w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Epidemiological
characterization
of
ostomized
patients
attended
in
referral
Center
from
the
city
of
Maceió,
Alagoas,
Brazil
夽
Manoel
Álvaro
de
Freitas
Lins
Neto
∗,
Danillo
Omena
de
Araújo
Fernandes,
Eveline
Leite
Didoné
UniversidadeFederaldeAlagoas(UFAL),Maceió,AL,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received12November2013
Accepted11August2014 Availableonline25March2016
Keywords: Ostomy
Descriptiveepidemiology Colorectalneoplasia Colostomy
Ileostomy
a
b
s
t
r
a
c
t
Introduction:Severalclinicalconditionsimplytherealizationofabowelostomy,asa treat-mentoption.However,thepresenceofastomaisanimportantlimitationinthequalityof lifeoftheostomizedpatient.
Aim:TodefinetheepidemiologicalprofileofpatientsenrolledintheOstomyProgramfrom tworeferenceservicesinthecityofMaceió,Alagoas,regardinggender,age,classification (aspermanentortemporary),typeofostomywithrespecttothebowelsegmentused,and causes.
Method:Thiswasadescriptivecross-sectionalstudywhosedatawereobtainedfrom regis-trationformsofactivepatientsinOstomyProgramsonMay2013.
Results:Of216patientsanalyzed,50.5%werefemaleand49.5%male.Theagegroupwith thehighestnumberofcaseswasthatbetween60and69years(23.6%)andtheaverageage was51.3years.Colostomiesaccountedfor89.4%oftheproceduresperformed,and56.9%of proceduresweretemporaryostomies.Asforthecause,themostprevalentwascolorectal cancer(40.7%),followedbytrauma(18.1%)andacuteabdomen(12.0%).
Conclusion:Thestudyprovidesrelevantdatathatcanbeusedasinputforpreventionand strategiestoimprovethehealthoftheostomizedpopulation.
PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeColoproctologia. ThisisanopenaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
夽
ResearchlinkedtotheServiceofColoproctology,HospitalUniversitárioProfessorAlbertoAntunes(HUPAA),Maceió,AL,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](M.Á.deFreitasLinsNeto). http://dx.doi.org/10.1016/j.jcol.2014.08.016
Caracterizac¸ão
epidemiológica
de
pacientes
ostomizados
atendidos
em
centro
de
referência,
Maceió,
Alagoas,
Brasil
Palavras-chave: Ostomia
Epidemiologiadescritiva Neoplasiascolorretais Colostomia
Ileostomia
r
e
s
u
m
o
Introduc¸ão: Diversascondic¸õesclínicasimplicamarealizac¸ãodeumaostomiaintestinal comoopc¸ãodetratamento.Entretanto,apresenc¸adeumestomaéumimportantelimitador naqualidadedevidadapessoaostomizada.
Objetivo: Definir o perfil epidemiológico dos pacientes cadastrados no Programa de Ostomizadosdedoisservic¸osdereferênciaemMaceió,Alagoasquantoagênero,idade, classificac¸ãodaostomiaemdefinitivaoutemporária,tipodeostomiaquantoaosegmento intestinalutilizadoecausas.
Método: Trata-sedeumestudotransversaldescritivocujosdadosforamobtidosdefichas cadastraisdepacientesativosemProgramasdeOstomizadosnomêsdemaiode2013. Resultados: Dos216pacientesanalisados,50,5%eramdogênerofemininoe49,5%dogênero masculino.Afaixaetáriacommaiornúmerodecasosfoiade60a69anos(23,6%)ea médiadeidadefoide51,3anos.Ascolostomiasrepresentaram89,4%dosprocedimentos realizadose56,9%dasostomiasforamtemporárias.Quantoàcausa,amaisprevalentefoi ocâncercolorretal(40,7%),seguidodostraumatismos(18,1%)edoabdomeagudo(12,0%). Conclusão: Oestudoapresentadadosrelevantesquepodemserutilizadoscomosubsídio paraac¸õesdeprevenc¸ãoeestratégiasdemelhoriadasaúdedapopulac¸ãoostomizada.
