w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Brief
communication
Temporomandibular
disorders
in
fibromyalgia
syndrome:
a
short-communication
Maísa
Soares
Gui
a,∗,
Marcele
Jardim
Pimentel
b,
Célia
Marisa
Rizzatti-Barbosa
baDepartmentofAnatomy,PiracicabaDentalSchool,UniversidadeEstadualdeCampinas,Piracicaba,SP,Brazil
bDepartmentofProsthesisandPeriodontology,PiracicabaDentalSchool,UniversidadeEstadualdeCampinas,Piracicaba,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received6February2014 Accepted18July2014
Keywords:
Fibromyalgia Facialpain
Temporomandibularjoint dysfunctionsyndrome
a
b
s
t
r
a
c
t
Fibromyalgiasyndrome(FMS)isachronicpainfulsyndromeandthecoexistenceofapainful conditioncausedbyTemporomandibularDisorders (TMD)andFMShasbeenfrequently raised forseveralstudies;however,a morelikelyhypothesisisthatasetofFMS char-acteristicsmayleadtotheonsetofTMDsymptomsandtheyarenotmerelycoexisting conditions.Therefore,ouraimispresentingareviewofliteratureabouttherelationbetween fibromyalgiaandthesignsandsymptomsoftemporomandibulardisorders.Forthis pur-pose, abibliographicsearchwasperformedfortheperiodof1990–2013,intheMedline, Pubmed,LilacsandScielodatabases,usingthekeywordsfibromyalgia,temporomandibular disordersandfacialpain.Herewepresentasetoffindingsintheliteratureshowingthat fibromyalgiacanleadtoTMDsymptoms.Thesestudiesdemonstratedgreaterinvolvement ofthestomatognathicsysteminFMSandmyogenicdisordersofmasticatorysystemare mostcommonlyfoundinthosepatients.FMSappearstohaveaseriesofcharacteristics thatconstitutepredisposingandtriggeringfactorsforTMD.
©2014ElsevierEditoraLtda.Allrightsreserved.
Disfunc¸ão
temporomandibular
na
síndrome
da
fibromialgia:
comunicac¸ão
breve
Palavras-chave:
Fibromialgia Dorfacial
Síndromedadisfunc¸ãoda articulac¸ãotemporomandibular
r
e
s
u
m
o
A síndrome dafibromialgia (SFM)é umasíndromedolorosa crônica.Acoexistência de umacondic¸ãodolorosacausadapeladisfunc¸ãotemporomandibular(DTM)epelaSFMtem sidofrequentementedescritapor váriosestudos.Noentanto,ahipótesemaisprovável é queum conjuntode característicasda SFMpodelevaraoaparecimento desintomas deDTM eelasnãosãoapenascondic¸õescoexistentes.Porisso,oobjetivodesteestudo éapresentarumarevisãodaliteraturasobrearelac¸ãoentreafibromialgiaeossinaise
∗ Correspondingauthor.
E-mail:[email protected](M.S.Gui).
