w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Socioeconomic
and
therapy
factor
influence
on
self-reported
fatigue,
anxiety
and
depression
in
rheumatoid
arthritis
patients
Mirjana
Lapˇcevi´c
a,
Mira
Vukovi´c
b,
Branislav
S.
Gvozdenovi´c
c,∗,
Vesna
Mioljevi´c
d,
Sne ˇzana
Marjanovi´c
eaPrimaryHealthcareCenter,DepartmentofGeneralMedicine,Belgrade,Serbia bGeneralHospitalValjevo,EducationCenter,Belgrade,Serbia
cPharmaceuticalProductDevelopmentSerbia,PharmacovigilanceDepartment,Belgrade,Serbia dClinicalCenterofSerbia,DepartmentofHospitalEpidemiologyandNutritionHygiene,Belgrade,Serbia eGeneralHospitalValjevo,DepartmentofPsychiatry,Valjevo,Serbia
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received22March2016 Accepted20December2016 Availableonline11March2017
Keywords:
Rheumatoidarthritis TherapyFatigue Anxiety Depression
a
b
s
t
r
a
c
t
Introduction:Fatigue,anxietyanddepressionareveryfrequentsymptomsinpatientswith rheumatoidarthritis(RA).
Goals:Inthisstudyweevaluatedtheinfluenceofsocioeconomiccharacteristics,therapyand comorbiditiesontheself-reportedhighfatigue,anxietyanddepressioninpatientswithRA. Method:Multicenter cross-sectional study was performed in 22 health institutions in SerbiaduringtheperiodfromApril–August2014inpopulationofolderRApatients. Self-reportedpatientshealthstatuswasmeasuredby:FatigueAssessmentScale,PatientHealth Questionnaire-9andGeneralizedAnxietyDisorder-7.Treatmentmodalitiesweredefined as: (1) non-steroidal anti-inflammatory drugs (NSAIDs)and/or analgesics and/or corti-costeroids; (2) synthetic disease-modifying antirheumatic drugs (DMARDs)alone or in combinationwithcorticosteroidsand/orNSAIDsand(3)anyRAtreatmentwhichincludes biologicDMARDs.
Results:Thereweresignificantpredictorsofhighdepression:syntheticDMARDstherapyin combinationwithcorticosteroidsand/orNSAIDs,physiotherapistself-payment,frequent taxiuse,alternativetreatmentandemploymentstatus.Theneedforanotherperson’s assis-tance,supplementalcalciumtherapyandprofessionalqualificationswerethepredictorsof ahighfatigue,whereastheageabove65yearshadtheprotectiveeffectonit.Anxietywasan independenthighfatiguepredictor.Thepredictorsofahighanxietywere:gastroprotection withproton-pumpinhibitorsandpatientoccupation.
∗ Correspondingauthor.
E-mail:[email protected](B.S.Gvozdenovi´c).
http://dx.doi.org/10.1016/j.rbre.2017.02.004
Conclusion: Socioeconomicpredictorsofself-reportedhighdepression,anxietyorfatigue aredifferentforeachofthementionedoutcomes,whileaccompaniedwiththebasicRA treatmenttheyexclusivelyexplainahighdepression.Theanxiety,jointedwiththe socioeco-nomicvariablesandsupplementaltherapy,isasignificantfatiguepredictorinRApatients. ©2017ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Influência
de
fatores
socioeconômicos
e
de
tratamento
sobre
a
fadiga,
ansiedade
e
depressão
autorrelatadas
em
pacientes
com
artrite
reumatoide
Palavras-chave: Artritereumatoide TratamentoFadiga Ansiedade Depressão
r
e
s
u
m
o
Introduc¸ão:Afadiga,aansiedadeeadepressãosãosintomasmuitofrequentesempacientes comartritereumatoide(AR).
Objetivos: Neste estudo, avaliou-se a influência de características socioeconômicas, característicasdetratamentoecomorbidadesnaelevac¸ãonafadiga,ansiedadeedepressão autorrelatadasempacientescomAR.
Método: Esteestudotransversal multicêntricofoi feitoem 22instituic¸ões desaúdena Sérviadeabrilaagostode2014napopulac¸ãodepacientesidososcomAR.Ostatusde saúdeautorrelatadodospacientesfoimedidopelosinstrumentosFatigueAssessmentScale, PatientHealthQuestionnaire-9eGeneralizedAnxietyDisorder-7.Asmodalidadesdetratamento foramdefinidascomo:1)anti-inflamatóriosnãoesteroides(AINE) e/ouanalgésicose/ou corticosteroides;2)fármacosantirreumáticosmodificadoresdadoenc¸asintéticos(DMARD) isoladamenteouemcombinac¸ãocomcorticosteroidese/ouAINEe3)qualquertratamento paraaARqueincluísseDMARDbiológicos.
Resultados: Houvepreditoressignificativosdedepressãoelevada:tratamentocomDMARD sintéticos em combinac¸ão com corticosteroides e/ou AINE, pagamento particular de fisioterapia,usofrequentedeservic¸osdetáxi,terapiasalternativasestatusocupacional. Anecessidadedeassistênciadeoutrapessoa,otratamentosuplementarcomcálcioeas qualificac¸õesprofissionaisforamospreditoresdefadigaelevada.Aidadeacimade65anos teveumefeitoprotetorsobreafadigaelevada.Aansiedadefoiumpreditorindependente defadigaelevada.Ospreditoresansiedadeelevadaforam:gastroprotec¸ãocominibidores dabombadeprótonseocupac¸ãodopaciente.
Conclusão: Os preditoressocioeconômicos de níveiselevados de depressão, ansiedade ou fadiga autorrelatadas são diferentes para cada um dos desfechos mencionados; quandoacompanhadosdotratamentobásicoparaaAR,essespreditoressocioeconômicos explicam exclusivamente uma depressão elevada. A ansiedade, associadaàs variáveis socioeconômicaseaotratamentocomplementar,éumimportantepreditordafadigaem pacientescomAR.
©2017ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Rheumatoidarthritis(RA)isamultifactorialsystemicchronic inflammatorydisease that primarilycauses pain, swelling, joint stiffness and loss of joint function.1 If not properly
treatedtheRAcancausejoint damageincluding their per-manentdestruction.2TheRAcausesjointdamageduringthe
firstorsecondyearofthedisease.Thatiswhyanearly diagno-sisandanadequatetreatmentofRAareveryimportant.The RAtreatmentgoalistheachievementofclinicalremission, i.e.discontinuationofthediseaseactivity.3Byincludingone
synthetic Disease-Modifying Antirheumatic Drug (DMARD) or, if necessary, two of them in combination during six monthsitisexpectedtoachievetheremissionoratleastthe lowRAactivity.If notachievedwithsyntheticDMARDsthe
biologicDMARDsshouldalsobeincluded.Besidesthe afore-mentioned therapy, non-steroidal anti-inflammatory drugs (NSAIDs)shouldbeincluded,togetherwithcorticosteroidsif needed, inorder tocontrolthe painand theinflammation andimproveRApatient’sgeneralhealthcondition.Duringthe administrationoftheabovementionedtherapy,itis neces-sarytoprotectthedigestivetractbleedingwithproton-pump inhibitors (PPI), especially in patients with high gastroin-testinalbleedingrisk.Inaddition,regularhematologicaland biochemicallaboratoryresultsfollowupsareneededinorder tomonitorapossiblemarrowbonedamageandhepatotoxicity duringtheDMARDsadministration.4,5
overwhelming,sustainedsenseofexhaustionanddecreased capacity for physicaland mental work”.6 The RApatients
definetheirfatigueaspersistent,multidimensionalsymptom withsevere,longtermconsequencestotheirdailylife7–9 or
asasymptomthatdisruptstheirdailyactivitiesandcauses anon-refreshingsleep.10Severalstudieshaveshownthatthe
highfatigueinRApatientswasrelatedtothepain,depression symptoms, sleepdisorder, high physicaleffort,genderand psychosocialfactors.11,12Otherreportsfoundthatdepression
isrelatedtothepain,fatigue,inabilitytoworkandlower ther-apycompliance.13,14Somestudiesreportahighincidenceofa
commondepressionandanxietyappearanceinRApatients.15
However,thereisalackofreportsintheliteratureabout com-moninfluencesofthebasic,adjuvantandsupplementalRA therapyandsocioeconomicfactorstotheanxiety,depression andfatigueinRApatients.