PublicadoporElsevierEditoraLtda.emnomedaSociedadeBrasileirade Coloproctologia.EsteéumartigoOpenAccesssobalicençadeCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
OstomyisaderivativeoftwowordsofGreekorigin,osand
tomé, whichmeans “openingofamouth” andindicate the
externalizationofahollowviscusinadifferentpointofits naturalorifice,aimingattheconstructionofastoma.1–4
Severalcriteriaareusedfortheclassificationofstomata.
Consideringtheirfunction,theseprocedurescanbedivided
intoventilation,nutrition,drainageoreliminationstomata.5
Theselatterconstituteasurgicalopeningintheabdominal
wall,aimingtopromotetheeliminationofwastesuchasfeces
andurine.Urinarystomataareperformedonpatientswith
diseasesinvolvingtherenalpelvis,ureters,bladderand ure-thra,inordertopreserverenalfunction.Ontheotherhand,
anintestinalstomaisrecommendedwhensomepartofthe
bowelsuffersdysfunction,obstructionorinjury.4
According to the exteriorized intestinal segment, an
intestinal stoma can also be termed as an ileostomy,
colostomyorcecostomy.Colostomyisthegenericnameofthe
proceduretobeperformed,beingcharacterizedbythe
exte-riorizationofthecolonthroughtheabdominalwall,forthe
purposeoffecalelimination.Onthe otherhand,the
artifi-cialopeningbetweenileum,atthesmallintestine,andthe
abdominalwallisreferredtoasanileostomy;and between
thecaecum,alsoatthesmallintestine,andthe abdominal
wallisreferredtoasacecostomy.6
Ostomiescan still beclassified astemporary or
perma-nent,depending on the etiology ofthe disease that led to
its creation. Temporary ostomiesare created toprotect an
anastomosis,inview ofitsclosure ina shorttime; onthe
otherhand,permanentostomiesareperformedwhenthere
is no possibility of restoringthe bowel transit.1 The main
advantageofperforminganostomy,inrelationtotheprimary repair,isthetheoreticalprincipleofreducingthemorbidity andmortalityofasuturedehiscence,orofanintra-abdominal infection.7
Theclinicalconditionsthatleadtotheconstructionofa
bowelostomy arerelatedtobenignandmalignant diseases
involving somebody organs,beingvery common in
oncol-ogy,traumaandgastroenterologicalsurgery.8Amongthemost
commonaretraumas,congenitaldisorders,inflammatory
dis-easesandcolorectaltumors.1,9–12
According to estimates ofthe National Cancer Institute
(INCA)fortheyear2012,inBrazilthecolorectalcancerappears
