Disponible en castellano/Disponível em língua portuguesa SciELO Brasil www.scielo.br/rlae 1 RN, PhD in Nursing, Professor; 2 RN, Family Health Program at Marília, Brazil, Specialist in Family Health, Colaborator Professor; 3 Physician, Master in Public Health, Professor. Medical School at Marília, Brazil
COMMUNITY CONTRIBUTIONS TO A FHU TEAM WORK
Maria José Sanches Marin1 Luciana Rocha de Oliveira2 Mércia Ilias3
Elza de Fátima Ribeiro Higa1
Marin MJS, Oliveira LR, Ilias M, Higa EFR. Community contributions to a FHU team work. Rev Latino-am Enfermagem 2007 novembro-dezembro; 15(6):1065-71.
Considering the importance of people participating in the construction of new health models, this study aimed to characterize and analyze contributions brought by community to health actions carried out in a Family Health Unit. It is a documentary analysis based on the records of 24 monthly meetings between the team and community. After reading the records, subject was divided into four themes: material and human resources, availability to secondary level health services, community adherence to the unit activities, health promotion and disease prevention. Discussions opened a wide perspective on health and stimulated co-responsibility, stronger links and information exchanging. Nevertheless, there is a need to improve community effective participation in the co-management of the health system.
DESCRIPTORES: family health program; community participation; public health
LAS CONTRIBUCIONES DE LA COMUNIDAD PARA EL TRABAJO DEL EQUIPO DE UN PSF
Considerando la relevancia de la participación de la población en la construcción de nuevos modelos de salud, el presente estudio propone caracterizar y analizar las contribuciones de la participación de la comunidad en las acciones de salud de una Unidad de Salud de la Familia. Se trata de un estudio de análisis documentario, basado en actas de 24 reuniones mensuales del equipo con la comunidad. Después de la lectura de los registros, los asuntos fueran clasificados en cuatro temáticas: recursos materiales y humanos, accesos a los servicios de salud de nivel secundario, adherencia de la comunidad a las actividades ofrecidas por la unidad y promoción de la salud y prevención de enfermedades. Verificó-se que las discusiones destacaron una visión íntegra de la salud e hicieron posible la co-responsabilidad, fortalecimiento del vínculo y cambio de información. Todavía es necesario avanzar para obtener la efectiva participación de la comunidad en la co-gestión del sistema de salud.
DESCRIPTORES: programa salud de la familia; participación comunitaria; salud pública
AS CONTRIBUIÇÕES DA COMUNIDADE PARA O TRABALHO DA EQUIPE DE UM PSF
Considerando a relevância da participação popular na construção de novos modelos de saúde, o presente estudo propõe-se a verificar as contribuições dessa participação nas ações de saúde de uma Unidade de Saúde da Família. Trata-se de estudo de análise documental, a partir de atas de 24 reuniões mensais da equipe com a comunidade. Após a leitura dos registros, os assuntos discutidos foram agrupados em quatro temáticas: recursos materiais e humanos, acesso aos serviços de saúde de maior complexidade, adesão da comunidade às atividades oferecidas pela unidade e promoção da saúde e prevenção de doenças. Constata-se que, embora as discussões vislumbrem a visão integral da saúde e possibilitem co-responsabilidade, fortalecimento do vínculo e troca de informação, ainda é necessário maior avanço para se obter a efetiva participação da comunidade na co-gestão do sistema de saúde.
INTRODUCTION
C
ommunity participation is a movement thathas been encouraged as a strategy to face health
problems, thus achieving greater political awareness
and sharing the responsibilities and information, in
the attempt to improve people’s autonomy and quality
of life.
Citizens’ participation in the public
management of health has been articulated since the
National Sanitary Reform Movement. The landmarks
for the restatement and consolidation of this
movement were the 8th and 9th National Conferences,
held in 1986 and 1992, respectively. It has been taking
place in the Municipal Health Councils (CMS), whose
composition, parity and attributions are guaranteed
by a judicial rule(1).
The design of the Brazilian health policy,
according to the 1988 constitution, contributes to this
construction by attributing to the Ministry of Health
the commitment to restructure the care model, based
on the health reference framework as a civil right
and assuming the organization of increasingly
problem-solving, integral and humanized services(2).
In this proposal, the achievement of “health
for all” by the year 2010 will not be possible without
people’s active participation, as the certainty to boast
prevention and primary health care depends on them.
This participation should also facilitate the coordination
of multiple state activities in the health area and
permit the construction of aw an holistic health vision
to be built(3).
Civil participation is characterized by the
replacement of the community or people category by
society as the central category. This concept is based
on the universalization of social rights, the expansion
of the citizenship concept and a new understanding of
the State’s nature, leading to the definition of the public
policy priorities based on a public debate(4). Hence,
this participation can be considered as control over
the situation itself, through interventions in decisions,
initiatives and management that affect the living
conditions this situation and projects develop in(5).
Due to these activities, collective involvement
has gradually established itself in recent years and
has produced political guidelines more and more
compatible with reality, so as to guarantee and
rationalize material, financial and human resources,
while people become increasingly aware of their tasks
and responsibilities(6).
Nowadays, after almost two decades of
elaboration of this model, the importance of society’s
active and continuous participation in the actions to
be developed seems evident. The implementation of
the Family Health Program (PSF), which has been
taking place throughout the country, contributes to
that and has characteristics that favor the integration
between the community and the family health teams,
as well as the worker-user relation. In this sense, the
introduction of community health agents (ACS) in the
teams, the enrollment of users in a defined territory
and team work are emphasized.
At family health units, team work favors the
community’s involvement and participation in the
elaboration of a common care project, as the reference
population is the recipient of the work developed,
assuming an institutional democratization process.
Therefore, the PSF philosophy seeks to achieve
a long-term change in the relationship between citizens
and the State, promoting the concept of health as a
civil right and permitting the subjects’ active insertion
in quality of life improvement processes through their
participation in public policy discussions(6).
Even though this participation is considered
relevant, a study about the PSF points to the absence
of users as protagonists of their own living and the
production of their care, as the team still places the
population beyond the scope of the decisions made
in their respect(7). The advances in participation and
team work have not guaranteed the elaboration of a
common care project(4).
The democratic participation in the decisions
and actions that define the fate of the Brazilian society
is being conquered through hard work, in view of the
authoritarian and excluding tradition that has
constituted the Brazilian society throughout history(8).
Therefore, acknowledging the relevance of
community people’s participation in the implementation
of a model that aims to improve the quality of life and
the difficulties to put it in practice, we try to understand
how this participation has been taking place in a PSF,
with a view to contributing with data that permit the
reflection and development of this elaboration.
PURPOSE
To check how community participation
contributes in the health actions of a Family Health
METHODS
This is a documentary analysis study, using
the minutes of team meetings with the community at
the Santa Augusta USF, located in Marília.
The Santa Augusta Family Health Unit started
its work on April 27, 2003. The coverage area includes
2,348 people. The health team consists of one
physician, one nurse, one dentist, one dental aid, two
nursing aids, six community agents, one general
service aid and, twice a week, one driver. Besides
serving as a training area for the first, second and
fourth years of the Nursing and Medical Courses at
Marília School of Medicine and for the
Multi-Professional Family Health Residence at the same
institution, the USF offers medical residents and
nurses and, as of 2006, dentistry, physical therapy
and social service residents. The USF delivers care to
the urban and rural population.
In addition to meeting the demand of medical,
nursing and dentistry visits, the team performs home
visits to people considered at higher risk and with
disabling diseases, and activities with hypertensive
and diabetes patients groups, soccer, walks, food
reeducation, handicraft, hair cut, pre-natal care,
growth and development group, and others. Team
meetings are held on a weekly basis, when community
problems and the team work process are discussed.
Once a month, a community meeting is held
with the participation of team professionals, students
from Marília School of Medicine (Medicine and Nursing
Courses), the chairman of the local community, South
Region Board (CONSUL) and other community
members. In addition to the team members,
approximately four to ten people participate in the
meetings. These meetings are recorded in minutes
and sent to the PSF Management Team at the Marília
Municipal Hygiene and Health Department.
To perform this study, we used the data
recorded in minutes of 24 meetings held by the Santa
Augusta SPF community, from March 2003 to March
2006.
The result analysis followed the steps of the
content analysis technique described by Bardin(9),
including: floating reading of each record unit; second
reading to separate the record units for classification
and to join the raw data contained in these units,
representing the content; and categorization per
record unit groups of common meaning and elements.
This analysis made it possible to joint the minutes of
the discussions within four themes: material and
human resources, access to more complex health
services, adherence of the community to the activities
provided by the unit, and health promotion and
disease prevention, which are shown as tables with
the respective common elements, followed by the
descriptive analysis.
RESULTS
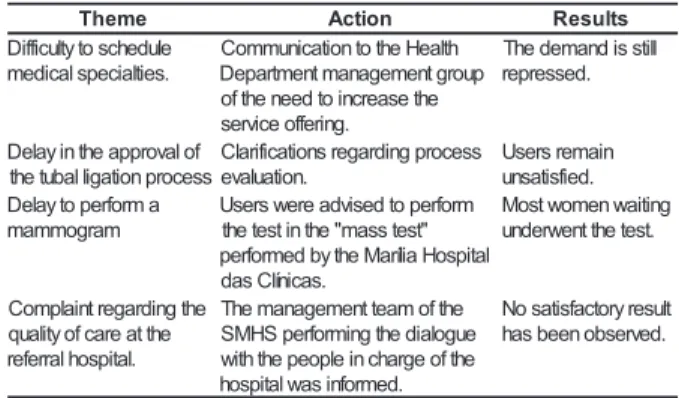
When referring to the themes discussed in
the PSF team meetings, whose minutes were
analyzed, the theme access to more complex health
services, joined in Table 1, shows to be a community
concern, due to the limits imposed on health care
continuity.
Table 1 - Distribution of subjects, actions and results
obtained from the community meetings with the USF
regarding the theme: access to more complex health
services. Marília, 2006
e m e h
T Action Results
e l u d e h c s o t y tl u c if f i D
. s e it l a i c e p s l a c i d e m
h tl a e H e h t o t n o it a c i n u m m o C
p u o r g t n e m e g a n a m t n e m t r a p e D
e h t e s a e r c n i o t d e e n e h t f o
. g n i r e f f o e c i v r e s
ll it s s i d n a m e d e h T
. d e s s e r p e r
f o l a v o r p p a e h t n i y a l e D
s s e c o r p n o it a g il l a b u t e h t
s s e c o r p g n i d r a g e r s n o it a c if i r a l C
. n o it a u l a v e
n i a m e r s r e s U
. d e if s it a s n u a
m r o f r e p o t y a l e D
m a r g o m m a m
m r o f r e p o t d e s i v d a e r e w s r e s U
" t s e t s s a m " e h t n i t s e t e h t
l a t i p s o H a il í r a M e h t y b d e m r o f r e p
. s a c i n íl C s a d
g n it i a w n e m o w t s o M
. t s e t e h t t n e w r e d n u
e h t g n i d r a g e r t n i a l p m o C
e h t t a e r a c f o y t il a u q
.l a t i p s o h l a r r e f e r
e h t f o m a e t t n e m e g a n a m e h T
e u g o l a i d e h t g n i m r o f r e p S H M S
e h t f o e g r a h c n i e l p o e p e h t h t i w
. d e m r o f n i s a w l a t i p s o h
tl u s e r y r o t c a f s it a s o N
. d e v r e s b o n e e b s a h
The access to health technologies represents
an important aspect to be considered by the sector, as
the implementation of the PSF to reorganizing basic care
has not been enough to meet the population’s needs.
As appointed by Merhy, the PSF must be
explored within its limits and incorporated as an
integrating technological modality of the complex care
net, before it is considered sufficient to solve all
problems(10).
The population’s difficulty to have access to
experts, specific tests and procedures, infringes on
constitutional and regulatory principles of the Brazilian
health service when it considers “health as a right of
all”, “integrality”, “equity” and “universality”.
The difficulty to schedule an appointment with
specific experts and tests, as mentioned by the
and, consequently, the users are predisposed to health
problems, with possible emergency hospitalizations. Additionally, this aspect causes discomfort to the USF
team, which is responsible for providing support and explanations about the delay.
When organizing the health system according to the hierarchization and regionalization principle,
the idea is to extend coverage and democratize access. However, the basic care net has not been able to
become the most important “entrance door”, as shown by the high demand in emergency rooms and difficulty
to obtain expert services(11). This fact is explained by
the lack of resources for health, the misuse of existing resources, in addition to the discrimination in the
private sector, exclusively based on the economic criterion, which seeks to guarantee its survival by
the creation of health insurances.
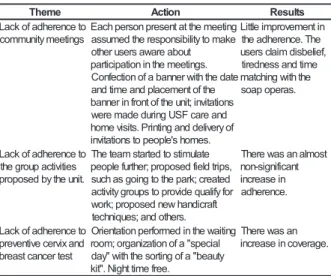
Table 2 - Distribution of subjects, actions and results obtained from community meetings with the USF team
regarding the theme: community adherence to the
activities provided by USF. Marília, 2006
Other promotion and prevention activities
proposed by the team have also shown little
adherence. In our opinion, this deserves reflection
and analysis in terms of effectiveness and adequacy
to the population needs. Additionally, these actions
need to be broadened, involving intersectoriality, not
only to maintain occupation and recreation, but a
qualification that permits conquests and perspectives
of a better quality of life possible.
In literature, most studies about adherence
refer to the process of getting sick and medication
treatment, making it difficult to acquire a further
understanding of the conditions that may be involved
in adherence to promotion and prevention actions like
those proposed by the team, as they demand the
elaboration of civil awareness.
It is remarkable that citizenship “is not
something natural”, as it is subject to social and cultural
rules. In collective societies like the Brazilian, “the
whole prevails over the parts, hierarchy is the basic
principle and the relationship is what matters”.
Therefore, if the subject has no connection with an
important person or institution, he/she is treated as
inferior(13).
Many times, cases of resistance reveal that
people are feeling depreciated or that there does not
exist a real dialog between the team and the users’
knowledge. It is also emphasized that, in the
knowledge confrontation, it is important to consider
the complexity articulated in the historical and cultural
core that makes this knowledge explicit, thus obtaining
an explanation for the difficult adherence(14).
This aspect represents a challenge to
healthcare team professionals, who many times adopt
authoritarian actions, considering their scientific
knowledge as the absolute truth.
Moreover, it seems that the valuation of
healing, medication use and the biological aspect as
the single way to improve health conditions is present
in both the users’ and the team’s imagination. This
fact may also make it more difficult to design measures
that aim for promotion and prevention so as to attend
to people’s needs and, consequently, achieve their
adherence.
Therefore, it seems that the lack of population
adherence to the healthcare actions, in the search
for a better quality of life, is multi-factorial, and the
overcoming of strategies must particularly consider
bonding, knowledge exchange and respect for the
other.