Study
goals
Theprimarygoalofthestudywastoevaluatetheinfluence ofthebasicRAtherapy,theadjuvantandsupplemental ther-apy,thedemographicandsocioeconomiccharacteristics,the RAcomplicationsand comorbiditiestotheanxiety, depres-sionandfatigueinRApatients.Thesecondaryobjectivewas toevaluatetherelationshipbetweenthedepressionandthe fatigueandanxietyofRApatients.
Methodology
Studylocationandtimeperiod
The study was conducted during the time period from April–August2014andincludedtheRApatientsfrom20 Ser-bianprimaryhealthcareinstitutions,onetertiaryhealthcare institution–InstituteofRheumatology,ClinicalCentreof Ser-bia, Belgrade, Serbia, and also two specialized health spa institutions–NiˇskaBanja,Niˇs,SerbiaandJodnaBanja,Novi Sad,Serbia.
Studydesign
Amulticenterepidemiologiccross-sectionalstudyinthe pop-ulationofolderRApatientswasconducted.Thecrosssection wasmadeaccordingtotheobtainedself-reportedoutcome categoriesofhighfatigueabsence/presence,highdepression absence/presenceandhighanxietyabsence/presence.
Patientsandprocedures
Thepatientsofbothgenderssufferingfrom RAolder than 18yearswereincluded.Thecriterionforexcludingpatients fromthestudywasatleastonemissinganswerinthefatigue, depressionoranxietyquestionnaires.
During onevisit tothe doctor the patients filled inthe surveythatcontainedquestionsgroupedintothreesections. Firstsectioncontainedquestionsrelatedtodemographicand socioeconomiccharacteristicsofthepatients.Thesecondone referredtothedurationofthedisease,typeanddurationof
the current RA therapy, aswell as the RAtreatment com-plications. Inthethirdsection therewere threemeasuring instrumentsofself-reportedhealthconditionofthepatient: “Fatigue Assessment Scale” (FAS) with 10 items; “Patient Health Questionnaire” (PHQ-9) with9 items,and “General-izedAnxietyDisorder”(GAD-7)with7items.Patientsneeded approximately30mintofilloutallthequestionnaires.
Variablesinthestudy
Theresultingvariables inthe studywere PHQ-9score,FAS scoreandGAD-7score.ThevaluesofFASscore≥22were con-sideredasahighfatigue.16HighanxietywasdefinedasGAD-7
score≥10,17,18whilethehighdepressionwasdefinedbythe
valuesofPHQ-9score≥10.19TheGAD-7andPHQ-9surveys
containthequestionswithprovidedanswersaboutthe pres-ence ofthe problem thatcaused dificultiestothe patients duringthe previoustwoweeks,and whichwere numbered byascendingLikertordinalscalefrom0to3(0–notatall;1 –fewdays;2–morethanahalfofthetimeand3–almost everyday).ThePHQ-9surveyisusedtoevaluatethelevelof depression,20,21whiletheGAD-7wasprimarlydevelopedto
evaluatethegeneralizedanxietydisorder.17TheFAScontains
ten questionsthatdescribethe presenceofpossible condi-tionswithfiveprovidedordinalanswermodalitiesfrom1to5 (1–never;2–sometimes;3–ordinarily;4–often;5–always). TheresultingFASscorerangesfrom10to50.TheFASsurvey wasprimarlydesignedasaninstrumenttoevaluateand mon-itorthefatigueinthegeneralpatientpopulation,22andithas
alsobeenvalidatedasareliablemasuringfatigueinstrument inthesarcoidosispatients.23
Theexamineddemographicandsocioeconomicvariables were: age, gender, marriage status, professional qualifica-tions,employmentstatus,occupation,theneedforanother person’s assistance, the need for frequent taxi use, phys-ioterapist payment, assisitance device use due to RA, the presenceofotherdiseases,osteoporosispresence,orthopedic surgicalinterventionandfracturedlimbscausedbytheRA. Theincludedtreatmentpredictorswere:currentRAtherapy status, current RAtherapy duration (months), periodfrom the beginning of the first RA symptoms until the start of the current therapy (months), proton-pump inhibitor and H2receptorantagonist useinordertoprotectthestomach, the use of supplements that contain glucosamine sulfat, chondroitin sulfat, hyaluronic acid, antirheumatic cream use, vitaminD3 and calcium consummation, self-initiative therapy cessation, stomach or duodenum bleeding during RA therapy, surgery performed because of the stomach or duodenum bleeding,aswell astheuse ofalternativeways of treatments. Thecurrent RAtherapy is defined bythree modalitiessuchas:(1)NSAIDsand/oranalgesicsand/or cor-ticosteroids;(2) syntheticDMARDsaloneor combinedwith corticosteroidsand/orNSAIDand(3)anyRAtreatmentwhich includes biologic DMARDs. There were also data recorded about the duration of the RA (months) as well as disease symptomsduration(months).
Statisticaldataprocessing
normaldistributionwasperformed.Inthedatawitha nor-maldistribution,thecontinous variablesaredescribedbya mean and a standard deviation, while the data that devi-atefromnormaldistribiutionaredescribedbyamedianand aninterquartile range. Thenominal variables are descibed by frequencyand percentage according to the appropriate categories.Inthe methodsofinferentialstatistics,the cor-relationof individual category predictors with each ofthe monitoredself-reportedoutcomes (absence/presenceofthe highfatigue,anxietyordepressionlevel)wasevaluatedbyPhi orCarmer’sVcorrelationcoefficient.Differenceevaluationin thecontinousnumericalvariablesbetweenthegroupwiththe presenceandthegroupwiththeabsenceofthetested self-reportedoutcomes,wasdonebyMann–Whitneymethod.The riskfactoranalysisforeachoftheself-reportedoutcomeswas donebythebinarylogisticregressionmethod.Theassessment oftherelationshipbetweenthelevelofdepressionwiththe fatigueandanxietylevelswasperformedbythemultiple lin-earregression(stepwisemethod).Thediagnosisofcollinearity betweenthe predictors inthe linear regression modelwas donebythearbitraryassesmentoftheconditionalindexand thevarianceinflationfactor(VIF).24,25Theabsenceofadoubt
intheexistanceofthecollinearitywasdefinedbyaconditional indexlessthan15 andVIFvaluelessthan 3.Theaccepted levelofsignificancewas0.05.Thestatisticalanalysiswas con-ductedusingIBMSPSSStatistics20.Thisstudywasapproved bytheinstitution’s institutionalreviewboardand obtained patients’consent.