asthethirdmostcommonneoplasiainbothmenandwomen,
exceptforthenon-melanomaskintumors.Theincidenceand
mortalityarehigherinmen,andagoodprognosisis
consid-eredifthe conditionisdiagnosedinitsearlystages.13 The
surgicalresectionofthe affectedsiteand the
implementa-tionofapermanentcolostomyconstitutethemosteffective
therapy.14
Although most studies consider cancer as the leading
causeofbowelostomycreation,abdominaltraumahasalso
been implicatedasanimportantcause,especiallyin
emer-gencycarereferencehospitals,whichreflectsthesocialreality withitshighratesofviolence.2,15
Sincethe twentiethcentury, alargeprogressinsurgical
techniquesusedinostomycreationandintheequipmentand
devicesavailablehavebeenobserved,aswellasagrowing con-cernforthequalityoflife,consideringthatthepresenceofa stomacanbeaseriouslimitingfactorforthequalityoflifeof ostomizedpatients.4,14,16,17
Inthiscontext,severalepidemiologicalstudieshavebeen conductedwithostomizedpatients2–4,6,12,14–16,18–23inorderto
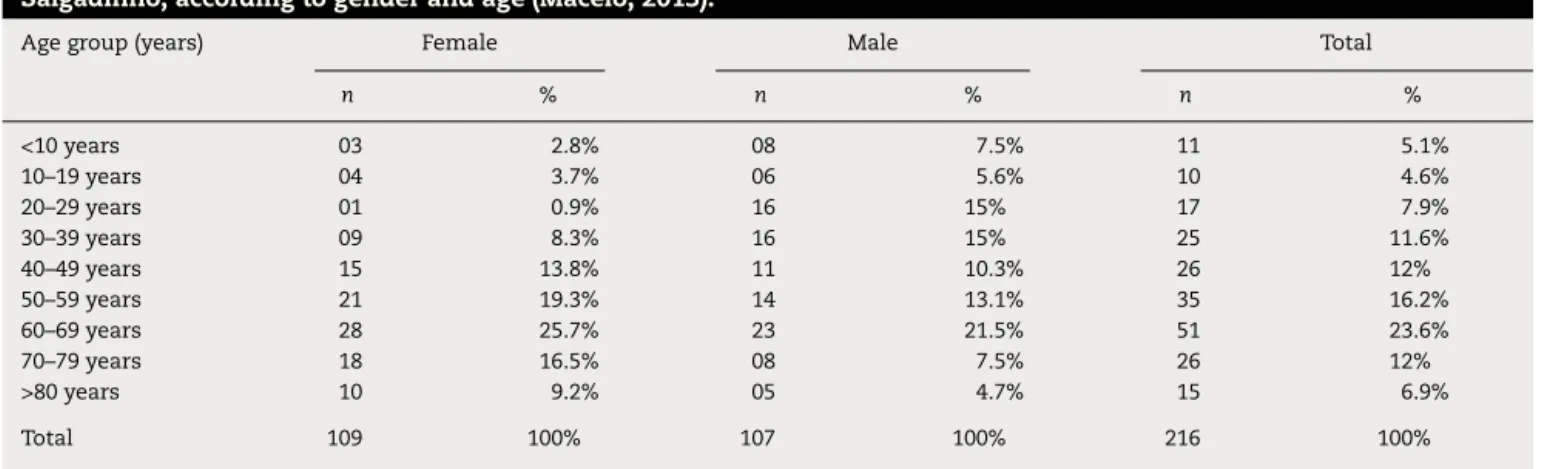
Table1–NumericandpercentagedistributionofpatientsenrolledintheOstomyProgramofCACONandPam Salgadinho,accordingtogenderandage(Maceio,2013).
Agegroup(years) Female Male Total
n % n % n %
<10years 03 2.8% 08 7.5% 11 5.1%
10–19years 04 3.7% 06 5.6% 10 4.6%
20–29years 01 0.9% 16 15% 17 7.9%
30–39years 09 8.3% 16 15% 25 11.6%
40–49years 15 13.8% 11 10.3% 26 12%
50–59years 21 19.3% 14 13.1% 35 16.2%
60–69years 28 25.7% 23 21.5% 51 23.6%
70–79years 18 16.5% 08 7.5% 26 12%
>80years 10 9.2% 05 4.7% 15 6.9%
Total 109 100% 107 100% 216 100%
allowingformeasurestobetakentominimizethe
deterio-rationofqualityoflifeafterthestomacreation.
Basedontheaboveconsiderations,thisstudyaimsto char-acterizeepidemiologicallyostomizedpatientsintworeferral
centers:CentrodeAltaComplexidadeem Oncologia(CACON)e
PamSalgadinho.
TheresearchprojectwassubmittedtotheEthics
Commit-teeinResearchofthe UniversidadeFederaldeAlagoas,being approvedonApril2,2013,undernumber13195813.2.0000.5013
and inaccordance with ethicalprinciples. Theresearchers
emphasize that the confidentiality of information and the
identificationofcasesweresecured,representingnoharmto
affected individuals.Theresearchwas conductedin
accor-dancewiththe ethicalprinciplesestablishedbyResolution
466/2012CONEP/MS.
