rev bras ortop.2013;48(6):563–566
w w w . r b o . o r g . b r
Case
Report
Chondromyxoid
fibroma
of
the
distal
fibula
in
a
pediatric
patient:
a
case
report
夽
Antonio
Carlos
Canto
Tomazini
a,∗,
João
Paulo
Carniel
b,
Luiz
Antonio
Munhoz
da
Cunha
b,caOrtopediaeTraumatologia,HospitalUniversitárioCajuru,Curitiba,PR,Brazil bHospitaldeClínicas,UniversidadeFederaldoParaná,Curitiba,PR,Brazil cHospitalPequenoPríncipe,Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received5May2012 Accepted17October2012
Keywords:
Fibroma Neoplasms Pediatrics
a
b
s
t
r
a
c
t
Thiscaseshowsararetumor(chondromyxoidfibroma)indistalfibulainapediatricpatient whopresentedwithlocalpainandtumescence.Afinaldiagnosiswasmadeonlyafterthe secondoperation,whereinthepathologywascomparedwithCTimagingmethodanduse ofadjuvants.
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Fibroma
condromixoide
em
fíbula
distal
em
paciente
pediátrico:
relato
de
caso
Palavras-chave:
Fibroma Neoplasia Pediatria
r
e
s
u
m
o
Estecasoretrataum rarotumor(fibroma condromixoide)em fíbuladistalem paciente pediátrico,queseapresentavacomdoreedemalocal.Odiagnósticofinalsófoifeitoapósa segundaintervenc¸ãocirúrgica,emqueoanatomopatológicofoicomparadocomasimagens tomográficaseousodemétodosadjuvantes.
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevierEditora Ltda.Todososdireitosreservados.
Introduction
Primarybonetumorsthataffectthepediatricagegroupare infrequentconditions,butwhentheyoccur,theyaremostly benign lesions.1,2 Chondromyxoid fibroma (CMF) is a very
夽
WorkperformedatHospitalPequenoPríncipe,Curitiba,PR,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](A.C.C.Tomazini).
raretumorandisdefinedbytheWorldHealthOrganization as a “benign tumor characterized by lobulated areas with fusiform cells;withabundantintercellularmyxoidor chon-droidmaterial,separatedbyzonesofgreater concentration ofroundedorfusiformcells,withgiantmultinucleatedcells ofdifferent types”. Areas ofmyxomatous tissueoccur due
2255-4971/$–seefrontmatter©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
564
r e v b r a s o r t o p . 2 0 1 3;48(6):563–566tonecrosisofthechondroidtissue,andfibrousareasdueto repairofthedegeneratedareas.Thesetumorscanbe con-foundedwithchondrosarcoma,sincetheymaypresentcells withpleomorphism.3 Theyaccountforless than1%of
pri-marybonetumors.3JaffeandLichteinstein,in1948,werethe
firsttodescribethistypeoflesion,inaseriesofeightcases locatedinthelower limbs.All ofthe casespresentedmild painandapalpablemassatthesite,withoutanyhistoryof trauma.4–6
Thesetumorshavegreaterincidenceinchildrenatpuberty andduringadolescence,andtheirmainlocationisthe meta-physealregionofthelongbones,especiallyinthelowerlimbs. Theproximaltibiaisaffectedin50%ofthecases,followedby thefemur,metatarsusandcalcaneus.6,7 Clinicalcomplaints
aregenerallyminimalorevennonexistentbutwhenpresent, thepatientreportsmildpainintheregionaffected,whichhas aninsidiousprogressivecourse,andslightedemaandjoint irritationmaybepresented.8,9
Radiologically, a metaphyseal lytic lesion of eccentric nature,whichonrareoccasionsmaycrosstheepiphysealline, canbeobserved.5,6 Athinhaloofreactivebonebordersthe
externalpartofthelesion,whiletheinternalpartappearsto haveanirregularoutlinethatmaypresentslightsclerosis.6,8