Results
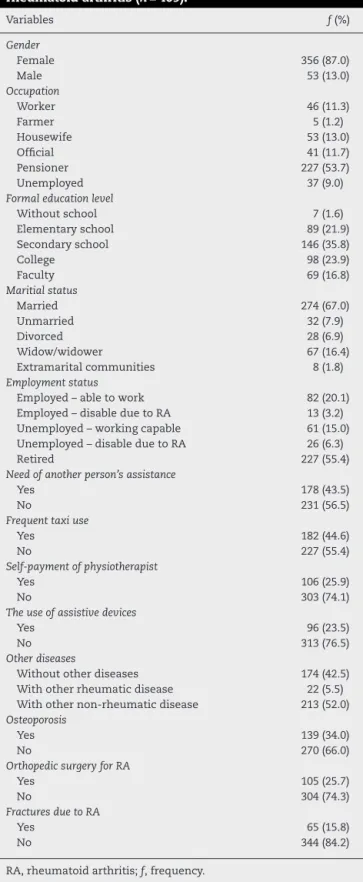
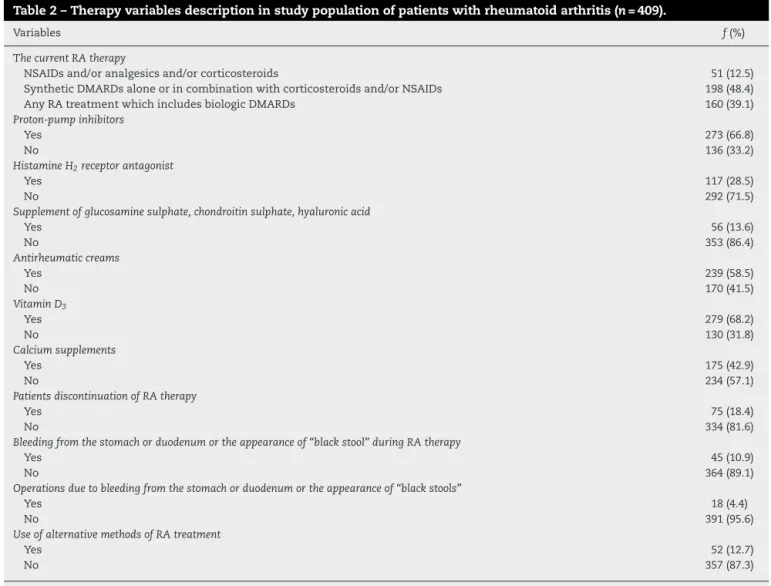
Outof494patients,409ofthemhavefulfilledtheinclusion studycriteria.Themeanageofthepatientswas58.03±12.16 years.The RA duration median was 144 monthswith the interquartilerangefrom84to288months,whilethe symp-tomsdurationmedian(pain,limitedmobility)causedbythe RAwas159.5monthswiththeinterquartilerangefrom 107 to240months.Durationmedianofthecurrent RAtherapy was60monthswiththeinterquartilerangefrom24 to108 months. The median of the time passed from the begin-ningofthesymptomscausedbytheRAuntilallcurrentRA therapiesstartwas68.5monthswiththeinterquartilerange from 24 to164 months,namely: (1) untilthe therapy with NSAIDsand/oranalgesicsand/orcorticosteroids(median=48 months;interquartilerangefrom13to201months);(2)until the therapy with synthetic DMARDs alone or in combina-tionwithcorticosteroidsand/orNSAIDs(median=49months; interquartilerangefrom12to151months);(3)anyRA treat-mentwhichincludesbiologicDMARDs(median=99months; interquartilerangefrom46to166months).Theaveragevalue oftheFASscorewas27.31±8.81.ThemeanvalueofthePHQ-9 scorewas10.13±7.00andoftheGAD-7scorewas8.21±6.11. Descriptionofdemographicandsocioeconomicvariables ispresentedinTable1.InTable2thecategoriesofthetherapy variablesweredescribed.
Onehundredandninetyseven(48.14%)patientshadthe PHQ-9score≥10.ThesamenumberalsohadtheFASscore
≥22,while148(36.19%)patientshadtheGAD-7score≥10.The descriptivestatisticsforthedurationofthedisease,difficulties
Table1–Descriptionofdemographicandsocioeconomic variablesinstudypopulationofpatientswith
rheumatoidarthritis(n=409).
Variables f(%)
Gender
Female 356(87.0)
Male 53(13.0)
Occupation
Worker 46(11.3)
Farmer 5(1.2)
Housewife 53(13.0)
Official 41(11.7)
Pensioner 227(53.7)
Unemployed 37(9.0)
Formaleducationlevel
Withoutschool 7(1.6)
Elementaryschool 89(21.9)
Secondaryschool 146(35.8)
College 98(23.9)
Faculty 69(16.8)
Maritialstatus
Married 274(67.0)
Unmarried 32(7.9)
Divorced 28(6.9)
Widow/widower 67(16.4)
Extramaritalcommunities 8(1.8)
Employmentstatus
Employed–abletowork 82(20.1)
Employed–disableduetoRA 13(3.2)
Unemployed–workingcapable 61(15.0)
Unemployed–disableduetoRA 26(6.3)
Retired 227(55.4)
Needofanotherperson’sassistance
Yes 178(43.5)
No 231(56.5)
Frequenttaxiuse
Yes 182(44.6)
No 227(55.4)
Self-paymentofphysiotherapist
Yes 106(25.9)
No 303(74.1)
Theuseofassistivedevices
Yes 96(23.5)
No 313(76.5)
Otherdiseases
Withoutotherdiseases 174(42.5)
Withotherrheumaticdisease 22(5.5)
Withothernon-rheumaticdisease 213(52.0) Osteoporosis
Yes 139(34.0)
No 270(66.0)
OrthopedicsurgeryforRA
Yes 105(25.7)
No 304(74.3)
FracturesduetoRA
Yes 65(15.8)
No 344(84.2)
RA,rheumatoidarthritis;f,frequency.
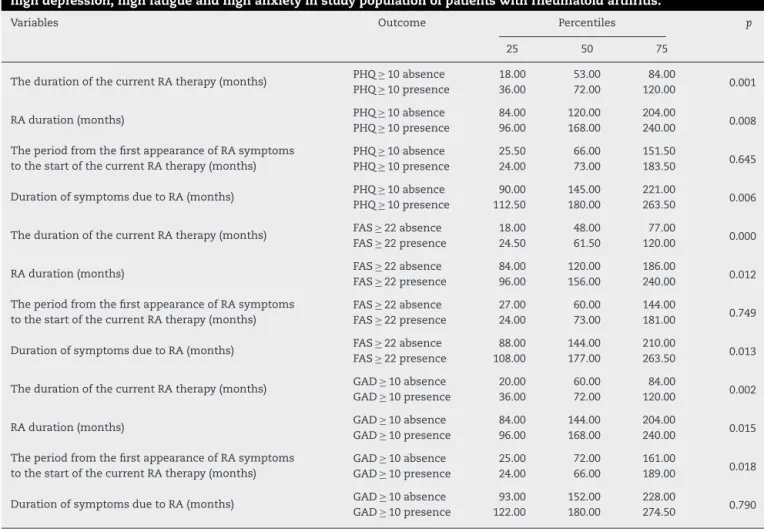
duration,currenttherapyandtheperiodfromthebeginning
ofthesymptomsuntilthecurrentRAtherapystartwiththe
levelofdifferencesignificancebetweenthegroupsofpatients
withtheabsenceandthegroupofpatientswiththepresence
ofhighdepression,anxietyandthehighfatiguearepresented
Table2–Therapyvariablesdescriptioninstudypopulationofpatientswithrheumatoidarthritis(n=409).
Variables f(%)
ThecurrentRAtherapy
NSAIDsand/oranalgesicsand/orcorticosteroids 51(12.5)
SyntheticDMARDsaloneorincombinationwithcorticosteroidsand/orNSAIDs 198(48.4)
AnyRAtreatmentwhichincludesbiologicDMARDs 160(39.1)
Proton-pumpinhibitors
Yes 273(66.8)
No 136(33.2)
HistamineH2receptorantagonist
Yes 117(28.5)
No 292(71.5)
Supplementofglucosaminesulphate,chondroitinsulphate,hyaluronicacid
Yes 56(13.6)
No 353(86.4)
Antirheumaticcreams
Yes 239(58.5)
No 170(41.5)
VitaminD3
Yes 279(68.2)
No 130(31.8)
Calciumsupplements
Yes 175(42.9)
No 234(57.1)
PatientsdiscontinuationofRAtherapy
Yes 75(18.4)
No 334(81.6)
Bleedingfromthestomachorduodenumortheappearanceof“blackstool”duringRAtherapy
Yes 45(10.9)
No 364(89.1)
Operationsduetobleedingfromthestomachorduodenumortheappearanceof“blackstools”
Yes 18(4.4)
No 391(95.6)
UseofalternativemethodsofRAtreatment
Yes 52(12.7)
No 357(87.3)
RA,rheumatoidarthritis;NSAIDs,non-steroidalanti-inflammatorydrugs;DMARDs,disease-modifyingantirheumaticdrugs;f,frequency.
