SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Morphologic
study
of
different
treatments
for
gastrocnemius
muscle
contusion
in
rats
夽
Ana
Carolina
Brandt
de
Macedo
a,∗,
Julye
Leiko
Ywazaki
b,
Rafael
Michel
de
Macedo
c,
Lucia
Noronha
d,
Anna
Raquel
Silveira
Gomes
aaUniversidadeFederaldoParaná,Curitiba,PR,Brazil
bAssociac¸ãodosPaiseAmigosdosExcepcionais(APAE),Pinhais,PR,Brazil cHospitalCardiológicoCostantini,Curitiba,PR,Brazil
dPontifíciaUniversidadeCatólicadoParaná,LaboratóriodePatologiaExperimental,Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received20July2015 Accepted7January2016 Availableonline15October2016
Keywords:
Musculoskeletalsystem Woundsandinjuries Musclestretchingexercises Ultrasonictherapy
a
b
s
t
r
a
c
t
Objective:Evaluatetheeffectsofultrasoundandstretchinginmorphologyafterratmuscle contusion.
Methods:MaleWistarrats(n=35,8–9weeks,271±14g)weredividedintofivegroups:control group(CG=3);lesiongroup(LG=8);lesion+ultrasoundgroup(LUG=8);lesion+stretching group(LSG=8);lesion+ultrasound+stretchinggroup(LUSG=8).Theultrasoundwasapplied inLUGandLUSGfromthethirdtotheseventhday,thedoseusedwas50%pulsed,0.5W/cm2,
5min.Fromthetenthuntilthetwentyfirstday,passivestretchingwasperformed,infour repetitionslasting30seachwith30sofrest.Initialandfinalbodyweight,muscleweightand length,numberandsarcomerelength,musclefibercross-sectionalarea,andpercentageof collagenwereevaluatedafter22days.
Results:Thefinalbodyweightwashigherthantheinitialinallgroups.Thenumberof sar-comereswasstatisticallyhigherinLSGthanLUGandhigherinLUSGthanLUSandCG;in sarcomerelengthwashigherinLUGwhencomparedwithLSG(p<0.05).Thecrosssectional areainLGwashigherthanLSG,andthepercentageofcollagenwashigherinLGwhen comparedwithLSGandCG;inLUGwhencomparedwithLSGandCG;andinLUSGwhen comparedwithCG.
Conclusion: Thepassivestretchingprotocolinducedsarcomerogenesisandantifibroticeffect overthemusclesubmittedtocontusion.Ultrasound,eveninassociationwithstretching, wasnotsufficienttopreventfibrosisintheinjuredmuscle.
©2016PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopedia eTraumatologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheCentroUniversitário(UniBrasil),PontifíciaUniversidadeCatólicadoParanáandUniversidadeFederaldoParaná, Curitiba,PR,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](A.C.Macedo).
http://dx.doi.org/10.1016/j.rboe.2016.10.001
Estudo
morfológico
entre
diferentes
tratamentos
da
contusão
muscular
de
gastrocnêmio
em
ratos
Palavras-chave:
Sistemamusculoesquelético Ferimentoselesões Exercíciosdealongamento muscular
Terapiaporultrassom
r
e
s
u
m
o
Objetivo: Avaliarosefeitosdoultrassomterapêuticoe/oualongamento,namorfologiaapós contusãomuscularemratos.
Métodos: RatosWistarmachos(n=35,8-9semanas,271±14g)foramdivididosemcinco grupos:GrupoControle(GC=3);GrupoLesão(GL=8);GrupoLesão+Ultrassom(GLUS=8); GrupoLesão+Alongamento(GLA=8);GrupoLesão+Ultrassom+Alongamento(GLUSA=8). Aaplicac¸ãodoultrassomnoGLUSeGLUSAfoifeitadoterceiroaosétimodia,pulsado50%, 0,5W/cm2,5min.Dodécimoaovigésimoprimeirodiafoifeitooalongamentopassivono
GLAeGLUSA,emquatrorepetic¸õesde30s,com30sdeintervalo,cadarepetic¸ão.Após22 dias,osratosforampesadoseosmúsculosdeambasaspatasforamretiradosparaanálise dopesoecomprimentomuscular,númeroecomprimentodossarcômeros,áreadesecc¸ão transversaeporcentagemdecolágeno.
Resultados: Opesocorporalfinalfoimaiordoqueoinicialemtodososgrupos.Onúmerode sarcômerosfoimaiornoGLAemrelac¸ãoaoGLUSenoGLUSAemrelac¸ãoaoGLUSeaoGC; ocomprimentodossarcômerosfoimaiornoGLUScomparadocomoGLA(p<0,05).Aárea desecc¸ãotransversanoGLfoimaiordoquenoGLAeaporcentagemdecolágenofoimaior noGLcomparadocomoGLAeoGC;noGLUScomoGLAeoGC;noGLUSAcomoGC.