Methods
Thisisadescriptive, cross-sectionalstudy usingdatafrom
patientsenrolledintheOstomy ProgramofCACONseenat
theHospitalUniversitárioHospitalProfessorAlbertoAntunes
(HUPAA)andintheOstomyProgramoftheEmergencyCare
Unit (Unidade de Pronto Atendimento/UPA), Pam Salgadinho, bothinthecityofMaceió,Alagoas.
ThedatacollectionwasconductedinMay2013,through
a questionnaire based on the registration forms of active
ostomizedpatientsduringthisperiod.Toformthesampleof
thisstudy,allostomizedpatientsregisteredinCACONorPam
SalgadinhoOstomyProgram were included.Thosepatients
who underwentbowel transitreconstructionor withdeath
outcomewereexcluded.
Thecollecteddatawereseparatedintonominalvariables,
suchasgender,causeofostomy,typeofostomyandits
per-manencetime(permanentortemporary),besidesnumerical
variablessuchasage.Thesedatawereprocessedandanalyzed usingMicrosoft®Excelprogram.
Results
Intotal,216caseswereanalyzed,ofwhich53patientsfrom
CACONand163fromPAMSalgadinho,besidesfivepatients
whosedatainmedicalrecordswerenotproperlyfilledand
therefore were excluded from the study. From the cases
analyzed, 109patients(50.5%)were femaleand 107(49.5%)
weremale.Themeanagewas51.3years(45.1yearsformales
and57.3yearsforfemales)andthemedianagewas55years.
AccordingtoTable1,theagegroupwiththehighestprevalence wasthatbetween50and69years(39.8%).
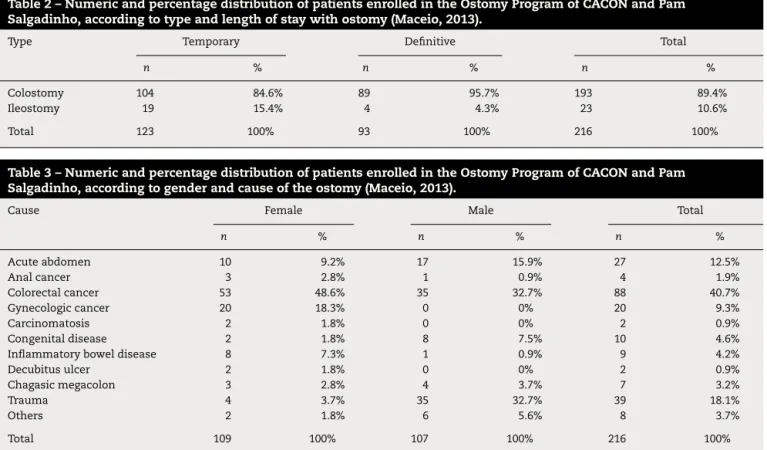
InTable2,inrelationtothebowelsegmentused,193(89.4%)
werecolostomiesand23(10.6%)wereileostomies;according
tostomapermanencetime,93(43.0%)werepermanentand
123(57%)weretemporary.
Asforthecausethatledtostomacreation(Table3),the
mostprevalentwascolorectalcancer,with88cases(40.7%),
ofwhich64werelocatedintherectum,13inthecolon,six
intherectosigmoidjunction,fourinthesigmoidandonein
anunspecifiedsite.Thesecondleadingcauseofostomywas
traumawith39cases(18.1%),ofwhich31wereduetogunshot
injury, three dueto knifeinjury, four from closed
abdomi-naltraumaandonefromanunknowncause.Acuteabdomen
representedthethirdleadingcauseofostomywith27cases
(12.5%),14withobstructiveorigin,seveninflammatorycases,
three byperforation and three from an unspecifiedorigin.
Gynecological malignancies represented the fourth leading
causewith20cases(9.3%),ofwhich17caseswereofcervical cancerandthreecasesofovariancancer.
Congenitaldiseaseswereobservedin10cases(4.6%):five
casesofHirschsprungdiseaseandfiveofimperforateanus.