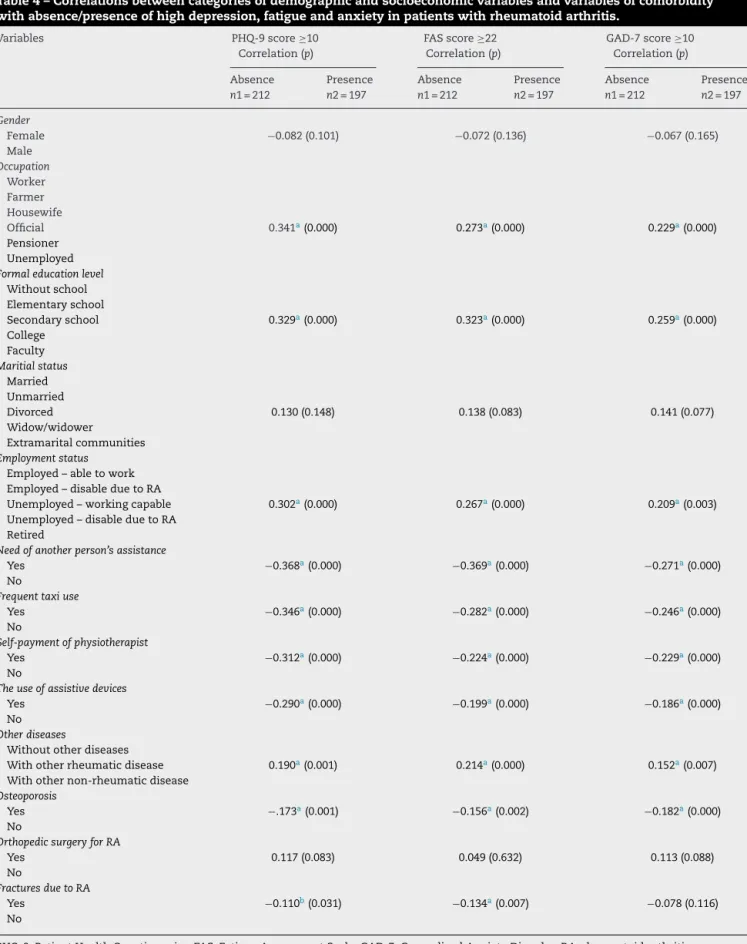
ItwasestimatedthatthePHQ-9score,theFASscoreand
theGAD-7scorecategoryvariablesstatisticallysignificantly
correlatewiththe majorityofsocioeconomicvariables and
comorbidity, except for gender, marital status and
ortho-pedic intervention (Table 4). In addition, the GAD-7 score
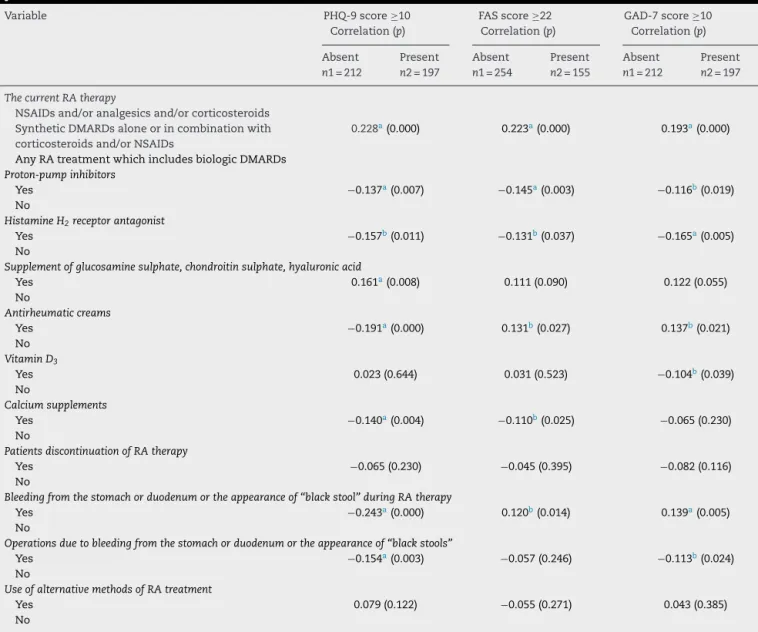
categoryvariablehasnotshownacorrelationwithbone frac-ture.Also,itwasnoticedthatthePHQ-9score,theFASscore and the GAD score statisticallysignificantly correlate with mostofthe therapy variables,exceptforthe self-initiative discontinuationoftheRAtherapyandthealternative ther-apyuse(Table5).Aditionally,the PHQ-9scoreandthe FAS scorehavenotshownasignificantcorrelationwiththe vita-mine D3 therapy, while the FAS score has not correlated withtheantirheumaticcreamuseandwiththeoperationin gastrointestinal tract causedby bleeding.The GAD-7score categoryvariable also hasnot showna significant correla-tionwiththeantirheumaticcreamuse,aswellasthecalcium therapy.
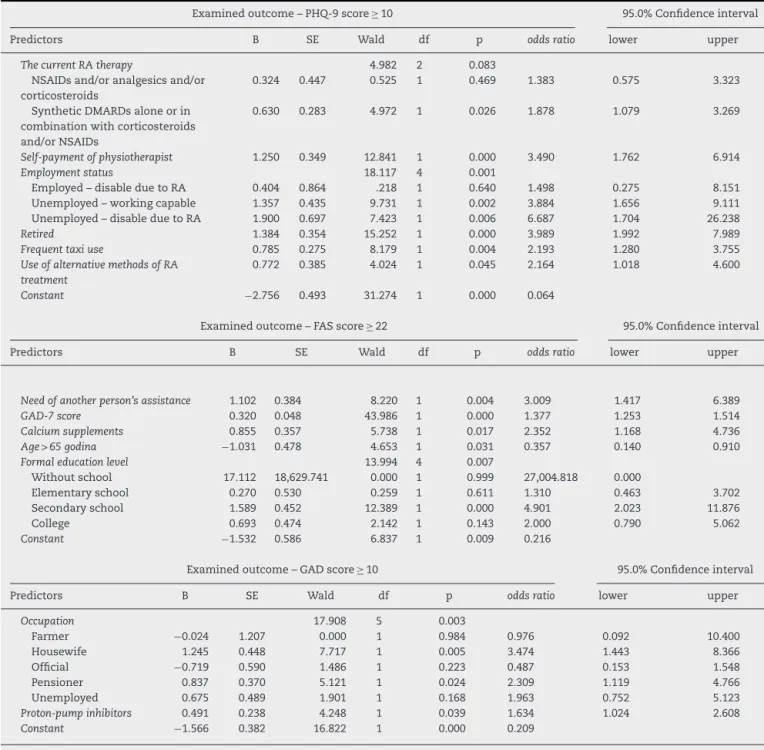
Bythelogisticregressionmodelitwasdemonstratedthat thehighdepressionwasrelatedtofiveindependent predic-tors(Table6).Thesignificantpredictorofthehighdepression wasthesyntheticDMARDstherapyaloneorcombinedwith the corticosteroids and/or NSAIDs. The sociodemographic
predictors of the PHQ-9 score ≥10 were physiotherapist self-payment, frequent taxi use, alternative treatment and employmentstatus.Twocategoriesoftheemployment sta-tushaveshowntobesignificantpredictorsofthePHQ-9score
≥10.Those arethe categoryofunemployed but capableto work,andthecategoryofunemployedasadisabledperson duetotheRA.Thankstothementionedpredictorsthe70.2%of thetotalvariabilityofthedependentvariablewasexplained, so thevariability ofthe presenceofthehigh depressionis explainedby75.5%,whilethevariabilityoftheabsenceofthe highdepressionisexplainedby65.3%.