Conclusão: Oprotocolodealongamentopassivoinduziuasarcomerogêneseeapresentou efeitoantifibróticoemmúsculossubmetidosacontusão.Oultrassom,independentemente daassociac¸ãocomoalongamento,nãofoisuficienteparaimpedirafibrosenosmúsculos lesados.
©2016PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade OrtopediaeTraumatologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Muscleinjuryaccountsfor60%ofsportsinjuries.1Despiteits
highprevalence,therearefewstudiesonitstreatment,which hindersthestandardizationofphysicaltherapy.2Amongthe
different forms of treatment, the most commonly recom-mended are:rest; cryotherapy/compression/elevation;early mobilization;laser;ultrasound;andexercisesofactive mobi-lization, passive stretching, and concentric and eccentric strengthening.2–5
Althoughitsbiologicaleffectsinacuteandchronic inflam-mationarenotwellunderstood,2,6–8 therapeuticultrasound
(TUS)hasbeenrecommended. Piedadeetal.7 assessedthe
effectsofpulsedapplicationonlaceratedgastrocnemius mus-cleofrats,andobservedasignificantincreaseinthenumber ofmyotubesintheregenerationzone14daysaftertreatment. However,despitesuchresults,theappropriatemodulationof the TUSparameters (frequency,intensity, mode,treatment time)isstillcontroversial.
In addition to treatment with electrothermal and pho-totherapeutic resources, exercise is recommended for the treatmentofmuscleinjury.Themostcommonlyprescribed exercise is muscle stretching.1,5 As with TUS, its
bene-fits on the injured fiber are unclear and it still has alow level of evidence. Nevertheless, Hwang et al.,9 in
experi-mental studies (rats), observed that the passive stretching doneduringtheinflammatory,proliferative,andregenerative phases reduced the muscle fibrosis area by 50%, increas-ingstrength and thenumber ofmyofiberswhen compared withthecontrolgroup,demonstratingabenefitformuscle
regeneration.Thebestresultsobtainedinthestudyoccurred when the stretching was initiated on the 14th day after injury.
Itisimportanttoemphasizethat bothTUSand muscle stretchingareindicatedforthetreatmentofmuscleinjury,2,5–9
butthereisstillnoconsensusonwhenandhowtoprescribe them.Moreover,itisunclearwhethertheassociationbetween thesetherapeuticmodalitiescan benefitthe muscle regen-erationmechanism.Thus,this studyaimedtoevaluatethe effectsofTUSand/orstretchingonmorphologyaftermuscle contusioninrats.
Methods
Sample
This was an experimental, prospective, randomized study. After approval by the Ethics Committee for Ani-mal Experimentation10 (EAEC) of the UFPR (Certificate No.
491/2010), 35 young Wistar rats were selected (8–9 weeks, 271±14g).Theanimalswere grouped infourper standard plastic cage, in an environment of controlled light (12h light/darkcycle)andtemperature,withfreeaccesstowater andpelletedfeed.
Inclusioncriteria
Sampledistribution
The animals included (n=35) were randomized into five groups: control group (CG=3); lesion group (LG=8); lesion+ultrasound group(LUG=8);lesion+stretchinggroup (LSG=8);lesion+ultrasound+stretchinggroup(LUSG=8).
Theanimalswererandomizedbydrawing.TheCGGroup wasplacedthreetimesandtheLUG,LSG,LG,andLUSGwere placedeighttimesinto aplasticbagfordrawing.Afterthe animalswereweighed,thedrawingwasconducted,andthe animalswereassignedintoeachgroupandseparatedintothe cages(Fig.1).
Protocolforpromotingmusclecontusion
The animals were anesthetized with ketamine (95mg/kg) andxylazine(12mg/kg)intraperitoneallyandkeptinaprone
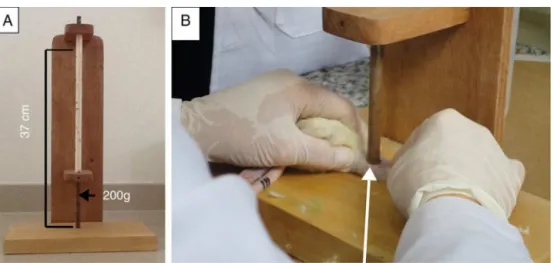
positionwith theright paw manuallyimmobilizedin knee extensionand90◦ dorsiflexionoftheanklejoint.Thelesion wasproducedintherightgastrocnemiusmuscle(RGM)using adeviceconsistingofawoodenplatformwithahollow alu-minumtube,graduatedat5cm,placedperpendicularlytothe platform,aspreviouslydescribedbyMinamotoetal.11(Fig.2).