http://dx.doi.org/10.1016/j.rbre.2014.07.004
sintomasdadisfunc¸ãotemporomandibular.Paraestefim,fez-seumapesquisa bibliográ-ficaqueenvolveuoperíodode1990a2013nasbasesdedadosMedline,Pubmed,Lilacse Scielo.Foramusadasaspalavras-chavefibromialgia,disfunc¸ãotemporomandibularedor facial.Nestetrabalho,apresenta-seumconjuntodeachadosdaliteraturaquemostram quea fibromialgiapodelevarasintomasde DTM.Estes estudosmostraramummaior envolvimentodosistemaestomatognáticonaSFMequeosdistúrbiosmiogênicosdo sis-temamastigatóriosãoosmaiscomumenteencontradosnessespacientes.ASFMpareceter umasériedecaracterísticasqueconstituemfatorespredisponentesedesencadeantespara aDTM.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Fibromyalgiasyndrome(FMS)isachronicpainfulsyndromeof unknownetiologythataffectspredominantlywomen.1New
criteriaforclinicaldiagnosisoffibromyalgiahavebeen pro-posedbythe AmericanCollegeofRheumatology(ACR)due torecognitionoftheimportanceofcognitiveproblemsand somaticsymptoms.2
Theyidentifiedtwovariablesthatbestdefinedfibromyalgia anditssymptomspectrum:thewidespreadpainindex(WPI) and thesymptom severity(SS)scale.TheSS scalescore is thesumoftheseverityofthe3symptoms(fatigue,waking unrefreshed,cognitivesymptoms)plustheextent(severity) ofsomaticsymptomsingeneral.Accordingtothisstudy,2 a
patientsatisfiesdiagnosticcriteriaforfibromyalgiaifthe fol-lowing3conditionsaremet:WPI≥7andSSscalescore≥5or WPI3–6andSSscalescore≥9;furthermore,symptomshave beenpresentatasimilarlevelforatleast3monthsandthe patientdoesnothaveadisorderthatwouldotherwiseexplain thepain.
Other symptoms such as sleep disturbances, depres-sion and fatigue are also associated with this disease. In addition, the coexistence ofa painful condition caused by temporomandibular disorders (TMD) and fibromyalgia has beenfrequentlyraisedforseveralstudies.TMDareasetof conditions affectingthe masticatorymuscles or joints and exhibitingpainastheirprimarycharacteristic.3
Hedenberg-Magnussonetal.4foundthatFMSpatientshave
frequentandseveresymptomsofTMDand94%reportedlocal painfromthetemporomandibularsystemwithamean dura-tionof12years.Generalbodypainhadasignificantlylonger durationthanTMD,whichindicatesthatfibromyalgiastarts inotherpartsofthebodyandlaterextendstothe temporo-mandibularregion.Therefore,amorelikelyhypothesisisthat asetofFMSsymptomsmayleadtotheonsetofTMD symp-toms,whilethereisaTMDsubgroupofpatientsthatcould present widespread pain, but donot meet the criteria for fibromyalgia.
Afterall,ourobjectiveispresentingareviewofliterature about therelationbetweenfibromyalgia and thesigns and symptomsoftemporomandibulardisorders.
Methods
Bibliographic search of electronic bibliographic databases (Medline, Pubmed, Lilacs and Scielo) for the period from
January1990 to December2013 was performed utilizing the keywords:
“TemporomandibularDisorders”or“FacialPain”combined with“Fibromyalgia”.
Initially,122pagesofresultswerefound.Then,two inde-pendent reviewers read the abstracts and those that were selected by consensus to the following inclusion criteria: PatientswithfibromyalgiaandTMDdiagnosis.Weexcluded articles, which didnot address onlythesetwo pathologies and thosethatdidnotaimtorelatethesymptomsofboth syndromes.
We selected 158 articles with cross-sectional design, which were thenreadand evaluatedforinclusion into the literaturereview.Consideringtheheterogeneityofthe stud-ies, additional inclusion criteria forresearch articles were: Investigations of the relationship and differences between fibromyalgia and TMD (n=13 papers selected), prevalence (n=7papers selected), and investigationsabout facial pain symptomsinFMS(n=8papersselected).
Results
TMDprevalenceinFMS
FMSpatientsare31timesmorelikelytohaveadiagnosisof facialmusclepainthanpatientswithoutthecondition.5
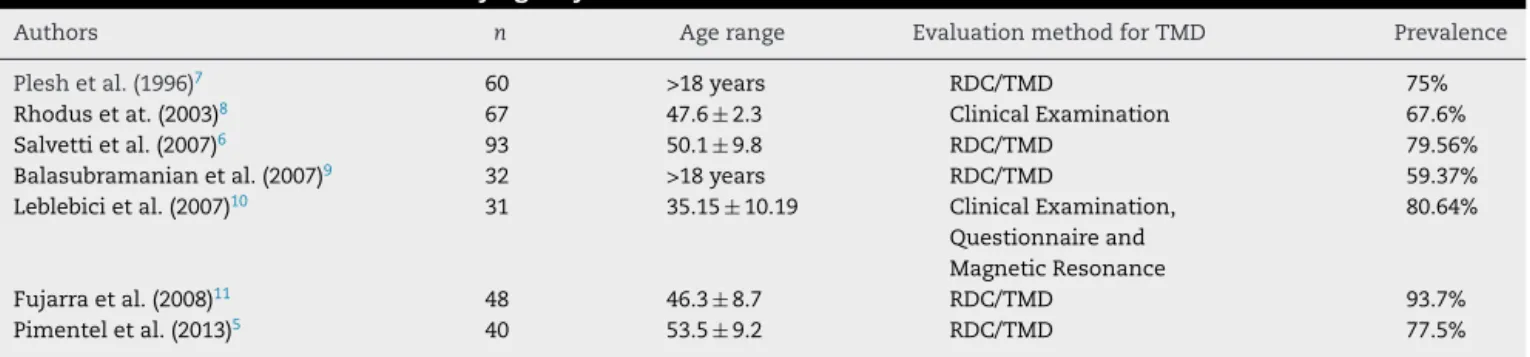
More-over,theliteraturepointstoahighprevalenceofTMDinthese patients(Table1).
OnlytwostudiesusedclinicalexaminationforTMD diag-nosesandfivestudiesusedtheResearchDiagnosticCriteria for TemporomandibularDisorder (RDC/TMD) that isa gold standard toolforTMDdetection.Regardless ofthe evaluat-ingmethods,thesestudiesshowaprevalencerangebetween 59.37%and93.7%,whichcanbeexplainedbymanyfactors. Oneofthemarethedifferentpopulationsstudied(e.g.Italy,6
UnitedStates,7–9Turkey10andBrazil5,11).
Moreover,whetherfibromyalgiastartsinotherpartsofthe bodyandlaterextendstothetemporomandibularregion,4the
timeofdiagnosis offibromyalgiacould influenceon preva-lenceresults.Therefore,chronicFMSpatientmightpresenta greaternumberofsymptomsofTMD.
TMDsignsandsymptomsinFMS
Table1–PrevalenceofTMDinfibromyalgiasyndrome.
Authors n Agerange EvaluationmethodforTMD Prevalence
Pleshetal.(1996)7 60 >18years RDC/TMD 75%
Rhodusetat.(2003)8 67 47.6±2.3 ClinicalExamination 67.6%
Salvettietal.(2007)6 93 50.1±9.8 RDC/TMD 79.56%
Balasubramanianetal.(2007)9 32 >18years RDC/TMD 59.37%
Leblebicietal.(2007)10 31 35.15±10.19 ClinicalExamination,
Questionnaireand MagneticResonance
80.64%
Fujarraetal.(2008)11 48 46.3±8.7 RDC/TMD 93.7%
Pimenteletal.(2013)5 40 53.5±9.2 RDC/TMD 77.5%
RDC/TMD,ResearchDiagnosticCriteriaforTemporomandibularDisorder.