Therewerealsoninecases(4.2%)ofinflammatorybowel
dis-ease: seven casesofCrohn’sdisease and twoofulcerative
colitis;andsevencases(3.2%)ofChagasmegacolon,four(1.9%)
ofanalcancer,two(0.9%)ofcarcinomatosis,andtwo(0.9%)
ofboweltransitchangeduetodecubituseschars.Eightother
causes ofostomy were representedbyonlyonecaseeach,
amountingeachto0.4%oftotalcasesandbeingrepresented
by: anal abscess, retroperitoneal stroma neoplasia, Ogilvie
syndrome,bladder cancer,rectal-cutaneousfistula,
colorec-talanastomosisdehiscence,infectionatthesurgicalsitedue
tohipdisarticulationprocedureandoneofunknowncause.
Discussion
Of216patients studied,the genderratiowas verycloseto
1:1,similartoresultsofotherstudies(2,14,17,20).Inthose
studiesshowingasignificantlyhigheramountofmaleversus
Table2–NumericandpercentagedistributionofpatientsenrolledintheOstomyProgramofCACONandPam Salgadinho,accordingtotypeandlengthofstaywithostomy(Maceio,2013).
Type Temporary Definitive Total
n % n % n %
Colostomy 104 84.6% 89 95.7% 193 89.4%
Ileostomy 19 15.4% 4 4.3% 23 10.6%
Total 123 100% 93 100% 216 100%
Table3–NumericandpercentagedistributionofpatientsenrolledintheOstomyProgramofCACONandPam
Salgadinho,accordingtogenderandcauseoftheostomy(Maceio,2013).
Cause Female Male Total
n % n % n %
Acuteabdomen 10 9.2% 17 15.9% 27 12.5%
Analcancer 3 2.8% 1 0.9% 4 1.9%
Colorectalcancer 53 48.6% 35 32.7% 88 40.7%
Gynecologiccancer 20 18.3% 0 0% 20 9.3%
Carcinomatosis 2 1.8% 0 0% 2 0.9%
Congenitaldisease 2 1.8% 8 7.5% 10 4.6%
Inflammatoryboweldisease 8 7.3% 1 0.9% 9 4.2%
Decubitusulcer 2 1.8% 0 0% 2 0.9%
Chagasicmegacolon 3 2.8% 4 3.7% 7 3.2%
Trauma 4 3.7% 35 32.7% 39 18.1%
Others 2 1.8% 6 5.6% 8 3.7%
Total 109 100% 107 100% 216 100%
whereasinthosestudieswithfemalepredominance,themain
causeofostomywereneoplasms.4,6,12
Themeanagewas51.3years.Inotherstudies,themean
agerangedfrom39to73years,sothatahighermeanagewas foundinstudieswithhigherprevalenceofneoplasia,whereas alowermeanageindicatedhighprevalenceoftraumaascause ofthestomas.4,7,12,14,18,21,22
Itwasobservedalsoamismatchwhengenderwas
com-paredwith age of patients. In those agedunder 40 years,
73%ofpatients weremale. Mantovaniet al.,23 inasimilar study,found63.9%ofmalesunder45years;andViolinetal.14
observed70%ofmalesunder50years.Thisprevalencecanbe
explainedbytheetiologythatimpliedtheostomycreationas anecessarysurgicalprocedure.
Like most studies,6,12,14,20,22,23 colorectal cancer was
responsibleformost ofthecauses ofostomy,representing
40.7%ofcases,mainly locatedintherectum, which
corre-spondedto72.7% ofthe totaland29.6% ofallcases,being
alsothemaincauseinwomen(48.6%)andmen(32.7%),with
equivalencetotraumacasesinmen.
Traumawasthesecondmostprevalentcause,with18.1%
ofcases,ofwhich89.4%weremale.Similardatawerefound
inastudyinParaná,where87%ofostomizedpatientswith
ostomataduetotraumaweremale.23
Mortalityfromexternalcausesinaspecificpopulation con-stitutesanexcellentindicatortoanalyzethehealthsituation withrespecttoaccidentsand violence.InAlagoas,in2010, accordingtofiguresprovidedbyComputerDepartmentof Sis-temaÚnicodeSaúde/SUS(DATASUL),3403deathsbyexternal
causeswererecorded;ofthese,88.5%weremale.