Afterthelesion,theabsenceoftibialfracturewasassessedby meansofpalpationandhandling.1
Ultrasoundprotocol
For the application of TUS, a researcher immobilized the mousewhileanotherappliedthedevice.ToapplyTUS (cal-ibrated),theposteriorregionoftherightpawwasshavedand positionedinkneeextensionand90◦dorsiflexionoftheankle joint,andTUSwasappliedonthemedialbellyoftheRGM.Gel wasthecontactmedium.Theeffectiveradiationareawas1
Adult male Winstar rats selected for the study
(n=35)
Outcomes: Body weight Muscle weight Muscle length
Number and length of sarcomeres Cross-section area of muscle fiber
Percentage of collagen Sample randomized
into 5 groups
Control group (CG=3)
Lesion group (LG=8)
Day 0 – lesion Day 0 – lesion
Day 3-7 – ultrasound
Day 22 – euthanasia
Day 22 – euthanasia
Day 22 – euthanasia
Day 22 – euthanasia
Day 22 – euthanasia
Day 3-7 – ultrasound Day 0 – lesion
Day 10-21 – stretching
Day 10-21 – stretching
Day 0 – lesion Lesion +
ultrasound group (LUG=8)
Lesion + stretching group
(LSG=8)
Lesion + ultrasound + stretching group
(LUSG=8) Included animals (n=35) which
did not present fracture associated with the muscle lesion and weighed between
250-300 g
Fig.2–Apparatusforperformingmusclelesion.
A,apparatusforinductionofmusclelesion,whichindicatesthemassofthe200-gprojectile(arrow),whichisslidfroma heightof37cm;B,arrowindicatestheprojectileontheventralregionofthegastrocnemiusmuscleduringthelesion procedure.
cm2.TheapparatususedwastheSonopulseespecial(Ibramed), 1MHz, pulsedat100Hz,50%cycle, intensity7 of0.5W/cm2, andapplicationtimeof5min.TUSwasstarted72hafterthe lesion.
Protocolforstretchingthegastrocnemiusmuscle
Animalswereplacedinthesupinepositionwiththefrontlegs immobilizedbyaresearcher,sothatanotherresearchercould performpassivestretching.Tothisend,themaximumdorsal flexionoftheanklejointwasdonemanuallywiththeknee extended,asdescribedbyMattiello-Sverzutetal.12The
pro-tocolwasmaintainedfor30s13duringeachrepetition,with
anintervalof30s,fourrepetitions,14fivetimesaweek(from
MondaytoFriday).Stretchingwasinitiatedonthe10thday afterthelesion.
Chronologicalpresentationoftheinterventionsinthe groups
Table1showsthesequenceofinterventionsineach exper-imentalgroup.Aspulsedultrasoundhasanti-inflammatory effects(amongothers),itwasdecidedtousethisfeature dur-ingtheinflammatoryphaseofthelesion.Inturn,stretching wasstartedinthefibroblastproliferationphase.9
Euthanasiaandmusclecollection
Theanimalsofallgroupswereanesthetizedwithketamine (95mg/kg) and xylazine (12mg/kg) intraperitoneally for removalofthe right and leftgastrocnemiusmuscles using scissorsandtweezers.Subsequently,theanimalswere eutha-nizedwithananestheticoverdose(ketamineandxylazineon the22thdayofthestudy).
Eachmusclewasseparatelyweighedonananalytical bal-anceandtheirlengthwasmeasuredbycaliper.Themuscles werelongitudinallydividedinhalfusingascalpelblade.The lateralportionwasdiscardedandthemedialportionwas lon-gitudinallydivided inhalf.Halfofthesamples(lateral)had theirdistalendsfixedintherestingpositionwithultrafine needlesandweremaintainedfor3hinglutaraldehyde(2.5%), then nitric acid (30%)for 48h, and subsequently storedin glycerol(50%).Thelateralhalfwassubjectedtoroutine pro-ceduresforassessingthenumberofsarcomeresinseries,as describedbyWilliamsandGoldspink.15Themedialhalfofthe
RGM was fixedin10% formalin formorphologicalanalysis ofcross-sectional area ofmuscle fibers (CSAMF) and colla-gen percentage.Leftgastrocnemiusmuscle(LGM)wasused ascontrol.
Thenumberofsarcomereswasassessedtoverifywhether the combination of ultrasound and/or stretching could
Table1–Sequenceofinterventionsoftheexperiment.
Groupintervention LG LUG LSG LUSG CG
Contusion Day0 Day0 Day0 Day0
Ultrasound 3rdto7thday 3rdto7thday
Stretching 10thto21stday 10thto21stday
Euthanasia 22ndday 22ndday 22ndday 22ndday 22ndday
Fig.3–Photomicrographofanisolatedmusclefiber(100× objective).Arrow:eachstripinthearrowheadrepresentsa sarcomerethatwascountedalong100m.
potentiatetheincreaseinthenumberofsarcomeresinseries afterlesion. In turn,the cross sectional area and the per-centage of collagen were assessed to verify whether the combination ofultrasoundand/or stretching could prevent muscleatrophyandreducethepercentageofconnective tis-sue after muscle lesion.All of these mechanisms may be affectedaftermusclelesion.