Throughimagingexaminations,itcanbedifferentiatedfrom chondroma,fibrousdysplasiaandaneurysmaticbonecysts. Helicoidcomputedtomographyclearlyshowsthedetailsof thetumor, whichgenerally rangesfrom 1.5to8cm insize andmaycontainsmallcalcifications.9,10Itisveryimportant
toestablish its relationship withthe growth plate and the neighboringstructures.6 Thetreatment consists of
intrale-sionalresectionofthetumor,withfulgurationofitsinterior, andbonecementcanbeusedtofillthespaceleftbythe exci-sion.Alternatively,curettagecanbeperformed,followedby autologousorhomologousgrafting,whichavoidsinjuringthe growthplate.8,9Recurrenceisextremelyrareandtheseisno
needforchemotherapyorradiotherapyincasesofthisbenign pathologicalcondition.4,5
Case
report
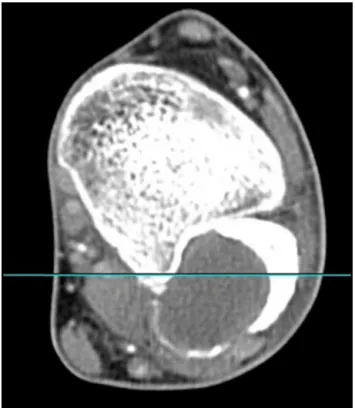
The patient was a 16-year-old male with a complaint of increased volume and pain in his left ankle over the last few months.He said that hehad notsuffered trauma. He showedslightabnormalityofgait,andtherewasno improve-mentinhisconditionthroughcontinuoususeofdiclofenac. Onphysicalexamination,hedidnotpresentanyrestrictions onmovement,butonlymildedema(+/4+)andpainondeep palpation of the lateral malleolus. Computed tomography showedalyticlesioninthefibularmalleolus,whichmeasured 2.9cm×2.6cmonthemajortransverseaxesand3cmonthe
verticalaxis.Hepresentedsmallfociofsolutionof continu-ityinthecorticalbone.Afteradministrationofcontrast,an annularareaofimpregnationwasobservedinsidethelesion, whichsuggestedtheexistenceofaninflammatory-infectious process.Themuscleandadiposetissuelayerswerepreserved (Figs.1and2).
The patient then underwent curettage of the lesion in the distal fibula, performed at the Pediatric Orthope-dics Service of Hospital Pequeno Príncipe (HPP, Curitiba,
Fig.1–Radiographoftheleftankle(March19,2009).
PR) in March 2009. Multiple fragments of firm granular pinkish–yellowishtissuewereremovedfromthefibula, mea-suring3cm×2.5cm×0.5cm.Fromtheanatomopathological
examination, it was concluded that this was an atypical
r e v b r a s o r t o p . 2 0 1 3;48(6):563–566
565
Fig.3–APandlateralradiographsoftheankle,oneyear afterthesurgery.
cartilaginousproliferation,withtherecommendationthatit shouldbeconsideredclinicallytobeanenchondroma.
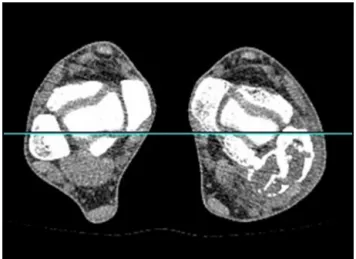
Atoutpatientreturnvisitsafter thesurgery, thepatient continued to present slight edema in the leg and pain on palpation of the malleolus. This worsened one year after the surgery. He complained of daily pain and a dis-crepancy of 10◦ less dorsiflexion of the foot, in relation to the other limb. After a new tomography examination (Figs.3and4),itwasdecidedtoperformanewsurgical inter-vention.
The patient underwent resection of the tumor, which measured8cm,and anautologousgraft fromthe iliacwas
Fig.4–Helicoidcomputedtomographyoftheankles bilaterally,oneyearafterthesurgery.
implanted,withfixationusingaKirschnerwireanda plaster-castsplint(Fig.5).Thereportfromtheanatomopathological examination showed that the tissue presented atypical cartilaginous proliferation and, after anatomoradiological correlation,thefinaldiagnosticconclusionwasthatthiswas chondromyxoidfibroma.
Atthesubsequentoutpatientfollow-ups,thepatientwas seentobeasymptomatic.TheKirschnerwirewasremoved60 daysaftertheoperationandweightbearingonthelimbwas progressivelyallowed.Therewasslightedemaandnolocal pain.Oneyearandtwomonthsafterthesecondsurgery,the patientnolongerreportedanypain;hiswalkinghad signifi-cantlyimprovedandthelimitationsonhismovementswere minimal(Fig.6).
566
r e v b r a s o r t o p . 2 0 1 3;48(6):563–566Fig.6–Radiographoftheankle,oneyearandtwomonthsafterthesecondsurgery.
Discussion
Chondromyxoidfibroma isa veryrare tumor and its form ofpresentationgenerallyconsistsofaclinical conditionof pain and edema,without any history of trauma. Itcan be demonstratedthroughsimpleradiographyonthelimb.The diagnosis ismade after anatomopathologicalanalysis, and thetreatmentmayvaryaccordingtotheregionaffected.Di Giorgioet al.10 reportedthat treatmentbymeans of
curet-tage,togetherwithphenolizationofthelesion,hadabetter prognosis.Likewise,Jesus-GarciaFilho4statedthattreatment
consistingofsimpleresectionofthelesionwasnotas effec-tive as treatment including associated adjuvant methods. Inourpatient, imagingmethodswere notusedinthefirst anatomopathological examinationfor correlating the diag-nosis, which may havedelayed the final diagnosis. In the secondsurgical approach,themultiprofessionalcorrelation usingimagingmethodstogetherwiththebiopsywasshown tobeeffective,asadvocatedinthestudybyGitelis.3
Bonetumorsduringchildhoodareentitiesthatare diffi-culttodiagnose, andtheseshouldbeborneinmindwhen facedwithachildwhopresentspainandincreasedvolume, orafracturethatisnotproportionatewiththeintensityofthe trauma.
Furthermore,whenapatientpresents asuspectedbone lesionandthisisbiopsied,itshouldbenotedthatforacorrect diagnosis,acorrelationshouldbemadebetweentheclinical conditionpresented,theradiologicalimagingandthe anato-mopathologicalreport,giventhat,asdescribed inthis case report,histologicalanalysisalonemayoftennotconfirmthe diagnosis. Theliterature suggests that when these lesions aretreatedbymeansofcurettage,thistechniqueshouldbe accompaniedbyanadjuvantmethod,inordertoeliminate theentiremassofneoplasticcells.
Conflicts
of
interest
Theauthorsdeclarethattherewerenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.CanaleT,BeatyJH.Campbell’soperativeorthopaedics.11th ed.Philadelphia:Mosby;2007.p.210–5.
2.MorrissyRT,WeinsteinSL,editors.Lovell&Winter’spediatric orthopaedics.6thed.Philadelphia:LippincottWilliams& Wilkins;2006.p.411–3.
3.GitelisS,WilkinsR,Conrad2ndEU.Benignbonetumors.Instr CourseLect.1996;45:425–46.
4.Jesus-GarciaFilhoR,KorukianM,IshiraraHI,MicenoFilho NM,FigueiredoMT,SeixasMT.Éacuretagemummétodo eficientenotratamentodostumoresósseos?RevBrasOrtop. 1993;28(11/12):813–6.
5.RalphLL.Chondromyxoidfibromaofbone.JBoneJointSurg Br.1962;44:7–24.
6.CaffeyJ.Onfibrousdefectsincorticalwallsofgrowing tubularbones:theirradiologicappearance,structure, prevalence,naturalcourse,anddiagnosticsignificance.Adv Pediatr.1955;7:13–51.
7.TakenagaRK,FrassicaFJ,McCarthyEF.Subperiosteal chondromyxoidfibroma:areportoftwocases.IowaOrthopJ. 2007;27:104–7.
8.RosalesOM,CaleroYG.Fibromacondromixoidediafisariode tíbia.RevCubanaOrtopTraumatol.2006;20(2):1–5.
9.LealFilhoMB,PereiraNetoA,PereiraLC,FrancoOS,SuzukiK, MelloPA,etal.Fibromacondromixoidedacolunatorácica: relatodecasoerevisãodaliteratura.ArqNeuropsiquiatr. 1995;53(4):837–40.