Table3–Descriptivestatisticsforthedurationofthediseaseandsymptomsandcurrenttherapydurationfromthe appearanceofsymptomstothestartofcurrenttherapyofrheumatoidarthritisaccordingtotheabsence/presenceof highdepression,highfatigueandhighanxietyinstudypopulationofpatientswithrheumatoidarthritis.
Variables Outcome Percentiles p
25 50 75
ThedurationofthecurrentRAtherapy(months) PHQ ≥ 10absence 18.00 53.00 84.00 0.001 PHQ ≥ 10presence 36.00 72.00 120.00
RAduration(months) PHQ ≥ 10absence 84.00 120.00 204.00 0.008
PHQ ≥ 10presence 96.00 168.00 240.00
TheperiodfromthefirstappearanceofRAsymptoms tothestartofthecurrentRAtherapy(months)
PHQ ≥ 10absence 25.50 66.00 151.50
0.645 PHQ ≥ 10presence 24.00 73.00 183.50
DurationofsymptomsduetoRA(months) PHQ ≥ 10absence 90.00 145.00 221.00 0.006
PHQ ≥ 10presence 112.50 180.00 263.50
ThedurationofthecurrentRAtherapy(months) FAS≥ 22absence 18.00 48.00 77.00 0.000
FAS≥ 22presence 24.50 61.50 120.00
RAduration(months) FASFAS≥ 22absence 84.00 120.00 186.00 0.012
≥ 22presence 96.00 156.00 240.00
TheperiodfromthefirstappearanceofRAsymptoms tothestartofthecurrentRAtherapy(months)
FAS≥ 22absence 27.00 60.00 144.00
0.749
FAS≥ 22presence 24.00 73.00 181.00
DurationofsymptomsduetoRA(months) FAS≥ 22absence 88.00 144.00 210.00 0.013
FAS≥ 22presence 108.00 177.00 263.50
ThedurationofthecurrentRAtherapy(months) GAD ≥ 10absence 20.00 60.00 84.00 0.002 GAD ≥ 10presence 36.00 72.00 120.00
RAduration(months) GAD ≥ 10absence 84.00 144.00 204.00 0.015
GAD ≥ 10presence 96.00 168.00 240.00
TheperiodfromthefirstappearanceofRAsymptoms tothestartofthecurrentRAtherapy(months)
GAD ≥ 10absence 25.00 72.00 161.00
0.018 GAD ≥ 10presence 24.00 66.00 189.00
DurationofsymptomsduetoRA(months) GAD ≥ 10absence 93.00 152.00 228.00 0.790
GAD ≥ 10presence 122.00 180.00 274.50
PHQ-9,PatientHealthQuestionnaire;FAS,FatigueAssessmentScale;GAD-7,GeneralizedAnxietyDisorder;RA,rheumatoidarhtritis.
Thesignificantpredictorofthehighanxietyinthelogistic
regression model were proton pump inhibitor
gastropro-tection and two occupation categories – housewife and
pensioner(Table6)andthesepredictorsexplained64.8%of
totalpensionerofthedependentvariable.Thevariabilityof thepresenceofthehighanxietywasexplainedwith13.5%, while the explained pensioner of absence of the severe anxietywas93.9%.
Thelinearregressionmodelresultedinthestatistically sig-nificantcorrelationofthePHQ-9scorewiththeGAD-7and the FASscores. That waspresentedbythe equation: PHQ-9score=−3.47+0.634×GAD-7score+0.323×FASscore.The multiplelinearregressionmodelstatisticsforthepredictors were:(1)fortheconstant(t=−0.784;p=0.000);(2)forthe GAD-7score(t=0.548;p=0.000)and(3)fortheFASscore(t=0.402; p=0.000).Thedeterminationcoefficient(R2)forthementioned linearmodelwas0.788.Therewasastatisticallysignificant changeoftheR2forthementionedlinearregressionmodel withtheFASscoreandGAD-7scorepredictorsforPHQ-9score incomparissonwithmodelthatcontainsonlytheGAD-7score (Fchanges=124.979;df1=1;df2=408;p=0.000).TheR2ofthe modelthatcontainedtheGAD-7score,astheonlypredictor ofthePHQ-9was0.716.Thebiggestconditionalindexinthe
linearregressionmodelwithtwopredictorswas10.021.The VIFvaluesinbothpredictorswereidenticalandwere2.221.
Discussion
Accordingtothesocialsignaltransductiontheoryof depres-sion,the lowsocioeconomicstatusimpliesthehigh riskof socialconflicts,socialisolation,excludingorrejectinga per-son,andalsorepresentsoneofthemostimportantprovoking factorsorbigstressfullifeeventsthatcausethemajor depres-sionand stimulationofinflammation.26 InRApatientsthe
interpersonal lossand the socialisolation are the key fac-torsthatcanleadtothediseaseexacerbationcausedbythe inflammationortotheadditionaldepressionsymptoms exac-erbationandtheappearanceofthemajordepression.27Our
Table4–Correlationsbetweencategoriesofdemographicandsocioeconomicvariablesandvariablesofcomorbidity withabsence/presenceofhighdepression,fatigueandanxietyinpatientswithrheumatoidarthritis.
Variables PHQ-9score≥10
Correlation(p)
FASscore≥22 Correlation(p)
GAD-7score≥10 Correlation(p)
Absence n1=212
Presence n2=197
Absence n1=212
Presence n2=197
Absence n1=212
Presence n2=197
Gender
Female −0.082(0.101) −0.072(0.136) −0.067(0.165)
Male Occupation
Worker Farmer Housewife
Official 0.341a(0.000) 0.273a(0.000) 0.229a(0.000)
Pensioner Unemployed
Formaleducationlevel
Withoutschool Elementaryschool
Secondaryschool 0.329a(0.000) 0.323a(0.000) 0.259a(0.000)
College Faculty
Maritialstatus
Married Unmarried
Divorced 0.130(0.148) 0.138(0.083) 0.141(0.077)
Widow/widower
Extramaritalcommunities
Employmentstatus
Employed–abletowork Employed–disableduetoRA
Unemployed–workingcapable 0.302a(0.000) 0.267a(0.000) 0.209a(0.003)
Unemployed–disableduetoRA Retired
Needofanotherperson’sassistance
Yes −0.368a(0.000) −0.369a(0.000) −0.271a(0.000)
No
Frequenttaxiuse
Yes −0.346a(0.000) −0.282a(0.000) −0.246a(0.000)
No
Self-paymentofphysiotherapist
Yes −0.312a(0.000) −0.224a(0.000) −0.229a(0.000)
No
Theuseofassistivedevices
Yes −0.290a(0.000) −0.199a(0.000) −0.186a(0.000)
No
Otherdiseases
Withoutotherdiseases
Withotherrheumaticdisease 0.190a(0.001) 0.214a(0.000) 0.152a(0.007)
Withothernon-rheumaticdisease
Osteoporosis
Yes −.173a(0.001) −0.156a(0.002) −0.182a(0.000)
No
OrthopedicsurgeryforRA
Yes 0.117(0.083) 0.049(0.632) 0.113(0.088)
No
FracturesduetoRA
Yes −0.110b(0.031) −0.134a(0.007) −0.078(0.116)
No
PHQ-9,PatientHealthQuestionnaire;FAS,FatigueAssessmentScale;GAD-7,GeneralizedAnxietyDisorder;RA,rheumatoidarthritis.
a Levelofstatisticalsignificanceforp≤0.01.