region,thetemporomandibularjointormasticatorymuscles, limitationor deviationofmandibularmovement, temporo-mandibularjointnoiseduringthefunctioningofmandibular andpalpationandabnormalrelationofstaticand dynamic oclusal.12
Just recently, psychological and behavioral factors have become well-established influences upon a wide range of painconditions including TMD pain. Genetics and sensory processingalsocontributetoTMDetiology.3
Individuals with these conditions (e.g. FMS and TMD) display diffuse hyperalgesia (increased pain to normally painfulstimuli)and/orallodynia(paintonormallynonpainful stimuli). This abnormality across conditions suggests that these individuals have a fundamental problem with pain orsensory processingratherthan anabnormalityconfined toaspecificregion ofthebody wherepain isperceived to originate.13
Pleshetal.7reportedthatasmallproportionofpatients
with TMD (18.4%) also had FMS, but most of those with FMS(75.0%)satisfiedcriteriaformuscular(myofascial)TMD. PatientswithFMShadlowerpainthresholdsandmoresevere manifestationsofalldiseasemeasures(e.g.,pain,fatigueand sleep) compared to those with TMD. They also had more painfulbodyregions.PatientswithFMSalsodiffered signif-icantlyfromthosewithTMDinself-reportedworkabilityand healthassessment.ThefeaturesthatbestdifferentiatedFMS fromTMDarefunctionaldisability,reportsofworkdifficulty, andgeneraldissatisfactionwithhealth.
In addition, FMS patients present high prevalence of myofascialpainonpalpationandduringmandibular move-ments, as a high self-reported daytime clenching and grinding.5
TMDonsetinFMS
Infibromyalgia,TMDhasaninsidiousonset,andetiologyis notfully known,inwhichbiochemical abnormalities, neu-roendocrine,and mechanisms ofcentral sensitization may play an important etiological role.14 According to Saltareli
et al.15 the complexity offactors involvedin the frame of
fibromyalgia, to the question of diagnosis and the proper approachbyhealthprofessionals, showstheneedformore studies that propose to expand the understanding of the issuesexperiencedbythesepatients.
Highfrequencyofheadache (78%),facialpainand tired-nessofthejawswerefoundinFMSandaboutfiftypercent
of the patientsof Hedenberg-Magnusson et al.4 study also
complainedaboutdifficultiestoopenthemouthandtochew. Thisstudyshowsthatpatientswithfibromyalgiaoftensuffer fromsymptomsofTMD,andthattheintensityofthepainis correlatedtogeneralbodypain.Thesefindingsindicatethat fibromyalgiaisoneofthecausesofTMD.
As well as FMS, in temporomandibular disorders, widespread pain is presented. Some studies have showed thatpatientswithTMDfrequentlydescribepaininmultiple body parts16 and overlap oftenderand trigger points was
foundinbothpatientgroups17whichisinconsistentwiththe
pathogeneticconceptofmyofascialtriggerpointsandlocal disturbancesoforofacialstructuresastheonlyonescausing TMDchronicpain.
However,arguingagainstanytransitionfromTMDtoFMS, Pfauetal.(2009)18describedasensitiveTMDsubgroupthat
resemblesFMS patients, but theyranked in-between them andhealthycontrols.Inaddition,FMSpatientsreportedthe longestpaindurationandthehighestimpairmentindailylife comparedtosensitiveandinsensitiveTMD.
WidespreadpaininTMDandFMS
Manypossiblefactors(e.g.environmental,genetic,cognitive, behavior)related towidespreadpainpresenceinTMD and FMSwerefoundanddiscussedintheliterature.
Among them,somefindings showed that patients with FMSandTMDsymptomssuchaschronicpainandstresscould increasesympatheticactivity,whichaltersthecardiovascular responsesandmakesthepainworse.Lightetal.19evaluated
10fibromyalgia,10TMDpatientsand16healthycontrolsand their resultssupportthe hypothesisthat bothfibromyalgia and thosewithTMDoftendevelopadysregulationof beta-adrenergicactivitythatcontributestoalteredcardiovascular responsesandcatecholaminesandseverityofclinicalpain.