Identifyingthenumberofsarcomeresinseries
For preparation of histological slides, five fibers were iso-lated(usingultrafinetipforceps)ofeachmuscle.Thefibers werephotographedunderalightmicroscope(100×objective, immersion).Oneachfiber,thenumberofsarcomeresinseries wasidentifiedin100m;threefieldsofdifferentdifferent
pho-tomicrographswere used along each muscle fiber, totaling 300m.
Aftercountingthenumber ofsarcomeresinthe 300m
area,thetotalnumberofsarcomereswasestimatedand cor-relatedwiththetotallengthofthemuscle,measured with calipersatthedayofeuthanasia(Fig.3).Thus,thefollowing equationwasused:numberofsarcomeresin300m,
multi-pliedbymusclelength,dividedby300.
Therefore,thetotalsarcomerenumberandlengthineach isolated fiber were estimated by correlation between the numberofidentifiedsarcomeresandthetotallengthofthe muscle.15–18
CSAMFandpercentageoftypeIandIIIcollagen
For analysis of the CSAMF,the material was stained with hematoxylinand eosin. Thephotomicrographs were made usingalightmicroscope at20× magnification. Tomeasure CSAMF, 100 muscle fibers were randomly selected in the central histologicalsection,using cross-sections of 8m.19
CSAMF was measured with the image program Pro Plus 4.0,and the unitofmeasurement adoptedwas the square micrometer(m2).Thefinalarithmeticmeanregardingthe
100measuredfiberswascalculated(Fig.4).
For analysis of collagen percentage, the material was stained withsirius red. Photomicrographs were made in a lightmicroscopeat20xmagnificationforhistologicalslides, usingcross-sectionsof8m.Theimageswereanalyzedusing
thesoftwareImageProPlus4.0.Aftercalibration,apreviously polarizedimagewaschosenbytheprogramtoestablisha pat-tern ofred and green,which was quantifiedinall images. Thisimagewasconsidered asa“mask”,which was super-imposeduponanyotherimagesforidentificationofcertain
Fig.4–Photomicrographofahistologicalcross-sectionof thegastrocnemiusmuscletomeasureCSAMFusingthe
ImageProPlus4.0software.Outlineinwhite:outlineto measurethecross-sectionalareaofmusclefiber(CSAMF).
colors.Afterthe“mask”wasoverlaidoneachimage,the pro-gramcalculatedthepercentageofredandgreencolors,which correspondtothemature(typeI)andimmature(typeIII) col-lagenoftheendomysiumandperimysial,respectively.20The
resultswereexpressedaspercentageofmaturecollagen(I, red)andimmaturecollagen(III,green),andthesumofbothis equalto100%(Fig.5).
Analysisofresults
Toassessnormalityandhomoscedasticity,theShapiro–Wilk and Levene tests were performed, respectively. Inter- and intra-group comparisons were made by one-way ANOVA
posthocTukey unequalHSDforparametric values;for non-parametricvalues,theKruskal–Wallistestwasused.Values were considered significant when p≤0.05.Statistica 7 was usedforthestatisticalanalyses.
Results
Bodyweight
Asignificantincreasewasobservedbetweentheinitialand finalweightinallgroups.Regardingabsoluteweight,thefinal bodyweightintheLGwashigherthanintheLUSG;thevaluein theLUGwashigherthanintheLUSG;andthevalueintheCG washigherthanthatintheLSGandintheLUSG.Inrelative difference,asignificantincreasewasnotedbetweenLGand LSG;LGandLUSG;LUGandLSG;andLUGandLUSG(Table2).
Weightandlengthofthegastrocnemiusmuscle
Therewasnostatisticallysignificantdifferenceinthe com-parisonofweightandmusclelengthbetweentheRGM and theLGMandamongthegroups(Fig.6AandB).
Estimatednumberofsarcomeresinseries(ENSS)
Fig.5–Photomicrographsofbladeswithtransversehistologicalsectionsofthegastrocnemiusmusclestainedwithsirius red.
A,imageshowsthecrosssectionofthegastrocnemiusmusclestainedwithsiriusred;whitearrowshowstheareastained inred,identifyingtypeIcollagen(mature)andtheasterisktheareaingreencorrespondstotypeIIIcollagen(immature);B, imageshowsaphotomicrographofthecross-sectionofthegastrocnemiusmuscleoverlappedbythe“mask”.Thenumbers representthevaluesoftheareasmarkedinredandgreencolors,identifiedbythesoftware.
intergroupcomparison,asignificantincreaseoftheENSSin theRGMwasobservedbetweentheLSGandLUG;LUSGand LUG;andLUSGandCG(Fig.6C).
SarcomerelengthandCSAMF
Inthecomparisonoftheright andleft sidesintheLSG, it wasfoundthatsarcomerelengthwasgreaterintheLGMthan intheRGM.Inthecomparisonbetweengroups,anincreased lengthofthesarcomeresoftheRGMwasobservedbetween LUGandLSG(Fig.6D).CSAMFoftheRGMwasgreaterinthe LGwhencomparedwithLSG(Fig.7A).