NationaldataaresimilartothosefromthestateofAlagoas,
witharecordof143,149deathsfromexternalcausesinthe
sameyear,with82.7%occurringinmales.24Thesedatareflect
thesocialrealitythatmen,especiallyyoungpeople, experi-ence today, livingina situation ofsocialvulnerability and
increased risk of death from accidents. Strengthening the
deathstatistics,weobservedthat94.1%ofpatientsbetween
20 and 29 yearswere male, aswell as93.5% ofthosewho
underwentostomyduetogunshotpenetratingtrauma.
Althoughmalesweremoreprevalentthanfemalesinthe
agegroupunder40years,57%ofmaleostomypatientswere
older than 40 years;however, the highestconcentrationof
cases forbothsexes was the age group of60–69years.Of
allostomizedwomen,84.4%wereabove40years.Inanother
study,although46.3%of477patientswerefemale,this per-centageroseto51.4%forthosepatientsover45years.23Thus,
thedataintheliteratureshowaprevalenceofolderwomen,
asoccurredinthepresentstudy.
Similardatatothosereportedbyotherauthorswerealso
found in our study, when it was observed that colostomy
(89.45%) prevailed over ileostomy (10.6%) procedures.2,22
However,althoughmostauthorshavereportedthatmore
per-manentversustemporaryproceduresareperformed,6,12,22we
foundaprevalenceof57%oftemporaryversus43.0%of
per-manentostomies.
Conclusion
Themainreasonforcarryingouttheostomywascolorectal
cancer,andrectalcancerwasthetypefoundmostfrequently.
Agegroupof60–69yearsandfemaleswerethemostprevalent
groups.Trauma–thesecondleadingcause–affectedmainly
theyoungmalepopulation.Temporarycolostomieswerethe
Inthisstudy,somedatathatcanbeusedasabasisfor strategiestoimprovehealthinthegroupofostomizedpatients arepresented.Suchinformationcouldhelphealth profession-alstobetterunderstandthecharacteristicsofthepopulation, aswellastoconducteducationalactivitiesinordertoimprove thequalityoflifeofpatientsafterstomacreation.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. GemelliLMG,ZagoMMF.Ainterpretac¸ãodocuidadocomo ostomizadonavisãodoenfermeiro:umestudodecaso.Rev LatAmEnferm.2002;10:34–40.
2. LuzMHBA,AndradeDS,AmaralHO,BezerraSMG,Benício CDAV,LealACA.Caracterizac¸ãodospacientessubmetidosa estomasintestinaisemumhospitalpúblicodeTeresina-PI. TextoContexto–Enferm.2009;18:140–6.
3. SedaMJA,VillegasMLIC,ÁlvarezSIP,SantiestebánSN, BarrientosJVR,ValdésGJO.Experienciadelaclínicade estomasdelH.R.1◦deOctubreISSSTE.RevEspecMedQuir.
2004;9:33–7.
4. FernandesRM,MiguirELB,DonosoTV.Perfildaclientela estomizadaresidentenomunicípiodePonteNova,Minas Gerais.RevBrasColoproctol.2010;30:385–92.
5. SainzML,RedínD,MiguelRS,BaleztenaJ,SantosMA,PetriM, etal.Problemasdeutilizacióndemedicamentosem
pacientesenterostomizados.AnSistSanitNavar. 2003;26:383–440.
6. StummEMF,OliveiraERA,KirschnerRM.Perfildepacientes ostomizados.SciMed(PortoAlegre).2008;18:26–30. 7. Biondo-SimõesMLP,BrennerS,LemosR,DuckD,ReySD.
Análisedascomplicac¸õespós-operatóriasemdecolostomias. ActaCirBras.2000;15:53–7.