Table5–Correlationsbetweencategoriesoftherapywithabsence/presenceofhighdepression,fatigueandanxietyin patientswithrheumatoidarthritis.
Variable PHQ-9score≥10
Correlation(p)
FASscore≥22 Correlation(p)
GAD-7score≥10 Correlation(p)
Absent n1=212
Present n2=197
Absent n1=254
Present n2=155
Absent n1=212
Present n2=197
ThecurrentRAtherapy
NSAIDsand/oranalgesicsand/orcorticosteroids SyntheticDMARDsaloneorincombinationwith corticosteroidsand/orNSAIDs
0.228a(0.000) 0.223a(0.000) 0.193a(0.000)
AnyRAtreatmentwhichincludesbiologicDMARDs
Proton-pumpinhibitors
Yes −0.137a(0.007) −0.145a(0.003) −0.116b(0.019)
No
HistamineH2receptorantagonist
Yes −0.157b(0.011) −0.131b(0.037) −0.165a(0.005)
No
Supplementofglucosaminesulphate,chondroitinsulphate,hyaluronicacid
Yes 0.161a(0.008) 0.111(0.090) 0.122(0.055)
No
Antirheumaticcreams
Yes −0.191a(0.000) 0.131b(0.027) 0.137b(0.021)
No
VitaminD3
Yes 0.023(0.644) 0.031(0.523) −0.104b(0.039)
No
Calciumsupplements
Yes −0.140a(0.004) −0.110b(0.025) −0.065(0.230)
No
PatientsdiscontinuationofRAtherapy
Yes −0.065(0.230) −0.045(0.395) −0.082(0.116)
No
Bleedingfromthestomachorduodenumortheappearanceof“blackstool”duringRAtherapy
Yes −0.243a(0.000) 0.120b(0.014) 0.139a(0.005)
No
Operationsduetobleedingfromthestomachorduodenumortheappearanceof“blackstools”
Yes −0.154a(0.003) −0.057(0.246) −0.113b(0.024)
No
UseofalternativemethodsofRAtreatment
Yes 0.079(0.122) −0.055(0.271) 0.043(0.385)
No
PHQ-9,PatientHealthQuestionnaire;FAS,FatigueAssessmentScale;GAD-7,GeneralizedAnxietyDisorder;RA,rheumatoidarthritis;NSAIDs, non-steroidalanti-inflammatorydrugs;DMARDs,disease-modifyingantirheumaticdrugs.
a Levelofstatisticalsignificanceforp≤0.01.
b Levelofstatisticalsignificanceforp≤0.05.
socialrejection,isolationand interpersonallossduetothe disability.Otherauthorsalsofoundthatthebad socioecono-micstatusincreasesthedepressionsymptomsmeasuredby PHQ-9surveyinRApatients.28Löweetal.demonstratedthat
thedepressionisasignificantpredictoroftheworking inca-pabilityoftheRApatients.29 Inourstudy,othersignificant
socioeconomicpredictors ofthehighdepressionwere: pen-sionerstatus,unemploymentoftheworkingcapablepatients, frequenttaxiuse,self-paymentofphysiotherapistand self-paymentofalternativetreatment.Thelastmentionedfactors alsoimplyabadsocioeconomicRApatients’statusduetothe lackofthe incomeorinsufficientpersonalincome,aswell astheiradditionalfinancialexhaustionbytheexpensesthey haveontheirownduringthedailyactivities,implementation ofphysiotherapymeasurementsorthealternativetreatment or someother activities requiredatthe rehabilitaion, pain
reliefandtheimprovementofthesocialfunctioningin gen-eral.
Wealsoshowedthat,ingeneral,theRAtherapyhasno influence on the appearance ofthe high depression inRA patients,butthereisasignificantinfluenceofthesynthetic DMARDtherapycategoryaloneorcombinedwith corticoste-roidsor/andNSAID.Inourstudypopulationpatientswiththe aforementionedtreatmentmodalitywere80%morelikelyto haveahighdepression,whichpotentiallyindicatesahigher RAactivity inthese patients.Itwasdemonstratedinsome longitudinalstudiesthatpersistentdepression/anxiety symp-tomspredictpoortreatmentresponsewhichcorrespondswith increasedRAactivityovertime.30Inaunivariateanalysisof
Table6–Logisticregressionmodelsparametersaccordingtosociodemographic,socioeconomicandtherapeutic predictorsofhighdepression,fatigueandanxietyinpatientswithrheumatoidarthritis.
Examinedoutcome–PHQ-9score ≥ 10 95.0%Confidenceinterval
Predictors B SE Wald df p oddsratio lower upper
ThecurrentRAtherapy 4.982 2 0.083
NSAIDsand/oranalgesicsand/or corticosteroids
0.324 0.447 0.525 1 0.469 1.383 0.575 3.323
SyntheticDMARDsaloneorin combinationwithcorticosteroids and/orNSAIDs
0.630 0.283 4.972 1 0.026 1.878 1.079 3.269
Self-paymentofphysiotherapist 1.250 0.349 12.841 1 0.000 3.490 1.762 6.914
Employmentstatus 18.117 4 0.001
Employed–disableduetoRA 0.404 0.864 .218 1 0.640 1.498 0.275 8.151
Unemployed–workingcapable 1.357 0.435 9.731 1 0.002 3.884 1.656 9.111
Unemployed–disableduetoRA 1.900 0.697 7.423 1 0.006 6.687 1.704 26.238
Retired 1.384 0.354 15.252 1 0.000 3.989 1.992 7.989
Frequenttaxiuse 0.785 0.275 8.179 1 0.004 2.193 1.280 3.755
UseofalternativemethodsofRA treatment
0.772 0.385 4.024 1 0.045 2.164 1.018 4.600
Constant −2.756 0.493 31.274 1 0.000 0.064
Examinedoutcome–FASscore≥ 22 95.0%Confidenceinterval
Predictors B SE Wald df p oddsratio lower upper
Needofanotherperson’sassistance 1.102 0.384 8.220 1 0.004 3.009 1.417 6.389
GAD-7score 0.320 0.048 43.986 1 0.000 1.377 1.253 1.514
Calciumsupplements 0.855 0.357 5.738 1 0.017 2.352 1.168 4.736
Age>65godina −1.031 0.478 4.653 1 0.031 0.357 0.140 0.910
Formaleducationlevel 13.994 4 0.007
Withoutschool 17.112 18,629.741 0.000 1 0.999 27,004.818 0.000
Elementaryschool 0.270 0.530 0.259 1 0.611 1.310 0.463 3.702
Secondaryschool 1.589 0.452 12.389 1 0.000 4.901 2.023 11.876
College 0.693 0.474 2.142 1 0.143 2.000 0.790 5.062
Constant −1.532 0.586 6.837 1 0.009 0.216
Examinedoutcome–GADscore≥ 10 95.0%Confidenceinterval
Predictors B SE Wald df p oddsratio lower upper
Occupation 17.908 5 0.003
Farmer −0.024 1.207 0.000 1 0.984 0.976 0.092 10.400
Housewife 1.245 0.448 7.717 1 0.005 3.474 1.443 8.366
Official −0.719 0.590 1.486 1 0.223 0.487 0.153 1.548
Pensioner 0.837 0.370 5.121 1 0.024 2.309 1.119 4.766
Unemployed 0.675 0.489 1.901 1 0.168 1.963 0.752 5.123
Proton-pumpinhibitors 0.491 0.238 4.248 1 0.039 1.634 1.024 2.608
Constant −1.566 0.382 16.822 1 0.000 0.209
PHQ-9,PatientHealthQuestionnaire;FAS,FatigueAssessmentScale;GAD-7,GeneralizedAnxietyDisorder;RA,rheumatoidarthritis;NSAIDs, non-steroidalanti-inflammatorydrugs;DMARDs,disease-modifyingantirheumaticdrugs.
frequency.31However,inotherreportstherewasnoRA
ther-apyinfluenceontheself-reportedhighdepressionfrequency intheRApatients.32Bothbeforeandduringthestudyperiod
thecurrentbiologicdrugsprovidedbythehealthinsurance ofRepublicofSerbia,thatwereavailabletotheRApatients are humanproteindrugs thatneutralize pro-inflammatory effectsoftumornecrosisfactorandinterleukin-6.Theabove mentioned biologic drug combined with methotrexate is prescribedtotheRApatientswhosediseaseisstillclinically active(i.e.whoseDiseaseActivityScoreisabove5.1)despite theimplementationofmethotrexate(atleast15mgonce a
experience of disforia, hopelessness and uselessness, can alsobeoneofthe contextual,psychosocialtriggersforthe appearence of major depression and poor RA treatment response.