AnalysisoftypeI(mature)andIII(immature)collagens
Therewasnostatisticallysignificantdifferenceinthe com-parisonbetweenRGMandLGMineachexperimentalgroup (p>0.05). In the intergroup analysis of RGM, a significant increase(p<0.05)wasfoundinthepercentagesofmature col-lagen(typeI)inLG andLSG(40±12%vs.24±14%);LGand CG(40±12%vs.21±9%);LUGandLSG(37±10%vs.24±14%);
LUGandCG(38±10%vs.21%);andLUSGandCG(36±12%vs.
21±9%)(Fig.7B).
Discussion
Passivemanualstretchingincreasedthenumberof sarcom-eresinseriesandpreventedtheincreaseintypeIcollagenin injuredmuscles.However,theultrasoundprotocol,regardless ofassociationwithstretching,showednoantifibroticeffectin thesemuscles.
Inrelationtobodyweight,allgroupsshowedanincrease whencomparingtheinitialwiththefinalweight.The abso-lutefinalbodyweightwashigherintheCGthanintheLSG and inthe LUSG;theLG andLUG had greaterweight than theLUSG.Therefore,thegroupsthatunderwentthehighest amountofstimulation(contusion,ultrasound,andstretching) mayhavepresentedanegativeinterferenceinabsolutebody weightgain,sincetheCGhadthehighestfinalbodyweight.
Therewerenosignificantdifferencesinmuscleweightand length,perhapsduetotheshortinterventionperiodandthe
Table2–Effectsofultrasoundand/orstretchingonthebodyweightofmice.
Groups Initialweight(g) Finalweight(g) Relativedifference(%) pANOVA
LG 267± 11 350± 18a,b 31±7e 0.02
LUG 266±10 352±19a,c 32±10f 0.01
LSG 271±11 323±18a 19±8 0.00
LUSG 270±14 318±16a 17±3 0.00
CG 299±16 383±24a,d 28±6 0.00
LG,lesiongroup;LUG,lesion+ultrasoundgroup;LSG,lesion+stretchinggroup;LUSG,lesion+ultrasound+stretchinggroup;CG,controlgroup.
a Comparedwiththeinitialbodyweight. b ComparedwithLUSG(p=0.02). c ComparedwithLUSG(p=0.01).
dComparedwithLSG(p=0.00)andLUSG(0.001). e ComparedwithLSG(p=0.00)andLUSG. f (p=0.000)comparedwithLSGandLUSG.
0 0.5 1 1.5 2 2.5
CG LUSG LSG LUG LG
Muscle weight (g)
0 5 10 15 20 25 30
CG LUSG LSG LUG LG
Muscle length (mm)
0 2000 4000 6000 8000 10 000 12 000
CG LUSG LSG LUG
a Compared with the right gastrocnemius muscle of the LUG (P=.001). b
Compared with the right gastrocnemius muscle of the CG (P=.04).
c Compared with the left gastrocnemius muscle (P=.001).
d Compared with the right gastrocnemius muscle of the LSG (P=.001). e
Compared with the left gastrocnemius muscle of the LSG (P=.001). Mean ± standard deviation.
LG
ENSS
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5
CG LUSG LSG LUG LG
Length of the sarcomeres (
µ
m)
Right Left B
a a, b, c
a
d
C
D
A
B
Fig.6–Effectsofultrasoundand/orstretchinginweightandmusclelength,number,andlengthofsarcomeres.A,muscle weight;B,musclelength;C,thenumberofsarcomeresinseries;D,lengthofthesarcomeres.
ENSS,estimateofthenumberofsarcomeresinseries;LG,lesiongroup;LUG,lesion+ultrasoundgroup;LSG, lesion+stretchinggroup;LUSG,lesion+ultrasound+stretchinggroup;CG,controlgroup.