BothFMSandTMDareclassifiedinthefamilyofcentral sensitivity syndromes and have severalsimilar features in common,e.g.,sleepdisturbances.20Smithetal.21suggested
thattheassociationofprimaryinsomniaandhyperalgesiaat anonorofacialsite suggeststhatprimaryinsomnia maybe linkedwithcentralsensitivityandcouldplayanetiologicrole inidiopathicpaindisorders,therefore,sleepdisturbancesare alsoconsideredanimportantriskindicatorforthe develop-mentofTMD.
subjectiveexperienceofunrefreshingsleep),22patientswith
TMDalsohadhigherimpairmentsonsleepand depression scores23 and excessive daytime sleepinesswas frequentin
patientswithmyofascialpainTMD.24
Inpatientswithfibromyalgiasyndromeandother gener-alizedpain syndromes, stressalso playsanimportantrole andthereisacloseassociationbetweenexacerbationofpain symptoms,increasedanxiety,andexposuretostressors.25
AsFMS, patients withTMD have reportedhigher levels ofaffectivedistress,somaticawareness,psychosocialstress, depressionandpaincatastrophizing.26Paincatastrophizing,
or responses to pain that characterize it as being awful, horrible, and unbearable, is increasingly recognized as an extremelyimportantcontributor tothe experienceofpain. Althoughchronicpainandpsychiatricconditionsoften co-occur, studies havefound catastrophizing tobe associated withpainandpain-relateddisabilityindependentofthe influ-enceofdepression.13
Inaddition,supportingthepossibleroleofgeneticfactors intheetiologyoffibromyalgia,onemajorlocusfor fibromyal-giaonthechromosome17p11.2–q11.2regionwasdetectedand thischromosomeregioncoincideswiththemapcoordinate for2potentialcandidategenesforfibromyalgia:theserotonin transportergene(SLC6A4)andthetransientreceptorpotential vanilloidchannel2gene(TRPV2).27
Recently,caseswithlocalizedTMDdifferedfromhealthy controls in allelic frequency of single nucleotide polymor-phisms (SNPs) that mapped to a serotonergic receptor pathway,whilecasesofTMDwithwidespreadpaindiffered inallelicfrequencyofSNPsthatmappedtoaT-cellreceptor pathway.28
Muscleimpairment
Musclesasapossiblesourceofpaininfibromyalgiahavebeen studiedextensively.Donaldsonetal.29examinedtheelectrical
characteristics(bysurfaceelectromyography)ofdiffuse mus-cularcoactivationassociatedwiththetenderpointsofFMS.It isdefinedasanincreasefromrestinglevels(tonus)inthe elec-tricalactivityofanymuscleduringamovement,whichdoes notinvolvethatmuscleandisnotpartofthe agonist.The resultsshowanincreaseinelectricalactivityinFMSpatients ascomparedtocontrols.Coactivationwasstrongerproximal totheneckanddecreasedinintensityasthearearecorded moveddistally.
Painandrestrictedmovementintheneckareaisconnected to the limitation in the jaw opening30 and an association
betweenthefunctionofthemasticatorymusclesand tem-poromandibularjointsandthemobilityofcervicalspineand tendernessoftheneck-shouldermuscleswasfound.31
Trapez-ius musclehasanimportantFMStenderpointandcan be highlightedthatuppertrapeziusmuscle(innervatedbycranial nerveXI)andmasticatorymuscles(e.g.masseterand tempo-ralis)arestriatedmusclesthatariseembryologicallyfromthe branchialarches.32
The local and referred pain elicited from active trigger pointsinthemasticatoryandneck-shouldermusclesshared similarpainpatternasspontaneousTMD,whichsupportsthe conceptofperipheralandcentralsensitizationmechanisms inmyofascialTMD.33
Itwassuggestedthatsensitizationofmusclenociceptors isrevealedbyabnormalpatternsofreflexmotorneuron acti-vationinpatientswithFMS.34 Adifferentpatternofmuscle
activation was observedintheFMS groupwhencompared with the TMD group, it seems that muscles impaired by FMScouldalreadypresentaconditionofpremature interrup-tion ofmusclecontraction,contraction mayhaveoccurred, dischargingthemotorunitsathigherfrequencies(tetanic con-traction)inordertoactivatetherequiredcontraction,whichis evenmorefatiguing,generatingacycleofmusclefatigueand pain.35
Elert et al.36 alsosuggest that the FMS patientshad an
inabilitytorelaxthemusclethroughouttheirbodiesbetween tasksandanotherstudyreportedthatFMShadsignificantly higherconductionvelocityintrapeziusmusclecontractions ofsinglemotorunits,37 i.e.increasingthenumberofactive
motorunits.
Discussion
Theliteraturefindings demonstrate greaterinvolvementof thestomatognathicsysteminfibromyalgiaandmyogenic dis-orders ofmasticatorysystemare mostcommonlyfoundin those patients. Fibromyalgia syndrome appears to have a seriesofcharacteristicsthatconstitutepredisposingand trigg-eringfactorsforTMD.
Ontheotherhand,widespreadpaininTMDshouldnotbe confoundedasfibromyalgia,butinsteadassuggestedbyPfau etal.(2009)18thereisasubgroupofTMDpatientsthathave
becomemoresensitivetopain.
Main similarities and differences between them are, respectively, widespread pain presence with psychological distress,andtheprevalenceandseverityofsymptoms,which are higherinFMSpatients(e.g. sleepproblems,depression, somatization,pain).
Although these two syndromes appear to overlap, the literature has shown that possibly the pathophysiology is different, mainly due to a strong genetic component of fibromyalgia,27 alsoconsidering thatenvironmental factors
influence the occurrence of the phenotype. Our review of literature also presented many studies suggesting that fibromyalgiacanleadtoTMDsymptoms,buttheyhave cross-sectional designsthat preventtemporal conclusions(cause andconsequence)frombeingdrawn.
Psychosocial factors likesleep problems, abnormal neu-romuscular response and central sensitization,acting con-comitantlyinFMS,couldeasilyexceedthelimitoffunctional adaptationtostressinthetemporomandibularsystemleading toitsdysfunctionandpain.35
TMDcasesalsoreportedhigherlevelsofpsychologicaland affectivedistress,greater perceivedstressand catastrophiz-ing,andincreasedsomaticawarenesscomparedtocontrols.26
Similarfindingssupportingpsychosocialvariablesas premor-bid riskfactors fordevelopmentofchronicpain havebeen reportedforotherchronicpainconditions,includingchronic widespreadpain,i.e.,fibromyalgia.38
TMDinpatientswithFMS,39thereby,alsoactingas
perpetu-atingfactorsforTMD.
Conclusion
Fibromyalgia syndrome presents a set of conditions that constitute predisposingand triggering factorsfor temporo-mandibulardisordersandcouldexplainthehighprevalence ofTMDsignsandsymptomsinthesepatients.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. WolfeF,SmytheHA,YunusMB,BennettRM,BombardierC, GoldenbergDL,etal.TheAmericanCollegeofRheumatology 1990criteriafortheclassificationoffibromyalgia.Arthritis Rheum.1990;33:160–72.
2. WolfeF,ClauwDJ,FitzcharlesM,GoldenbergDL,KatzRS, MeaseP,etal.TheAmericanCollegeofRheumatology preliminarydiagnosticcriteriaforfibromyalgiaand measurementofsymptomseverity.ArthritisCareRes. 2010;62:600–10.
3. OhrbachR,FillingimRB,MulkeyF,GonzalezY,GordonS, GremillionH,etal.Clinicalfindingsandpainsymptomsas potentialriskfactorsforchronicTMD:descriptivedataand empiricallyidentifieddomainsfromtheOPPERAcase-control study.JPain.2011;12:T27–45.
4. Hedenberg-MagnussonB,ErnbergM,KoppS.Presenceof orofacialpainandtemporomandibulardisorderin fibromyalgia.Astudybyquestionnaire.SwedDentJ. 1999;23:185–92.
5. PimentelMJ,GuiMS,MartinsdeAquinoLM,Rizzatti-Barbosa CM.Featuresoftemporomandibulardisordersinfibromyalgia syndrome.JCranioPract.2013;31:40–5.
6. SalvettiG,ManfrediniD,BazzichiL,BoscoM.Clinicalfeatures ofthestomatognathicinvolvementinfibromyalgia
syndrome:acomparisonwithtemporomandibulardisorders patients.JCranioPract.2007;25:127–33.
7. PleshO,WolfeF,LaneN.Therelationshipbetween fibromyalgiaandtemporomandibulardisorders:prevalence andsymptomseverity.JRheumatol.1996;23:1948–52.
8. RhodusNL,FrictonJ,CarlsonP,MessnerR.Oralsymptoms associatedwithfibromyalgiasyndrome.JRheumatol. 2003;30:1841–5.
9. BalasubramaniamR,deLeeuwR,ZhuH,NickersonRB, OkesonJP,CarlsonCR.Prevalenceoftemporomandibular disordersinfibromyalgiaandfailedbacksyndromepatients: ablindedprospectivecomparisonstudy.OralSurgOralMed OralPatholOralRadiolEndod.2007;104:204–16.
10.LeblebiciB,Pektas¸ZÖ,OrtancilÖ,HürcanEC,BagisS,Akman MN.Coexistenceoffibromyalgia,temporomandibular disorder,andmasticatorymyofascialpainsyndromes. RheumatolInt.2007;27:541–4.
11.FujarraFJC[Dissertac¸ão]Disfunc¸ãotemporomandibulare síndromefibromiálgica:caracterizac¸ãodeamostrasegundo critériosclínicos.SãoPaulo:FaculdadedeMedicinada UniversidadedeSãoPaulo;2008.
12.DworkinSF,LeRescheL,DeRouenT,VonKorffM.Assessing clinicalsignsoftemporomandibulardisorders:reliabilityof clinicalexaminers.JProsthetDent.1990;63:574–9.
13.WilliamsDA,ClauwDJ.Understandingfibromyalgia:lessons fromthebroaderpainresearchcommunity.JPain.
2009;10:777–91.
14.AdlerGK,ManfredsdottirVF,CreskoffKW.Neuroendocrine abnormalitiesinfibromyalgia.CurrPainHeadacheRep. 2002;6:289–98.
15.SaltareliS,PedrosaDFA,HortenseP,SousaF.Avaliac¸ãode aspectosquantitativosequalitativosdadornafibromialgia. RevBrasReumatol.2008;48:151–6.
16.ChenH,SladeG,LimPF,MillerV,MaixnerW,DiatchenkoL. Relationshipbetweentemporomandibulardisorders, widespreadpalpationtenderness,andmultiplepain conditions:acase-controlstudy.JPain.2012;13:1016–27.
17.GrangesG,LittlejohnG.Prevalenceofmyofascialpain syndromeinfibromyalgiasyndromeandregionalpain syndrome:acomparativestudy.JMusculoskeletPain. 1993;1:19–35.
18.PfauDB,RolkeR,NickelR,TreedeRD,DaublaenderM. Somatosensoryprofilesinsubgroupsofpatientswith myogenictemporomandibulardisordersandfibromyalgia syndrome.Pain.2009;147:72–83.
19.LightKC,BragdonEE,GrewenKM,BrownleyKA,GirdlerSS, MaixnerW.Adrenergicdysregulationandpainwithand withoutacutebeta-blockadeinwomenwithfibromyalgiaand temporomandibulardisorder.JPain.2009;10:542–52.
20.YunusMB.Fibromyalgiaandoverlappingdisorders:the unifyingconceptofcentralsensitivitysyndromes.Semin ArthritisRheum.2007;36:339–56.
21.SmithMT,WickwireEM,GraceEG,EdwardsRR,BuenaverLF, PetersonS,etal.Sleepdisordersandtheirassociationwith laboratorypainsensitivityintemporomandibularjoint disorder.Sleep.2009;32:779–90.
22.StoneKC,TaylorDJ,McCraeCS,KalsekarA,LichsteinKL. Nonrestorativesleep.SleepMedRev.2008;12:275–88.
23.SelaimenC,JeronymoJ,BrilhanteDP,GrossiML.Sleepand depressionasriskindicatorsfortemporomandibular disordersinacross-culturalperspective:acase-controlstudy. IntJProsthodont.2006;19:154–61.
24.CollesanoV,SeguM,MasseroliC,ManniR.
Temporomandibulardisordersandsleepdisorders:which relationship?MinervaStomatol.2004;53:661–8.
25.GreenPG,AlvarezP,GearRW,MendozaD,LevineJD.Further validationofamodeloffibromyalgiasyndromeintherat.J Pain.2011;12:811–8.
26.FillingimRB,OhrbachR,GreenspanJD,KnottC,DubnerR, BairE,etal.Potentialpsychosocialriskfactorsforchronic TMD:descriptivedataandempiricallyidentifieddomains fromtheOPPERAcase-controlstudy.JPain.2011;12:T46–60.
27.ArnoldLM,FanJ,RussellIJ,YunusMB,KhanMA,KushnerI, etal.Thefibromyalgiafamilystudy:agenome-widelinkage scanstudy.ArthritisRheum.2013;65:1122–8.
28.SladeGD,SmithSB,ZaykinDV,TchivilevaIE,GibsonDG, YuryevA,etal.Facialpainwithlocalizedandwidespread manifestations:separatepathwaysofvulnerability.Pain. 2013;154:2335–43.
29.DonaldsonC,MacInnisA,SnellingL,SellaG,MuellerH. Characteristicsofdiffusemuscularcoactivation(DMC)in personswithfibromyalgia–part2.NeuroRehabil. 2002;17:41–8.
30.ErikssonP,Häggman-HenriksonB,ZafarH.Jaw–neck dysfunctioninwhiplash-associateddisorders.ArchOralBiol. 2007;52:404–8.
31.SipiläK,SuominenAL,AlanenP,HeliövaaraM,TiittanenP, KönönenM.Associationofclinicalfindingsof
temporomandibulardisorders(TMD)withself-reported musculoskeletalpains.EuroJPain.2011;15:1061–7.
33.Fernández-de-las-Pe ˜nasC,Galán-del-RíoF,Alonso-BlancoC, Jiménez-GarcíaR,Arendt-NielsenL,SvenssonP.Referred painfrommuscletriggerpointsinthemasticatoryand neck-shouldermusculatureinwomenwith
temporomandibulardisorders.JPain.2010;11:1295–304.
34.VierckCJJr.Mechanismsunderlyingdevelopmentofspatially distributedchronicpain(fibromyalgia).Pain.2006;124:242–63.
35.GuiMS,PedroniCR,AquinoLMM,PimentelMJ,AlvesMC, RossiniS,etal.Facialpainassociatedwithfibromyalgiacan bemarkedbyabnormalneuromuscularcontrol:a
cross-sectionalstudy.PhysTher.2013;93:1092–101.
36.ElertJ,Rantapää-DahlqvistS,Henriksson-LarsenK,Lorentzon R,GerdleB.Muscleperformance,electromyographyandfibre
typecompositioninfibromyalgiaandwork-relatedmyalgia. ScandJRheumatol.1992;21:28–34.
37.GerdleB,ÖstlundN,GrönlundC,RoeleveldK,KarlssonJS. Firingrateandconductionvelocityofsinglemotorunitsin thetrapeziusmuscleinfibromyalgiapatientsandhealthy controls.JElectromyogrKinesiol.2008;18:707–16.
38.McBethJ,MacfarlaneGJ,BenjaminS,SilmanAJ.Featuresof somatizationpredicttheonsetofchronicwidespreadpain: resultsofalargepopulation-basedstudy.ArthritisRheum. 2001;44:940–6.