REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
A
comparative
study
between
propofol
and
etomidate
in
patients
under
general
anesthesia
Supriya
Aggarwal,
Vipin
Kumar
Goyal
∗,
Shashi
Kala
Chaturvedi,
Vijay
Mathur,
Birbal
Baj,
Alok
Kumar
DepartmentofAnesthesiaandCriticalcare,MahatmaGandhiMedicalCollegeandHospital,Jaipur,Rajasthan,India
Received12September2014;accepted28October2014 Availableonline12May2015
KEYWORDS Propofol; Inductionof anesthesia; Myoclonus; Hemodynamic stability; Meanarterial pressure
Abstract
Backgroundandobjectives: Induction ofanesthesia isacritical partofanesthesiapractice. Suddenhypotension,arrhythmias,andcardiovascularcollapsearethreateningcomplications followinginjectionofinductionagentinhemodynamicallyunstablepatients.Itisdesirableto useasafeagentwithfeweradverseeffectsforthispurpose.Presentprospectiverandomized study isdesignedtocomparepropofolandetomidatefor theireffectonhemodynamicsand variousadverseeffectsonpatientsingeneralanesthesia.
Methods:HundredASAIandIIpatientsofagegroup18---60yearsscheduledforelectivesurgical procedureundergeneralanesthesiawererandomlydividedintotwogroupsof50each receiv-ingpropofol(2mg/kg)andetomidate(0.3mg/kg)asaninductionagent.Vitalparametersat induction,laryngoscopyandthereafterrecordedforcomparison.Adverseeffectviz.painon injection,apneaandmyoclonuswerecarefullywatched.
Results:Demographic variableswere comparableinboth thegroups.Patients inetomidate groupshowedlittlechangeinmeanarterialpressure(MAP)andheartrate(HR)comparedto propofol (p>0.05) frombaselinevalue. Painoninjectionwas moreinpropofolgroup while myoclonusactivitywashigherinetomidategroup.
Conclusions: Thisstudyconcludesthatetomidateisabetteragentforinductionthanpropofol inviewofhemodynamicstabilityandlesspainoninjection.
© 2015SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
PALAVRAS-CHAVE Propofol;
Induc¸ãodaanestesia; Mioclonia;
Estudocomparativoentrepropofoleetomidatoempacientessobanestesiageral
Resumo
Justificativaeobjetivos: Ainduc¸ãodaanestesiaéumapartecríticadapráticadeanestesia. Hipotensão súbita,arritmiasecolapsocardiovascularsãocomplicac¸õesameac¸adorasapósa
∗Correspondingauthor.
E-mail:[email protected](V.K.Goyal).
http://dx.doi.org/10.1016/j.bjane.2014.10.005
Estabilidade hemodinâmica; Pressãoarterial média
injec¸ãodeagentedeinduc¸ãoem pacienteshemodinamicamenteinstáveis.Éaconselhávelo usodeumagentesegurocommenosefeitosadversosparaessepropósito.Opresenteestudo prospectivo, randômico teve como objetivo comparar propofol e etomidatoquanto a seus efeitossobreahemodinâmicaeaosváriosefeitosadversosempacientessobanestesiageral.
Métodos: Cem pacientes ASA I e II, idades entre 18-60 anos, programados para procedi-mento cirúrgico eletivo sobanestesia geral foramdivididos aleatoriamente em dois grupos de 50 cadapara receber propofol (2mg/kg) e etomidato (0,3mg/kg) como um agente de induc¸ão.Osparâmetrosvitais nainduc¸ão,laringoscopiae posteriormenteforamregistrados paracomparac¸ão.Efeitosadversoscomodoràinjec¸ão,apneiaemiocloniaforam cuidadosa-mentemonitorados.
Resultados: Asvariáveisdemográficasforamcomparáveisemambososgrupos.Ospacientesdo grupoetomidatoapresentarampoucaalterac¸ãodapressãoarterialmédia(PAM)edafrequência cardíaca(FC)emcomparac¸ãocomogrupopropofol(p<0,05)apartirdovalorbasal.Houve mais doràinjec¸ão nogrupo propofol,enquanto houvemais atividade mioclônicano grupo etomidato.
