.
4.MikkiläV,RäsänenL, RaitakariOT,PietinenP,ViikariJ. Lon-gitudinalchangesindietfrom childhoodintoadulthoodwith respecttoriskofcardiovasculardiseases:theCardiovascular RiskinYoungFinnsStudy.EurJClinNutr.2004;58:1038---45. 5.TwiskJW,VanMechelenW,KemperHC,PostGB.Therelation
betweenlong-termexposuretolifestyleduringyouthandyoung adulthoodandriskfactorsforcardiovasculardiseaseatadult age.JAdolescHealth.1997;20:309---19.
6.Berenson GS. Childhood risk factors predict adultrisk asso-ciated withsubclinical cardiovascular disease. The Bogalusa HeartStudy.AmJCardiol.2002;90:3L---7L.
7.HardyLL,GrunseitA,KhambaliaA,BellC,WolfendenL,Milat AJ. Co-occurrence of obesogenic risk factors among adoles-cents.JAdolescHealth.2012;51:265---71.
8.FariasJúniorJC,NahasMV,BarrosMV,etal.Comportamentos deriscoàsaúdeemadolescentesnoSuldoBrasil:prevalênciae fatoresassociados.RevPanamSaludPublica.2009;25:344---52. 9.Plotnikoff RC, Karunamuni N, Spence JC, et al. Chronic
disease-related lifestyleriskfactors inasampleofCanadian adolescents.JAdolescHealth.2009;44:606---9.
10.OheneSA,IrelandM,BlumR.Theclusteringofriskbehaviors amongCaribbeanyouth.MaternChildHealthJ.2005;9:91---100. 11.FariasJúniorJC,LopesAS.Comportamentosderisco relaciona-dosàsaúdeemadolescentes.RevBrasCiencMov.2004;12:7---12. 12.FeltonGM,PateRR,ParsonsMA,etal.Healthriskbehaviorsof
ruralsixthgraders.ResNursHealth.1998;21:475---85. 13.Müller-RiemenschneiderF,NoconM,WillichSN.Prevalenceof
modifiablecardiovascularriskfactorsinGermanadolescents. EurJCardiovascPrevRehabil.2010;17:204---10.
14.KelishadiR,GholamhosseinS,TavasoliAA,etal.A prevalên-ciacumulativadefatoresderiscoparadoenc¸acardiovascular em adolescentes iranianos --- IHHP-HHPC. J Pediatr (Rio J). 2005;81:447---53.
15.Farias JúniorJC, MendesJK, BarbosaDB, Lopes AS. Fatores de risco cardiovascular em adolescentes: prevalência e associac¸ãocomfatoressociodemográficos.RevBrasEpidemiol. 2011;14:50---62.
16.RomanziniM,ReichertFF,LopesAS,PetroskiEL,FariasJúnior JC.Prevalênciadefatoresderiscocardiovascularem adoles-centes.CadSaudePublica.2008;24:2573---81.
17.Guedes DP, Guedes JE, Barbosa DS, Oliveira JA, Stanganelli LC.Fatoresde risco cardiovascularesem adolescentes: indi-cadores biológicos e comportamentais. Arq Bras Cardiol. 2006;86:439---50.
18.NahasMV,BarrosMV,GoldfineBD,etal.Physicalactivityand eating habits in public high schools from different regions in Brazil: the Saude na Boa project. Rev Bras Epidemiol. 2009;12:270---7.
19.XavierIC,HardmanCM,AndradeML,BarrosMV.Frequênciade consumodefrutas,hortalic¸aserefrigerantes:estudo compara-tivoentreadolescentesresidentesemáreaurbanaerural.Rev BrasEpidemiol.2014;17:371---80.
20.Tassitano RM, Barros MV, Tenório MC, et al. Enrollment in physical education is associated with health-related behav-ior among high school students. J Sch Health. 2010;80: 126---33.
21.TenórioMC, BarrosMV,TassitanoRM, BezerraJ,Tenório JM, Hallal PC. Atividadefísica e comportamento sedentário em adolescentesestudantesdoensinomédio.RevBrasEpidemiol. 2010;13:105---17.
22.Organizac¸ão Pan-Americana da Saúde Prevenc¸ãode doenc¸as crônicas:uminvestimentovital.Genebra:OMS;2005. 23.KatzmarzykPT,ChurchTS,CraigCL,BouchardC.Sittingtime
andmortalityfromallcauses,cardiovasculardisease,and can-cer.MedSciSportsExerc.2009;41:998---1005.
24.Organizac¸ãoMundialdaSaúdeReducingrisk,promotinghealthy life.Geneva:OMS;2002.
25.SilvaKS,LopesAS,VasquesDG,CostaFF,SilvaRC.Clusteringof riskfactorsforchronicnoncommunicablediseasesamong ado-lescents:prevalenceandassociatedfactors.RevPaulPediatr. 2012;30:338---45.
26.EisensteinE. Adolescência:definic¸ões, conceitos ecritérios. AdolescSaude.2005;2:6---7.
27.FariasJúniorJC,LopesAS,MotaJ,HallalPC.Práticade ativi-dadefísicaefatoresassociadosemadolescentesnoNordeste doBrasil.RevSaudePublica.2012;46:505---15.
28.Matsudo SM, Matsudo VR, Araújo T, et al. Nível de ativi-dade física da populac¸ão do Estado de São Paulo: análise de acordo com o gênero, idade, nível socioeconômico, distribuic¸ãogeográficaedeconhecimento.RevBrasCiencMov. 2002;10:41---50.
29.Bicalho PG, Hallal PC, Gazzinelli A, Knuth AG, Velásquez-MeléndezG. Atividadefísicaefatoresassociadosem adultos de área rural em Minas Gerais, Brasil. Rev Saude Publica. 2010;44:884---93.