We also found that the RA therapy (Table 6) does not increasetheriskofthehighfatigueordepression,aswellas that the high fatigueand anxiety, completely independent onefromanother,leadtothehighleveloftheself-reported depressionsymptoms.Ontheotherhand,theresultsimply that the increase of the anxiety level also increases the risk of the high fatigue appearance. These are important factssincethereisnospecificpharmacotherapyofthehigh fatigue.Withalltheabovementioned,wehighlightthatthe specific medicamentous therapy should be implemented withantidepressantsthathaveastronganxiolyticeffect(for examplewithselectiveserotoninreuptakeinhibitors),bothin ordertoreducethedepressionsymptomsandtopotentially decreasethehighfatigueoftheRApatients.
Inourstudytheageabove65yearshadaprotectiveeffect ontheappearanceofthehighfatigueinRApatients.Thiskind offindingcoexistswiththefindingsofWattetal.,whoshowed that,dependingontheage,fatigueinthegeneralpopulation hasanon-lineartrend.33Inthegeneralpopulationaglobal
fatigueevaluationaftertheageof65wasdecreasingbecause ofthementalandcognitivefatiguecomponentdecrease. How-ever,thestudiesintheRApatientspopulationsdidnotshow anychangesinthefatiguelevelwiththechangeofage.34
Wealsodemonstratedthatcalciumsuplementation ther-apy for prophylaxis or therapy of osteoporosis in the RA patientscansignificantlyincreasetheriskofthehighfatigue appearance.This potentially suggests thatcalcium supple-ments therapy in our patients was administered without adequatemonitoringofserumionizedcalcium.Fatigueisvery commonsymptomofhypercalcemia.35Oelzneretal.reported
thatabout30%oftheRApatientshavehypercalcemia(high levelsofserum ionizedcalcium) thatoccurs inassociation withthe highdisease activity,suppressedparathyroid hor-monesecretion,suppressedvitaminDhormonesynthesisand bonemineraldensityreduction.36
From socioeconomicfactors the importantpredictors of thehighfatigueintheRApatientsweretheneedforother peo-ple’shelpandcare,aswellastheleveloftheformaleducation thatisdefinedasfinishedcollegeeducation.InSerbiaformal educationtoobtainacollegedegreelastsfor12years. Castre-jonetal.foundthattheRApatientswithaformaleducation lastinglessthanorexactly12yearshadthebiggerfatigue com-paredtothepatientswithformaleducationthatlastedmore than 12years.37 Theneed forother people’shelpand care
impliessomeseveresetbackandtheseRApatients’problemin performingdailyactivities.Inotherstudiesitwasshownthat therestrictionofdailyactivitiescorrelatespositivelywiththe fatigue,andthattheincreaseofthedailyactivitiescorrelates negativelywiththefatigue.38,39
Whenitcomestothesocioeconomicpredictorsofthehigh anxietyinourstudypopulation,the significantriskfactors weretwocategoriesofoccupation–pensionerandhousewife (Table6).Itisdescribedintheliteraturethatthehousewives withthemilderRAweremoreanxiouseventhoughtheyhad theirspouse’sunderstandingfortheirdisease.40Patientswith
thespecificoccupationcategorieswhosesociallifeismostly
spentinthehouseormostlyrelatedtothehouseand fam-ilysurroundings canpossiblyexperience moreanxietythat isinversely relatedtothe RAseverityand theexperienced understandingbythepersonswithwhomtheylive.
Additionally,theriskfactorofthehighanxietyappearance was alsoastomachbleedingpreventionbythe PPI.In Ser-bia,unlikethedrugsfromtheH2antagonistgroupwhichare cheap,theRApatientshavetopayforthePPIgastroprotecive therapybythemselvesswhichisveryexpensiveforthem.The fearwhether andhowlong theywillbeabletopayforthe PPI,forthegastroprotectioncanalsobeariskfactorofthe highRApatients’anxiety.Therestofthesocioeconomicand therapypredictorsinthisstudy(Tables4and5)haveshown, inspiteoftheachievedstatisticalsignificance,aweak corre-lationwiththeself-reportedoutcomesofthepatients.These predictorsshareasmallmutualvarianceofallthreeoutcomes (depression,fatigueandanxiety),whichimpliesthattheyare notspecificforanyofthem.
The limitations of our study primarily originate from its design. A cross sectional study designdoes not evalu-atethespecificsofthequestionedpredictors’influenceson theappearanceofthefatigue,depressionandanxetyinRA patients, comparedto thepatient populationwith another inflammatory or non-inflammatory disease. In our study, theRAactivitywasnotmonitoredandthereforewecannot excludecertainbiasinourexplanationsoftherelationship betweentheappearanceofthehighdepressionandtreatment responses.Sincewehavenotmonitoredthestatusofcalcemia and/orRAactivity,therealsomaybesomebiasinour explana-tionofthelinkbetweenthehighfatigueandcalciumtherapy. Eventhoughwehadalargepatientspopulationinthestudy, themalepopulationresponsenumberwasunusuallysmall. Consequently,comparedtothefemalepopulation,observed riskfactorsoftheappearanceofthequestionedself-reported outcomesthatcomefromthemalepopulationarepotentially lessanalyzed.Also,inourRApatientpopulationwehaven’t recordedanydataabouttheuseofantidepressant,sedative and/oranxiolyticdrugs.
Conclusion
Demographic,socioeconomicandpsychosocialfactors,along with contextualand treatment factors, canlargely explain the appearanceofthe high levelofdepression andfatigue andhighanxietyinrheumatoidarthritispatients.The evalua-tionofthepsychosocial,socioeconomicandtherapyimpacts, along withtherheumatoidarthritisactivity and inflamma-tionontheappearanceofthehighdepression,highfatigue andhighanxietycanbeofgreatimportanceinfuturestudies inrheumatoidarthritispatients.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
theirgenuineengagementintheorganizationofthisstudy.We arealsothankfulforlinguisticcorrectionsofthemanuscript texttoAnaVukovi´c,languageandliteratureprofessor.
r
e
f
e
r
e
n
c
e
s
1. AlamanosY,DrososA.Epidemiologyofadultrheumatoid arthritis.AutoimmunRev.2005;4:130–6.
2. EmeryP,BreedveldFC,DougadosM,KaldenJR,SchiffMH, SmolenJS.Earlyreferralrecommendationfornewly
diagnosedrheumatoidarthritis:evidencebaseddevelopment ofaclinicalguide.AnnRheumDis.2002;61:290–7.
3. BlomM,vanRielPL.Managementofestablishedrheumatoid arthritiswithanemphasisonpharmacotherapy.BestPract ResClinRheumatol.2007;21:43–57.