Conclusões:Esteestudoconcluiqueetomidatoéumagentemelhorparaainduc¸ãoquepropofol emrelac¸ãoàestabilidadehemodinâmicaemenosdoràinjec¸ão.
©2015SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Inductionagents aredrugs that,whengiven intravenously inanappropriatedose,causearapidlossofconsciousness. Inductionagentsareusedtoinduceanesthesiapriortoother drugsbeinggiventomaintainanesthesia,asthesoledrugfor shortprocedures,tomaintainanesthesiaforlonger proce-duresbyintravenousinfusion,toprovideconscioussedation duringproceduresundergoinginlocalanesthesiaand inten-sivecareunit.
Propofol, 2,6-diisopropylphenol is most popular induc-tionagent with its favourble characteristics of rapid and smoothinductionandrecovery,decreaseincidenceof nau-seaandvomiting,etc.1,2Whileonothersidedecreaseblood pressure,dosedependentdepressionofventilation,painon injectionarethemajordrawbacks.3---5
Etomidate, carboxylated imidazole is characterized by hemodynamicstability,minimalrespiratorydepressionand cerebralprotectiveeffects.Itslackofeffectonsympathetic nervoussystem,baroreceptorreflexregulatorysystemand itseffectofincreasedcoronaryperfusionevenonpatients withmoderate cardiac dysfunctionmakes it an induction agentofchoiceincardiacdiseasepatients.6---9However,the adverseeffectssuchaspainoninjection,thrombophlebitis andmyoclonusaresomeundesirableadverseeffects.10,11
Thisstudyisanattempttoevaluatetheeffectsof propo-folandetomidatebycomparingcertainparameterssuchas change in blood pressure and heart rate during induction andintubationasaprimaryoutcomeandpainaninjection, myoclonicmovements,Post-operativenauseaandvomiting as a secondary outcome; so that we can choose a safer inductionagent.
Methods
Thisprospectiverandomizeddoubleblindstudyisconducted on 100 patients of American Society of Anaesthesiologist
(ASA)gradeIandIIbetween18and60yearsofageofeither sex,scheduledforelectivesurgicalprocedureundergeneral anesthesiawithendotrachealintubation.
After approval from institutional ethical committee, written informed consent was obtained from all the patients. The total 100 patients were randomly assigned into2groupsof50patientseach accordingtoacomputer generatedtableofrandomnumbers.
• GroupI(n=50):receivedInj.Propofol1%(2mg/kgofbody weight)
• Group II (n=50): receivedInj. Etomidate (0.3mg/kg of bodyweight)
Patientswithhistoryofallergytostudydrugs,historyof seizuredisorder,presenceofprimaryandsecondarysteroid deficiency/onsteroidmedicationandhypotensivepatients wereexcludedfromstudy.
Allpatientswerepre-medicatedwithtabletsalprazolam 0.25mgandranitidine150mg,thenightbeforethesurgery and instructed for fasting for 8h. On arrival at operation theatre, patientswere attachedwithstandard anesthesia monitoringincludingElectrocardiogram(ECG),Non-invasive blood pressure (NIBP), Pulse oximeter and baseline vital parameterswererecorded. An18G intravenous(I.V.) can-nulawassecuredinlefthandandringerlactate10mL/kg/h wasstarted.
Refusal to consent (14)
On steroid medication (2)
16 patients excluded
100 patients were recruited
Propofol (2mg/kg) n=50
Etomidate (0.3mg/kg) n=50
116 patients assessed for eligibility
Figure1 Studydesign.
was maintained withoxygen and nitrousoxide (70:30) in isoflurane along withintermittent boluses of vecuronium, asrequiredthroughout thesurgery.At theendofsurgery, the residual neuromuscular block was antagonized with neostigmine (0.05mg/kg) and glycopyrrolate (0.01mg/kg) I.V. and extubation was performed when respiration was adequateandpatientwasabletoobeyverbalcommands.
Systolicblood pressure,diastolic bloodpressure, mean arterialpressure, heartrate werecontinuouslymonitored and recorded before induction, at induction and laryn-goscopyfollowedby1,3,5and10minutesafterintubation. Painoninjectionwasmeasuredusing4gradedscale;0---no pain,1---verbalcomplaintofpain,2---withdrawalofarm, 3--- bothverbalcomplaintandwithdrawalofarm.The inci-denceanddegreeofmyoclonicmovementsalsorecordedas follows: 0=no myoclonicmovements, 1=minor myoclonic movements,2=moderatemyoclonicmovements,3=major myoclonicmovements. Episode of apnea, ifoccurred was recorded.
Statisticalanalysis
Data are presented as mean±SD. Patient characteristic data were analysed with one way ANOVA for continuous variablesandchi-squaretestforcategoricalvariables. Sta-tisticalanalysiswasdoneusingSPSS20(IBMSPSSStatistics).
p-Value<0.05wasconsideredsignificant.
Results
A total of 116 patients were assessed for eligibility from December2013toMay2014,outofwhich16patientswere excludedfromstudyonaccountofrefusaltoconsent (four-teen patients) andon steroidmedications(two patients). 100patientswerecompletedthestudyafterrandomization intwogroups(Fig.1).
Both groups were comparable in age, sex, weight and ASAphysical status,withnostatisticallysignificant differ-ences (p>0.05) (Table 1). Pre-operative vitals (HR, SBP, DBP and MAP) were comparable in both groups with no statistically significant differences (p>0.05). Decrease in MAPandincreaseinheart ratewasmorefrombaselinein propofolgroupthanetomidategroupatinduction(p>0.05) (Figs.2and3).Fiftypercentofpatientsreceivedpropofol complainedpainwhile onlyfourpercentpatientin etomi-date group(p>0.05).Also,the severityof painwasmore with propofol (Table 2). Incidence of apnea was similar
Table1 Demographiccharacteristicofpatients(p>0.05).
Variable GroupI GroupII
Sex(female:male) 30:20 27:23 Age(years)mean±SD 29.16±11.38 27.86±10.09 Weight(kg)mean±SD 56.02±11.03 57.4±11.16
ASAgradeI/II 26/24 23/27
Baseline At induction At Laryngoscopy
1 min 3 min 5 min 10 min
Group II Group I
40 60 80 100 120
20
0
Figure2 ShowingMAPatdifferenttimeintervals.A
signifi-cantdecreaseinMAPfrombaselineatinductionwithpropofol incomparetoetomidateisobserved(p>0.05),thereafterMAP becamecomparabletoetomidate(p>0.05).
0 20 40 60 80 100 120
Baseline At induction
At lar yngoscop
y
1 min 3 min 5 min 10 min
Group I Group II
Figure3 ShowingHRatdifferenttimeintervals.Increasein
heart rate from baseline at induction is significantly high in propofolgroup(p>0.05),thenbecame comparableto etomi-date(p>0.05).
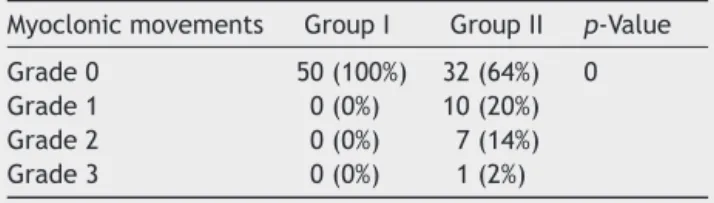
in both groups (p>0.05) (Table 3). Myoclonic movements wereonly seen in etomidate group (p>0.05). Severity of myoclonuswasnotedasgrade1(20%),grade 2(14%)and grade3(2%)(Table4).
Table2 Incidenceandgradingofpainoninjection.
Group Painoninjection p-Value
Grade0 Grade1 Grade2
Table3 Incidenceofapneaoninductioninbothgroups.
Group Apneaoninduction p-Value
Yes No
GroupI 38(76%) 12(24%) 0.271 GroupII 33(66%) 17(34%)
Table4 Incidenceofmyoclonicmovementsinbothgroups.
Myoclonicmovements GroupI GroupII p-Value
Grade0 50(100%) 32(64%) 0
Grade1 0(0%) 10(20%)
Grade2 0(0%) 7(14%)
Grade3 0(0%) 1(2%)
Discussion
Induction of anesthesia is associated with hemodynamic
variationofmildtomoderatedegreedependinguponmany
factors. In our study, we observed that propofol caused
significanthypotensionandtachycardiaatinductionin
com-parison to etomidate. Hypotension occurs with propofol
is mainly due to reduction of sympathetic activity
caus-ing vasodilation or its direct effect on vascular smooth
muscles.12,13Suddenhypotensionandtachycardiahas dele-teriouseffectsonmaintainingthecirculationtovitalorgans in patients of coronary artery disease, valvular stenosis, uncontrolledhypertensionandshock.Onanotherside hemo-dynamicstabilityobservedwithetomidatemaybeduetoits uniquelackofeffectonthesympatheticnervoussystemand onbaroreceptorfunctions.14,15Mayeretal.16andWuetal.17 alsoconcludedthatetomidatepreservehemodynamic sta-bilityduringanesthesia.
Etomidatedoesnothave itslimitationtonormotensive patients for its hemodynamic peculiarity. In various stud-ies, etomidate shown less cardiovascular depression and minimize use of vasopressor agents than other induction agent in sepsis and critically ill patients. Although eto-midate can cause adrenal insufficiency in these patients in postoperative period, clinical consequence of that is stillunclearover itsadvantage topreventhypotensionat induction.18---21
Painduringinjectionofanestheticagentisabad expe-rienceforpatientwhile itquiteembarrassingsituationfor ananesthesiologist.Etomidateshownafavourbleoutcome andit wasvery well supported by Saricaogluet al.22 and Wu etal.17 in their studies. Both agents had shown simi-larityin their respiratorydepressant effect. The episodes of apnea were transient and not associated withany fall in oxygen saturation. Boysen et al.23 in their study con-cluded that there was no significant difference between two groups (propofol and etomidate) asregard to apnea followinginduction.Theonlynegativecharacteristicnoted withetomidatewashighincidenceofmyoclonicjerks.Miner et al.24 was also concluded high incidence of myoclonus (20% vs. 1.8%) in etomidate and propofol group respec-tively.
Conclusion
Inconclusion,etomidateisbetterforitshemodynamic sta-bility over propofol along with less incidence of pain on injection.Onlydrawbackwashighincidenceofmyoclonus. We thereforesuggest thatetomidate isa betteroption in patients particularlypronetohemodynamic fluctuationat induction likeuncontrolled hypertension,septic, critically illandpatientswithcoronaryarterydisease.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Shinn HK, Lee MH, Moon SY, et al. Post-operative nausea andvomitingaftergynecologiclaparoscopicsurgery: compar-isonbetweenpropofolandsevoflurane.KoreanJAnesthesiol. 2011;60:36---40.
2.GrundmannU,SilomonM,BachF,etal.Recoveryprofileand sideeffectsofremifentanil-basedanaesthesiawithdesflurane orpropofolforlaparoscopiccholecystectomy.ActaAnaesthesiol Scand.2001;45:320---6.
3.MaruyamaK,NishikawaY,NakagawaH,etal.Canintravenous atropinepreventbradycardiaandhypotensionduringinduction oftotalintravenousanesthesiawithpropofolandremifentanil? JAnesth.2010;24:293---6.
4.FrazeeBW,ParkRS,LoweryD,etal.Propofolfordeep proce-duralsedationintheED.AmJEmergMed.2005;23:190---5. 5.Ozgul U, Begec Z, Erdogan MA, et al. Effect of
alkalinisa-tionoflignocainefor propofolinjectionpain: aprospective, randomised, double-blind study. Anaesth Intensive Care. 2013;4:501---4.
6.Sarkar M, Laussen PC, Zurakowski D, et al. Hemodynamic responsestoetomidateoninductionofanesthesiainpediatric patients.AnesthAnalg.2005;101:645---50.
7.Morel J, Salard M, Castelain C, et al. Haemodynamic con-sequences of etomidate administration in elective cardiac surgery: a randomized double-blinded study. Br J Anaesth. 2011;107:503---9.
8.Paris A, Philipp M, Tonner PH, et al. Activation of alpha 2B-adrenoceptorsmediatesthecardiovasculareffectsof eto-midate.Anesthesiology.2003;99:889---95.
9.KimTK,ParkIS.Comparativestudyofbrainprotectioneffect betweenthiopentalandetomidateusingbispectralindex dur-ing temporary arterial occlusion. J Korean Neurosurg Soc. 2011;50:497---502.
10.Nyman Y,Von Hofsten K, PalmC,et al. Etomidate-Lipuro is associated with considerably less injection pain in children comparedwithpropofolwithaddedlidocaine.Br JAnaesth. 2006;97:536---9.
11.NymanY,vonHofstenK,RitzmoC,etal.Effectofasmall prim-ingdoseonmyoclonicmovementsafterintravenousanaesthesia induction with Etomidate-Lipuro in children. Br J Anaesth. 2011;107:225---8.
12.HokaS,YamauraK,TakenakaT,etal.Propofol-inducedincrease invascularcapacitanceisduetoinhibitionofsympathetic vaso-constrictiveactivity.Anesthesiology.1998;89:1495---500. 13.MuziM,BerensRA,KampineJP,etal.Venodilationcontributes
to propofol-mediated hypotension in humans. Anesth Analg. 1992;74:877---83.
studyinrabbitscomparingthiopental,propofolandetomidate. ActaMedOkayama.2001;55:197---203.
15.HughesRL,MacKenzieJE.Aninvestigationofthecentrallyand peripherallymediatedcardiovascular effectsofetomidate in therabbit.BrJAnaesth.1978;50:101---8.
16.Mayer M, Doenicke A, Nebauer AE, et al. Propofol and Etomidate-Lipurofor inductionofgeneralanesthesia. Hemo-dynamics, vascular compatibility, subjective findings and postoperativenausea.Anaesthesist.1996;45:1082---4.
17.Wu J, Yao S, Wu Z, et al. A comparison of anesthetic reg-imens using etomidate and propofol in patients undergoing first-trimesterabortions:double-blind,randomizedclinicaltrial ofsafetyandefficacy.Contraception.2013;87:55---62. 18.RayDC,HayAW,McKeownDW.Inductiondrugandoutcomeof
patientsadmittedtotheintensivecareunitafteremergency laparotomy.EurJAnaesthesiol.2010;27:481---5.
19.RayDC,McKeownDW.Effectofinductionagentonvasopressor andsteroiduse,andoutcomeinpatientswithsepticshock.Crit Care.2007;11:56.
20.ZausigYA,BusseH,LunzD,etal.Cardiaceffectsofinduction agentsinthesepticratheart.CritCare.2009;13:144. 21.RayDC,McKeownDW.Etomidateforcriticallyillpatients.Pro:
yeswecanuseit.EurJAnaesthesiol.2012;29:506---10. 22.SaricaogluF,UzunS, ArunO,et al.Aclinicalcomparisonof
Etomidate-Lipuro,propofolandadmixtureatinduction.Saudi JAnaesth.2011;5:62---6.
23.BoysenK, Sanchez R,Krintel JJ,et al.Induction and recov-erycharacteristicsofpropofol,thiopentalandetomidate.Acta AnaesthesiolScand.1989;33:689---92.