volumeofthe stretchingprotocol,that is,onlytwoweeks, fortwominuteseachsession.Coutinhoetal.19observedan
increasemusclelengthafter40minstretchingforthreeweeks. Therefore,theinterventionperiodandthevolumeof stretch-ingcontributetolongitudinalmusclegrowth.However,the measurementofthecross-sectionalareaofmusclefibersand thenumberofsarcomeresinseriescountarethemost accu-ratemethodsforassessingmuscletrophisminparallelandin series,respectively.21
Regarding the number of sarcomeres in series, the LSG presented a higher number, demonstrating the effect of stretchingonthesarcomerogenesisofinjuredmuscles.This differencemayalsobeduetothevolumeofstimulus,asthe LUGreceivedonlyfiveTUSapplicationsandtheLSGreceived ten stretching sessions.19 The combination of TUS with
stretching(LUSG)contributed totheincreaseinsarcomeres inserieswhencomparedwiththeLUG,demonstratingonce
againthestretching-stimulatedsarcomerogenesis,whichwas alsocrucialtothegrowthofsarcomeresininjuredmuscles. Furthermore,thisoutcomewasconfirmedthroughthe obser-vationthatthenumberofsarcomeresinseriesintheLUSG washigherthan intheCG.Thus,thisisthefirst confirma-tionofanincreaseinthenumberofsarcomeresinseriesin previously injured muscles. Thissuggests that the adapta-tionresultingfromtheassociationofTUSwithstretchingwas notonlyachangeinthepassivetensionofthelengthofthe muscle-tendonunit,beingsufficienttoinducemorphological adaptationofthelongitudinalmuscle.22
IntheLUG,thelengthofthesarcomeresintheRGMwas lowerthanintheLGM;comparingRGMs,thelengthof sarcom-ereswaslowerintheLUGthanintheLUSG.Theseoutcomes confirm the sarcomerogenesis observed in the LSG, since, accordingtoKoh,23skeletalmusclecanincreaseordecrease
0 2000 4000 6000 8000 10 000 12 000 14 000 16 000 18 000
A
B
Cross-sectional area (
µ
m²
)
LUG LG a
LSG LUSG CG
Right Left
0 10 20 30 40 50 60 70 80 90 100
LG
Percentage of the area of collagen
a
LUG b
LUSG LSG
c
CG
% Red D % Red E % Green D % Green E
a Compared with the right gastrocnemius muscle of the LUG (P=.01). b Compared with the LSG (p =.00) and CG (P=.00).
c Compared with the LSG (p = 0,00) and CG (P=.00).
Mean ± standard deviation
Fig.7–Ultrasoundand/orstretchingeffectsonCSAMF(A)andonthepercentageoftheareaoftypeIcollagen(mature,red) andtypeIIIcollagen(immature,green)(B).
R,right;L,left;LG,lesiongroup;LUG,lesion+ultrasoundgroup;LSG,lesion+stretchinggroup;LUSG,
lesion+ultrasound+stretchinggroup;CG,controlgroup;RedR(darkgraycolumn),typeIcollagenoftheRgastrocnemius; RedL(graycolumn),typeIcollagenoftheLgastrocnemius;GreenR(whitecolumn),typeIIIcollagenoftheR
gastrocnemius;GreenL(blackcolumn),typeIIIcollagenoftheLgastrocnemius.
sarcomereinwhichmaximummusclestrengthwillbe pro-ducedduringcontraction.Thus,thismechanismmighthave occurredintheintragroupLSGandinthecomparisonwith theLUG,since,asincreasednumbersofsarcomeresinseries wereobservedintheLSG,therewasadecreaseofthe sarcom-erelengthinthisgroup;thereversepatternwasidentifiedin theLUG.
Regarding CSAMF, it was observed that this value was higher in the LG than in the LSG; however, no difference wasobservedwhencomparingwiththeCG.Thebodyweight ofthe LGincreasedby31%,vs. 19%inthe LSG,whichmay haveinfluencedtheCSAMF,despitethefactthatnoincrease inmuscleweightwasobserved.Inthepresentstudy, ultra-soundandstretchingdidnotinfluenceCSAMF.Marketetal.6
assessedtheeffectsofTUSandlow-intensitywalking exer-cisefor 20min on the treadmill (speed 14m/min)for four days,initiated24haftermechanicallesionofthe gastrocne-mius,andalsodidnotobserveanincreaseinCSAMF.Coutinho etal.19foundthat40-minstretchingincreasedCSAMFinthe
immobilizedandstretchedgroupwhencomparedwiththe groupthatwas onlyimmobilized; thoseauthors concluded thatstretchingcanpreventmuscleatrophy,andits applica-tionisrelevantinimmobilizedmuscles.AstheLGpresenteda higherCSAMFthantheLSG,stretchingmayhaveinterferedin reducingedemaandregeneratingthesarcolemma,butitwas notsufficienttostimulateradial(transverse)musclegrowth, asreported inother studies.24,25 However,tofurther
eluci-datethemechanismsinvolvedinchangesinmuscletrophism, studies analyzingthe muscle ultrastructureand regulatory genesaresuggested.
Theinjuredmusclesandthosethatdidnotundergo inter-vention(ultrasoundand/orstretching)showedanincreased
percentageoftypeIcollagen,demonstratingthefibroticeffect ofthelesion.Thiseffectwasalsoobservedwhenultrasound wasappliedinisolationandinassociationwithstretching. Conversely,whenstretchingwasperformedalone,the prolif-erationofcollagenwaslowerthanthatobservedinmuscles thatunderwentTUSalone.Therefore,itcanbeconcludedthat stretchingshowedanantifibroticeffectwhencomparedwith isolatedorcombinedultrasound.