8. BatistaMRFF,RochaFCV,SilvaDMG,SilvaJGJ.Autoimagemde clientescomcolostomiaemrelac¸ãoàbolsacoletora.RevBras Enferm.2011;64:1043–7.
9. SilvaAL,ShimizuHE.ArelevânciadaRededeApoioao estomizado.RevBrasEnferm.2007;60:307–11.
10.BecharaRN,BecharaMS,BecharaCS,QueirozHC,OliveiraRB, MotaRS,etal.AbordagemMultidisciplinardoOstomizado. RevBrasColoproctol.2005;25:146–9.
11.JainS,McGoryML,KoCY,SverdlikA,TomlinsonJS,Wendel CS,etal.Comorbiditiesplayalargerroleinpredicting
health-relatesqualityoflifecomparedtohavinganostomy. AmJSurg.2007;194:774–9.
12.MacêdoMS.Perfildosostomizadosatendidosemhospital privadonomunicípiodeTeresina–PI[Trabalhodeconclusão decurso].Teresina:UniversidadeFederaldoPiauí;2001. 13.InstitutoNacionaldeCâncer[Internet],MinistériodaSaúde,
Brasil.Estimativa2012:incidênciadeCâncernoBrasil. Brasília(DF):INCA;2012.Availablein:
http://www.inca.gov.br/estimativa/2012/index.asp?ID=5 [accessed01.10.12].
14.ViolinMR,MathiasTAF,UchimuraTT.Perfildeclientes colostomizadosinscritosemprogramadeatenc¸ãoaos estomizados.RevEletrEnferm.2008;10:924–32.
15.VonBahtenLC,NicoluzziJE,SilveiraF,NicollelliGM,Kumagai LY,LimaVZ.MorbimortalidadedaReconstruc¸ãodeTransito IntestinalColônicaemHospitalUniversitário–Análisede42 Casos.RevBrasColoproctol.2006;26:123–7.
16.SouzaAPMA,SantosIBC,SoaresMJGO,SantanaIO.Perfil clínico-epidemiológicodelospacientesatendidosycensados enelCentroParaibanodeOstomizados-JoãoPessoa,Brasil. Gerokomos.2010;21:183–90.
17.Mengual-BallesterM,García-MarínJA,Pellicer-FrancoE, Guillén-ParedesMP,García-GarcíaML,Cases-BaldóMJ,etal. Protectiveileostomy:complicationsandmortalityassociates withclosure.RevEspEnfermDig.2012;104:350–4.
18.PereiraAPS,CesarinoCB,MartinsMRI,PintoMH,NetinhoJG. Associac¸ãodosfatoressociodemográficoseclínicosà qualidadedevidadosestomizados.RevLatAmEnferm. 2012;20:93–100.
19.BritoJR,JiménezVK,TolorzaLG,SiquésLP,RojasPF,Barrios PL.OstomíasenIquique:característicasepidemiológicas.Rev ChilCir.2003;55:580–3.
20.SantosCHM,BezerraMM,BezerraFMM,ParaguassúBR.Perfil doPacienteOstomizadoeComplicac¸õesRelacionadasao Estoma.RevBrasColoproctol.2007;27:16–9.
21.SilvaJB,CostaDR,MenezesFJC,TavaresJM,MarquesAG, EscalantesRD.Perfilepidemiológicoemorbimortalidadedos pacientessubmetidosàreconstruc¸ãodetrânsitointestinal: experiênciadeumcentrosecundáriodonordestebrasileiro. ArqBrasCirDig.2010;23:150–3.
22.SasakiVDM,PereiraAPS,FerreiraAM,PintoMH,GomesJJ. Healthcareserviceforostomypatients:profileofthe clientele.JColoproctol.2012;31:232–9.
23.MantovaniMF,MunizMR,SimõesMC,BoschcoMD,Oliveira GD.Operfildosusuárioscadastradosnaassociac¸ão paranaensedeostomizados–APO.CogitareEnferm. 2007;12:76–81.
24.MinistériodaSaúde.Óbitoporcausasexternasporsexo segundoUnidadedaFederac¸ão.Availablein: