rev bras hematol hemoter. 2016;38(3):271–273
w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Case
Report
Transient
red
cell
aplasia
in
two
brothers
with
sickle
cell
anemia
and
erythrovirus
B19
infection
Marina
dos
Santos
Brito
Silva
Furtado
a,
Marina
Lobato
Martins
a,
Rosângela
Maria
de
Figueiredo
b,
Marcos
Borato
Viana
c,∗aFundac¸ãoHemominas,BeloHorizonte,MG,Brazil bHospitalInfantilJoãoPauloII,BeloHorizonte,MG,Brazil cUniversidadeFederaldeMinasGerais,BeloHorizonte,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received26March2016 Accepted11April2016 Availableonline2May2016
Introduction
Erythrovirus B19 (B19V), a member of Parvoviridae family, genusErythrovirus,isasmallnon-envelopedDNAvirus,with approximately5000nucleotides.Therearethreedistinct geno-types(1,2and3)withgenotype1beingthemostprevalentin theworld.1
B19Vinfectionisassociatedwithmanyclinical manifes-tations,dependingontheimmunologicalandhematological statusofthepatient.Thevirushastropismforbonemarrow erythroblasts,onwhichitexertsacytotoxiceffectand deter-minestemporarysuspensionoferythropoiesis,leadingtoa transientepisodeofredcellaplasia.2
Insicklecellanemia(SCA)patients,B19Visknowntobe theetiologicagentoftransientaplasticcrises.3 Manyother complicationsmaybeassociatedwithB19Vinfection,suchas acutesplenicsequestration4,5andacutechestsyndrome.6
ThediagnosisofB19Vinfectioncanbeachievedby detec-tinganti-B19Vantibodiesorbymolecularbiologytechniques that allow the identification ofthe viral DNA using direct
∗ Correspondingauthorat:Al.GuilhermeHenriqueDaniel,94/206,0220-200BeloHorizonte,MG,Brazil. E-mailaddress:[email protected](M.B.Viana).
hybridizationorpolymerasechainreaction(PCR),orevenby directidentificationofthevirusbyelectronmicroscopy.7
TheB19Vseroprevalenceincreaseswithageandcanvary from2to15%inunderfive-year-oldchildren,15to60%for individualsagedsixto19years,between30and60%inadults, andupto85%intheelderlypopulation,8bothindeveloped anddevelopingcountries.9
Inastudy of278childrenwithsicklecelldisease (SSor S0-thalassemia,medianage5.8years;range:0.9–12.3years), ithasbeenshownthatpastorrecentviralinfectionoccurred in29.5% (95%confidenceinterval:24.1–34.9%).5 Thisreport describestheclinicalcourseandthelaboratorytestsoftwo siblingsselectedtoparticipateinthatcohort.
Case
reports
A10-year-oldmale(LLS)withhomozygousSS,hadbeen reg-ularlyfollowedupintheoutpatientclinicoftheBloodCenter inBeloHorizontesincethediagnosisofSCAbytheNewborn ScreeningProgramofMinasGerais,Brazil.Hewasadmittedto
http://dx.doi.org/10.1016/j.bjhh.2016.04.004
272
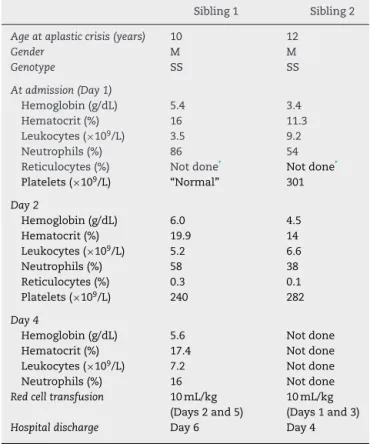
revbrashematolhemoter.2016;38(3):271–273Table1–Bloodcountsduringtransientaplasticcrisesin twosiblingswithsicklecellanemia.
Sibling1 Sibling2
Ageataplasticcrisis(years) 10 12
Gender M M
Genotype SS SS
Atadmission(Day1)
Hemoglobin(g/dL) 5.4 3.4 Hematocrit(%) 16 11.3 Leukocytes(×109/L) 3.5 9.2
Neutrophils(%) 86 54 Reticulocytes(%) Notdone* Notdone*
Platelets(×109/L) “Normal” 301
Day2
Hemoglobin(g/dL) 6.0 4.5
Hematocrit(%) 19.9 14
Leukocytes(×109/L) 5.2 6.6
Neutrophils(%) 58 38
Reticulocytes(%) 0.3 0.1
Platelets(×109/L) 240 282
Day4
Hemoglobin(g/dL) 5.6 Notdone
Hematocrit(%) 17.4 Notdone
Leukocytes(×109/L) 7.2 Notdone
Neutrophils(%) 16 Notdone
Redcelltransfusion 10mL/kg
(Days2and5)
10mL/kg (Days1and3)
Hospitaldischarge Day6 Day4
∗ Reticulocytecountsarenotpartoftheroutinetestsperformedin
thehospitallaboratory;countsontheseconddayofadmission wereperformedintheHemominaslaboratory.