4. CushJJ.Safetyoverviewofnewdisease-modifying antirheumaticdrugs.RheumDisClinNorthAm. 2004;30:237–55.
5. DeWitMPT,SmolenJS,GossecL,vanderHeijdeDMFM. Treatingrheumatoidarthritistotarget:thepatientversionof theinternationalrecommendations.AnnRheumDis. 2011;70:891–5.
6. VoithAM,FrankAM,SmithPiggJ.Nursingdiagnosis:fatigue. In:CarrollJohnsonRM,editor.Classificationofnursing diagnoses.Proceedingsof8thConferenceNANDA.St.Louis: Mosby;1989.
7. KirwanJR,HewlettS.Patientperspective:reasonsand methodsformeasuringfatigueinrheumatoidarthritis.J Rheumatol.1992;34:1171–3.
8. MinnockP,KirwanJ,BresnihanB.Fatigueisareliable, sensitiveanduniqueoutcomemeasureinrheumatoid arthritis.Rheumatology.2009;48:1533–6.
9. WareJEJr,SherbourneCD.TheMOS36-ItemShort-Form HealthSurvey(SF-36).I.Conceptualframeworkanditem selection.MedCare.1992;30:473–83.
10.HewlettS,CockshottZ,ByronM,KitchenK,TiplerS,PopeD, etal.Patients’perceptionsoffatigueinrheumatoidarthritis: overwhelming,uncontrollable,ignored.ArthritisRheum. 2005;53:697–702.
11.Repping-WutsH,FransenJ,vanAchterbergT,BleijenbergG, vanRielP.Persistentseverefatigueinpatientswith rheumatoidarthritis.JClinNurs.2007;16:377–83.
12.HuyserBA,ParkerJC,ThoresonR,SmarrKL,JohnsonJC, HoffmanR.Predictorsofsubjectivefatigueamongindividuals withrheumatoidarthritis.ArthritisRheum.1998;41:2230–7.
13.WolfeF,MichaudK.Predictingdepressioninrheumatoid arthritis:thesignalimportanceofpainextentandfatigue, andcomorbidity.ArthritisCareRes.2009;61:667–73.
14.SheehyC,MurphyE,BarryM.Depressioninrheumatoid arthritis–underscoringtheproblem.Rheumatology. 2006;45:1325–7.
15.CovicT,CummingSR,PallantJF.Depressionandanxietyin patientswithrheumatoidarthritis:prevalenceratesbasedon acomparisonoftheDepression,AnxietyandStressScale (DASS)andthehospital,AnxietyandDepressionScale (HADS).BMCPsychiatry.2012;12:6.
16.DrentM,LowerEE,DeVriesJ.Sarcoidosis-associatedfatigue. EurRespir.2012;40:255–63.
17.SpitzerRL,KroenkeK,WilliamsJB,LöweB.Abriefmeasure forassessinggeneralizedanxietydisorder:theGAD-7.Arch InternMed.2006;166:1092–7.
18.KroenkeK,SpitzerRL,WilliamsJB,MonahanPO,LöweB. Anxietydisordersinprimarycare:prevalence,impairment, comorbidity,anddetection.AnnInternMed.2007;146:317–25.
19.KroenkeK,SpitzerR,WilliamsJ.ThePHQ-9:validityofabrief depressionseveritymeasure.JGenInternMed.
2001;16:606–13.
20.KroenkeK,SpitzerRL.Thephq-9:anewdepression diagnosticandseveritymeasure.PsychiatrAnn.2002;32:1–7.
21.LöweB,UnützerJ,CallahanCM,PerkinsAJ,KroenkeK. MonitoringdepressiontreatmentoutcomeswiththePatient HealthQuestionnaire-9.MedCare.2004;42:1194–201.
22.MichielsenHJ,deVriesJ,vanHeckGL,vandeVijverFJ, SijtsmaK.Examinationofthedimensionalityoffatigue:the constructionoftheFatigueAssessmentScale(FAS).EurJ PsycholAssess.2004;20:39–48.
23.deVriesJ,MichielsenH,vanHeckGL,DrentM.Measuring fatigueinsarcoidosis:theFatigueAssessmentScale(FAS).BrJ HealthPsychol.2004;9:279–91.
24.HairJF,AndersonRE,TathamRL,BlackWC.Multivariatedata analysis:withreadings.EnglewoodCliffs,NewJersey: Prentice-Hall;1995.
25.DiamantopoulosA,SiguawJA.Formativeversusreflective indicatorsinorganizationalmeasuredevelopment:a comparisonandempiricalillustration.BrJManag. 2006;17:263–82.
26.SlavichGM,IrwinRM.Fromstresstoinflammationandmajor depressivedisorder:asocialsignaltransductiontheoryof depression.PsycholBull.2014;40:774–815.
27.MillerAH.Elucidatingtheconsequencesofchronicstresson immuneregulationandbehaviorinrheumatoidarthritis. BrainBehavImmun.2008;22:22–3.
28.HarrisonMJ,TrickerKJ,DaviesL,HassellA,DawesP,ScottDL, etal.Therelationshipbetweensocialdeprivation,disease outcomemeasures,andresponsetotreatmentinpatients withstable,long-standingrheumatoidarthritis.JRheumatol. 2005;32:2330–6.
29.LöweB,WillandL,EichW,ZipfelS,HoAD,HerzogW,etal. Psychiatriccomorbidityandworkdisabilityinpatientswith inflammatoryrheumaticdiseases.PsychosomMed. 2004;66:395–402.
30.MatchamF,NortonS,ScottDL,SteerS,HotopfM.Symptoms ofdepressionandanxietypredicttreatmentresponseand long-termphysicalhealthoutcomesinrheumatoidarthritis: secondaryanalysisofarandomizedcontrolledtrial. Rheumatology(Oxford,England).2016;55:268–78.
31.MargarettenM,BartonJ,JulianL,KatzP,TrupinL,TonnerC, etal.Socioeconomicdeterminantsofdisabilityand depressioninpatientswithrheumatoidarthritis.Arthritis CareRes(Hoboken).2011;63:240–6.
32.AttarSM.Canwepredictdepressioninpatientswith rheumatoidarthritis.KuwaitMedJ.2014;46:219–24.
33.WattT,GroenvoldM,BjornerJB,NoerholmV,RasmussenNA, BechP.FatigueintheDanishgeneralpopulation.Influenceof sociodemographicfactorsanddisease.JEpidemiol
CommunityHealth.2000;54:827–33.
34.StebbingsS,HerbisonP,DoyleTCH,TreharneGJ,HightonJ.A comparisonoffatiguecorrelatesinrheumatoidarthritisand osteoarthritis:disparityinassociationswithdisability, anxietyandsleepdisturbance.Rheumatology.2010;49: 361–7.
35.CarrolMF,SchadeDS.Apracticalapproachtohypercalcemia. AmFamPhysician.2003;67:1959–66.
36.OelznerP,LenhmannG,EidnerT,FrankeS,MüllerA,WolfG, etal.Hypercalcemiainrheumatoidarthritis:relationship withdiseaseactivityandbonemetabolism.RheumatolInt. 2006;26:908–15.
37.CastrejonI,YaziciY,PincusT.Lowlevelsofformaleducation generallyareassignificantashighageandlongdurationof diseasetoidentifypoorclinicalstatusinpatientswithmost rheumaticdiseases.ArthritisRheum.2013;63.
38.ThybergI,DalhströmO,ThybergM.Factorsrelatedtofatigue inwomenandmenwithearlyrheumatoidarthritis:the SwedishTIRAstudy.JRehabilMed.2009;41:904–12.
39.Rongen-vanDartelSAA,Repping-WutsH,HoogmoedD. Relationshipbetweenobjectivelyassessedphysicalactivity andfatigueinpatientswithrheumatoidarthritis:inverse
correlationofactivityandfatigue.ArthritisCareRes. 2014;66:852–60.