Williams et al.26 stated that dailystretching ofmuscles
shortenedduetoimmobilizationpreventsthedepositionof connectivetissueinthemuscletissue.ThestudybyHwang etal.9 corroboratedtheseresults.Theyassessedtheeffects
ofstretchingoninjuredmusclesandobserveditsantifibrotic effect. These authors indicated that stretching should be startedonthe14thdayafterlesion.However,inthepresent study stretching wasinitiatedonthe 10thday; despitethe earlyinitiation,thefibrinolyticeffectwasstillobserved. Jarvi-nenetal.27havesuggestedthattheincreaseintramuscular
connectivetissuecontributestofunctionaldeficits,producing tensilestrength,compliance,andmusclestiffness.Stretching programsmaycontributetoincreasemuscleextensibility,due tothereorganizationofintramuscularconnectivetissue.28
The LUG had a higher percentage of mature collagen in relation to the LSG and the CG. The increased density ofconnective tissue,associatedwith adecreased numbers ofsarcomeres, whichwas foundin LUG relativetoLSG, is characteristic of shortened skeletal muscle under fibrosis process.9,19,21,26Thisdemonstratesthatultrasoundusedalone
foronlyfivedayshasnofibrinolyticeffect.Rantanenetal.29
lesion.Theauthors foundanincreasedproductionof fibro-blastsafter musclecontusion inrats from the groupsthat hadundergoneatleastfivesessionsofpulsedTUS.Piedade etal.,7starteddailyapplicationsof1MHzpulsedTUSat50%,
intensityof0.57W/cm2,for5min,throughthesliding tech-nique,andobservedtheearlyonsetoftypeIcollagenfibers fourdaysaftergastrocnemiusmusclelesioninrats;abetter structuralarrangementandbetteralignmentofmyotubesin formationwasobservedinthegrouptreatedwithTUS.These authorssuggestedthatTUScanstimulateearlyaggregationof thistypeofcollagen.
AlthoughnoincreaseinthepercentageoftypeIcollagen (mature)wasobservedinthepresentstudy,theauthorsdid notassessthearrangement,thatis,theorientationofthe col-lagenfibers.Thus,itisnotpossibletopredictwhetherthis increaseintypeIcollagenmaygeneratefunctionaldeficits. Therefore,futurestudiesshouldusepolarizingmicroscopyfor analysisofbirefringenceofintramuscularconnectivetissue28
andrangeofmotion.
Theoutcomesofthisstudyindicateimportantclinical per-spectives,demonstrating thatapassive stretching protocol performedtendaysaftermusclelesioninduced sarcomeroge-nesisandpresentedanantifibroticeffect,indicatingapossible improvementofskeletalmuscleextensibility.Thus, respec-ting the limitations regarding direct extrapolations of the presentresultshumans,itcanbehypothesizedthat stretch-ingexercisescouldbeprescribedforthetreatmentofmuscles injuredbycontusion.
Study
limitations
Thisstudywaslimitedbytheuseofananimalmodel,which producesalowerlevelofscientificevidence.Therefore, ran-domized controlled clinical trials should be performed to assessthe effectsofultrasound,whether ornotassociated withstretching,ininjured skeletal muscleofhumans.The authorsrecommendtheuseofelectronmicroscopytoassess sarcomere length in future studies. Furthermore, analyses withmolecularbiologytechniquesshouldbeusedto investi-gatethegenesinvolvedintheprocessesofrepairandtropism ofskeletalmuscle,especiallyresultingfromtheapplication ofthetwotherapeuticmodalities,ultrasoundandstretching. Biomechanicalassaysforanalysisofmuscle-tendonunit ten-sionarealsoimportanttoelucidatetheviscoelasticproperties inresponsetoultrasoundand/orstretching.
Conclusion
Thepassivestretchingprotocolinducedsarcomerogenesisin injuredmuscles.Furthermore,stretchingalonehadan antifi-broticeffect,whileultrasound,regardlessofassociationthe stretching,wasnotsufficienttopreventtheincreaseof colla-genIininjuredmuscles.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
The authors would like to thankthe FederalUniversity of Paraná;theNationalCouncilforScientificandTechnological Development(CNPq, ProcessNo.474303/2011-0andProcess No. 308696/2012-3); the Pontifícia Universidade Católica do Paraná(PUC/PR);andUnibrasil.
r
e
f
e
r
e
n
c
e
s
1.SmithC,KrugerMJ,SmithRM,MyburghKH.The inflammatoryresponsetoskeletalmuscleinjury: illuminatingcomplexities.SportsMed.2008;38(11):947–69.
2.JärvinenTA,JärvinenTL,KääriäinenM,KalimoH,JärvinenM. Muscleinjuries:biologyandtreatment.AmJSportsMed. 2005;33(5):745–64.
3.OliveiraNM,ParizzottoNA,SalviniTF.GaAs(904-nm)laser radiationdoesnotaffectmuscleregenerationinmouse skeletalmuscle.LasersSurgMed.1999;25(1):13–21.
4.MasonD,DickensV,VailA.Rehabilitationforhamstring injuries.ScandJMedSciSports.2007;17:191–2.
5.ReurinkG,GoudswaardGJ,TolJL,VerhaarJA,WeirA,Moen MH.Therapeuticinterventionsforacutehamstringinjuries:a systematicreview.BrJSportsMed.2012;46(2):103–9.
6.MarkertCD,MerrickMA,KirbyTE,DevorST.Nonthermal ultrasoundandexerciseinskeletalmuscleregeneration.Arch PhysMedRehabil.2005;86(7):1304–10.
7.PiedadeMC,GalhardoMS,BattlehnerCN,FerreiraMA,Caldini EG,deToledoOM.Effectofultrasoundtherapyontherepair ofgastrocnemiusmuscleinjuryinrats.Ultrasonics. 2008;48(5):403–11.
8.WilkinLD,MerrickMA,KirbyTE,DevorST.Influenceof therapeuticultrasoundonskeletalmuscleregeneration followingbluntcontusion.IntJSportsMed.2004;25(1):73–7.
9.HwangJH,RaYJ,LeeKM,LeeJY,GhilSH.Therapeuticeffectof passivemobilizationexerciseonimprovementofmuscle regenerationandpreventionoffibrosisafterlacerationinjury ofrat.ArchPhysMedRehabil.2006;87(1):20–6.
10.NationalResearchCouncil.Guideforthecareanduseof laboratoryanimals.Washington,DC,USA:NationalAcademy Press;1996.
11.MinamotoVB,BunhoSR,SalviniTF.Regeneratedratskeletal muscleafterperiodiccontusions.BrazJMedBiolRes. 2001;34(11):1447–52.
12.Mattiello-SverzutAC,CarvalhoLC,CornachioneA,
NagashimaM,NederL,ShimanoAC.Morphologicaleffectsof electricalstimulationandintermittentmusclestretchafter immobilizationinsoleusmuscle.HistolHistopathol. 2006;21(9):957–64.
13.BertoliniGRF,BarbieriCH,MazzerN.Análiselongitudinalde músculossóleosderatossubmetidosaalongamentopassivo comusopréviodeultrassom.RevBrasMedEsporte. 2009;15(2):115–8.
14.TaylorDC,DaltonJDJr,SeaberAV,GarrettWEJr.Viscoelastic propertiesofmuscle-tendonunits.Thebiomechanicaleffects ofstretching.AmJSportsMed.1990;18(3):300–9.
15.WilliamsPE,GoldspinkG.Longitudinalgrowthofstriated musclefibres.JCellSci.1971;9(3):751–67.
16.MatanoT,TamaiK,KurokawaT.Adaptationofskeletal muscleinlimblengthening:alightdiffractionstudyonthe sarcomerelengthinsitu.JOrthopRes.1994;12(2):193–6.
18.TardieuC,TabaryJC,TabaryC,HuetdelaTourE.Comparison ofthesarcomerenumberadaptationinyoungandadult animals.Influenceoftendonadaptation.JPhysiol(Paris). 1977;73(8):1045–55.
19.CoutinhoEL,GomesAR,Franc¸aCN,OishiJ,SalviniTF.Effect ofpassivestretchingontheimmobilizedsoleusmusclefiber morphology.BrazJMedBiolRes.2004;37(12):1853–61.
20.Biondo-SimõesML,ZimmermannE,DaherTS,BorsatoKS, deNoronhaL.Effectsofhormonalreplacementtherapyon colonanastomosishealinginrats.ActaCirBras.
2005;20(3):237–42.
21.GomesARS,CoutinhoEL,Franc¸aCN,PolonioJ,SalviniTF. Effectofonestretchaweekappliedtotheimmobilizedsoleus muscleonratmusclefibermorphology.BiolRes.
2004;37:1473–80.
22.HoangPD,HerbertRD,ToddG,GormanRB,GandeviaSC. Passivemechanicalpropertiesofhumangastrocnemius muscletendonunits,musclefascicles,andtendonsinvivo.J ExpBiol.2007;210Pt23:4159–68.
23.KohTJ.Doadaptationsinserialsarcomerenumberoccur withstrengthtraining.HumMovSci.1995;14:61–77.
24.GoldspinkDF,CoxVM,SmithSK,EavesLA,OsbaldestonNJ, LeeDM,etal.Musclegrowthinresponsetomechanical stimuli.AmJPhysiol.1995;2682(Pt1):E288–97.
25.GoldspinkG.Changesinmusclemassandphenotypeandthe expressionofautocrineandsystemicgrowthfactorsby muscleinresponsetostretchandoverload.JAnat.1999;194 Pt3:323–34.
26.WilliamsPE.Useofintermittentstretchinthepreventionof serialsarcomerelossinimmobilisedmuscle.AnnRheumDis. 1990;49(5):316–7.
27.JärvinenTA,JärvinenTL,KääriäinenM,AärimaaV,Vaittinen S,KalimoH,etal.Muscleinjuries:optimisingrecovery.Best PractResClinRheumatol.2007;21(2):317–31.
28.CoutinhoEL,DeLucaC,SalviniTF,VidalBC.Boutsofpassive stretchingafterimmobilizationoftheratsoleusmuscle increasecollagenmacromolecularorganizationandmuscle fiberarea.ConnectTissueRes.2006;47(5):278–86.