theemergencyroomoftheJoãoPauloIIChildren’sHospitalin BeloHorizontewithahistoryofbackpain,headacheandfever ofupto38.7◦Cfortwodayspriortoadmission.Physical
exam-inationrevealedaheartrateof90bpmandliver3cmbelow thecostalmargin,spleennotpalpableandanicteric.Onthe dayofadmission,hehadtwoepisodesofvomiting,andslurry evacuation.Respiratorysymptomswereabsent.Lowbackpain subsidedthesamedayandtheheadachebecame intermit-tent.Thevomitinganddiarrhearecededthe followingday. Ampicillinwasinitiateduponadmissionbutwasdiscontinued thenextday,sincetherewasnofeverorothersymptomsof bacterialinfection,andradiographicevaluationshowedthat chestandfacewerenormal.BloodcountsareshowninTable1. Beforethehospitaladmission,thispatienthadbeen ran-domly selected for a research study aiming to investigate B19VinfectioninchildrenwithSCA,aspreviouslymentioned. His serum sample had been drawn 16 months before the transientbonemarrowhypoplasiaevent.Inthatsampleno anti-B19Vantibodies(IgGorIgMclass–Biotrin,Ireland)had been detected, nor had viral DNA byquantitative PCR (in-housetest).Oneyearaftertheepisodeoferythroidhypoplasia anew serum sampleofthe patientwas drawn,as recom-mendedbythestudy.Thissamplewaspositiveforanti-B19V IgGantibodiesandnegativeforIgMantibodiesandviralDNA. A 12-year-old male (ALS), sibling of “Case 1”, was also regularly followed up in the outpatientclinic at Fundac¸ão HemominassincethediagnosisofSCAinthenewbornperiod.
Thepatientwasadmittedtothesamehospital13daysafter his brother. Before hospital admission, his symptoms had beenheadacheandrunnynosewithoutfeverforoneweek. They subsidedspontaneously, but afterthreedays,he pre-sentedaheadacheassociatedwithvomitingandafeverpeak of38.7◦C.Ibuprofenwasprescribedatagovernmenthealth
clinicandthesymptomsreceded.Onedaypriortohospital admission,heagainhadheadachesassociatedwithpainin thecervicalspineandvomiting.Hismotherreportedthatthe degreeofherson’spallorhadclearlyincreased.Atadmission, hewas slightly dehydrated,severely paleand mildly jaun-diced.Heartandrespiratoryrateswere110bpmand26breaths per minute,respectively;blood pressurewas110/70mmHg, hisliver was7cmfrom the costalmargin, and spleenwas notpalpable.BloodcountsarealsoshowninTable1. B19V DNAwasdetectedbyrealtimePCR,andtypedasgenotype1 (Figure1).
Comments
B19Vinfectioncausessignificantmorbidityinchildrenwith SCA. Althoughstudies have been reported on the subject, therearestilllimiteddataontheepidemiologyofthis infec-tion,aswellasthecomplicationsassociatedwithit.
IntrafamilialtransmissionofB19Vinfectionisconsidered animportanteventforviralspread.Ithasbeendemonstrated thatthesingleriskfactorforB19Vseroconversioninachild wasthepresenceofsiblingswitharecentB19Vinfection(odds ratio:2.97;95%confidenceinterval:1.29–6.81).2Therateof sec-ondaryinfectioninfamilieswithtwoormorechildrenwith sicklecelldiseasewas56.3%.
Itisknown that thevast majorityofchildrenwithSCA whohaveserologicevidenceofpreviousB19Vinfectionhad not developed symptomatic aplastic crisis,10 as was also demonstratedbyourrecentcohortstudy.5Differentdegrees ofbaselinehemoglobinconcentration,virusload,virus geno-typesorotherunknownfactorscouldexplainthisobservation, althoughgenotypeandvirusloadwerethesameinboth chil-drenduringanosocomialB19Voutbreak,onechildwithvery severemanifestationsandtheotherwithanasymptomatic course.11Itisinterestingtonotethatthediagnosisofacute transientaplasticcrisisinchildrenwithSCAwhoarebeing treatedwithhydroxyureaisnotdifferenttothosewhoarenot beingtreatedwithhydroxyurea.Theclinicalcoursewasvery similar,relapsingorchronicB19Vinfectionwasnotobserved, and the production of B19V-specific immunoglobulins was apparentlynormal.12
Inconclusion,ourreportsuggeststhathostimmunologic background may play a significant role in the pathogene-sisand clinical courseofaplasticcrisessecondary toB19V infection, asboth brothers showed life-threatening clinical manifestations.Sinceserologicalandmoleculartestsarenot alwaysavailable,thereticulocytecountisessentialwhen tran-sientbonemarrowhypoplasiacausedbyB19Vissuspected,so thatpropersupportivecarecanbeimmediatelystarted.
Conflicts
of
interest
revbrashematolhemoter.2016;38(3):271–273
273
1.0e+001
1.0e+000 CT
Threshold
1.0e–001
Delta Rn
Delta Rn vs cycle
1.0e–002
1.0e–003
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
Cycle number
17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40
Figure1–In-houserealtimepolymerasechainreactionassayusingspecifichydrolysisprobestodetecterythrovirusB19 genotypes1,2,and3.Positiveamplificationforgenotype1(blackline)wasdetectedinCase2.Thehorizontalgreenline representsthethresholdforpositivity.Intersectionofthislinewiththeblackline(arrow)indicatesthecycleamplification threshold(Ct)value.TheearlyCt=12pointsforahighvirusload.Fluorescentsignalsbelowthethresholdindicatenegative resultsforgenotypes2and3.
Ethical
approval
ThestudywasapprovedbytheHumanEthicsCommitteeon ResearchofFundac¸ãoHemominasandUniversidadeFederal de MinasGerais. Itwas conductedin accordance withthe Helsinki Declarationasrevised in2008. Childrenand their parentssignedaninformedconsentform.
Funding
Conselho Nacional de Desenvolvimento Científico e Tec-nológico,Brazil(CNPq),NúcleodeAc¸õesePesquisaemApoio Diagnóstico,Brazil(Nupad),Fundac¸ãodeAmparoàPesquisa doEstadodeMinasGerais,Brazil(Fapemig).
r
e
f
e
r
e
n
c
e
s
1. ServantA,LapercheS,LallemandF,MarinhoV,deSaintMaur G,MeritetJF,etal.Geneticdiversitywithinhuman
erythroviruses:identificationofthreegenotypes.JVirol. 2002;76(18):9124–34.
2. Smith-WhitleyK,ZhaoH,HodinkaRL,KwiatkowskiJ,CecilR, CecilT,etal.EpidemiologyofhumanparvovirusB19in childrenwithsicklecelldisease.Blood.2004;103(2): 422–7.
3. SerjeantGR,SerjeantBE,ThomasPW,AndersonMJ,PatouG, PattisonJR.Humanparvovirusinfectioninhomozygous sicklecelldisease.Lancet.1993;341(8855):1237–40.
4. YatesAM,HankinsJS,MortierNA,AygunB,WareRE. Simultaneousacutesplenicsequestrationandtransient
aplasticcrisisinchildrenwithsicklecelldisease.Pediatr BloodCancer.2009;53(3):479–81.
5.DosSantosBritoSilvaFurtadoM,BoratoVianaM,Silqueira HicksonRriosJ,LaísLimaGontijoR,MariaSilvaC,doVal RezendeP,etal.PrevalenceandincidenceoferythrovirusB19 infectioninchildrenwithsicklecelldisease:theimpactof viralinfectioninacuteclinicalevents.JMedVirol. 2016;88(4):588–95.
6.TsitsikasDA,GallinellaG,PatelS,SeligmanH,GreavesP, AmosRJ.Bonemarrownecrosisandfatembolismsyndrome insicklecelldisease:increasedsusceptibilityofpatientswith non-SSgenotypesandapossibleassociationwithhuman parvovirusB19infection.BloodRev.2014;28(1):23–30.
7.HeegaardED,BrownKE.HumanparvovirusB19.Clin MicrobiolRev.2002;(3):485–505.
8.KellyHA,SiebertD,HammondR,LeydonJ,KielyP,MaskillW. Theage-specificprevalenceofhumanparvovirusimmunity inVictoria,Australiacomparedwithotherpartsoftheworld. EpidemiolInfect.2000;124(3):449–57.
9.IwalokunBA,IwalokunSO,HodonuSO.Seroprevalenceof parvovirusB19antibodiesandevidenceofviremiaamong Nigerianpatientswithsicklecellanemia.JBiomedRes. 2013;27(4):272–82.
10.ZimmermanSA,DavisJS,SchultzWH,WareRE.Subclinical parvovirusB19infectioninchildrenwithsicklecellanemia.J PediatrHematolOncol.2003;25(5):387–9.
11.SlavovSN,KashimaS,Silva-PintoAC,AmarillaAA,Aquino VH,CovasDT.Molecularandclinicalevaluationoftheacute humanparvovirusB19infection:comparisonoftwocasesin childrenwithsicklecelldiseaseanddiscussionofthe literature.BrazJInfectDis.2013;17(1):97–101.
12.HankinsJS,PenkertRR,LavoieP,TangL,SunY,HurwitzJL. ParvovirusB19infectioninchildrenwithsicklecelldiseasein thehydroxyureaera.ExpBiolMed(Maywood).