e m e h
T Action Results
o t e c n e r e h d a f o k c a L s g n it e e m y t i n u m m o c g n it e e m e h t t a t n e s e r p n o s r e p h c a E e k a m o t y t il i b i s n o p s e r e h t d e m u s s a t u o b a e r a w a s r e s u r e h t o . s g n it e e m e h t n i n o it a p i c it r a p e t a d e h t h t i w r e n n a b a f o n o it c e f n o C e h t f o t n e m e c a l p d n a e m it d n a s n o it a t i v n i ; t i n u e h t f o t n o r f n i r e n n a b d n a e r a c F S U g n i r u d e d a m e r e w f o y r e v il e d d n a g n it n i r P . s t i s i v e m o h . s e m o h s ' e l p o e p o t s n o it a t i v n i n i t n e m e v o r p m i e lt t i L e h T . e c n e r e h d a e h t , f e il e b s i d m i a l c s r e s u e m it d n a s s e n d e r it e h t h t i w g n i h c t a m . s a r e p o p a o s o t e c n e r e h d a f o k c a L s e it i v it c a p u o r g e h t . t i n u e h t y b d e s o p o r p e t a l u m it s o t d e t r a t s m a e t e h T , s p i r t d l e if d e s o p o r p ; r e h t r u f e l p o e p d e t a e r c ; k r a p e h t o t g n i o g s a h c u s r o f y f il a u q e d i v o r p o t s p u o r g y t i v it c a t f a r c i d n a h w e n d e s o p o r p ; k r o w . s r e h t o d n a ; s e u q i n h c e t t s o m l a n a s a w e r e h T t n a c if i n g i s -n o n n i e s a e r c n i . e c n e r e h d a o t e c n e r e h d a f o k c a L d n a x i v r e c e v it n e v e r p t s e t r e c n a c t s a e r b g n it i a w e h t n i d e m r o f r e p n o it a t n e i r O l a i c e p s " a f o n o it a z i n a g r o ; m o o r y t u a e b " a f o g n it r o s e h t h t i w " y a d . e e r f e m it t h g i N . " t i k n a s a w e r e h T . e g a r e v o c n i e s a e r c n i
From the etymological point of view, adherence,
from the Latin word adhaesione, means junction, union,
approval, agreement, solidarity manifestation, support;
it assumes a relation and link. Multi-factorial process is
understood as a process structured on the relationship
between the care provider and receiver, and involves
continuity, perseverance and frequency(12).
Regarding adherence to the community
meetings, the small number of people participating in
the meetings, around four to ten per meeting, was
discussed. Some appoint “tiredness after work” and
“the time matching with soap operas” as reasons, in
addition to the devaluation of the meeting as a space
Despite low community participation, both in
team meetings and activities developed at the unit, a
great advance is observed in the theme approaches
oriented to health promotion and disease prevention,
revealing concerns with the development of
interventions that go beyond the simple medicalization
of life and aim to improve health levels, as observed
in Table 3.
The Ottawa letter defines health promotion
as “the community qualification process to act in the
improvement of quality of life and health, including a
higher participation in the control of this process”(15).
In this sense, the community meetings have
portrayed the theme, as shown in Table 3.
Table 3 - Distribution of subjects, actions and results
obtained from the community meetings with the USF
team regarding the theme: health promotion and
disease prevention, Marília, 2006
There are also signs of a search for
intersectorial alliances in favor of the population’s health, which focuses on social activities, with the
support of healthcare team professionals.
In the team meetings, one of the themes
emphasized refers to material and human resources of the unit, as seen in Table 4. The lack of basic drugs
was the theme addressed in a number of meetings
and the population’s dissatisfaction is emphasized, as shown by the great value attributed to this item and
the risk that the lack of drugs may represent for the
people’s health.
Table 4 - Distribution of subjects, actions and results
obtained from community meetings with the USF team
regarding the theme: material and human resources of the unit. Marília, 2006
e m e h
T Action Results
t e e r t s e h t n i s l a m i n
A Guidanceregardingtherisks g n i p e e k f o e c n a t r o p m i d n a e h t n i , e m o h t a s l a m i n a ' S C A e h t g n i r u d d n a s g n it e e m . s t i s i v e m o h f o e s a e r c e d a s a w e r e h T e h t n i s l a m i n a f o r e b m u n e h t t e e r t s d a e r p s e g a b r a G s t e e r t s e h t t u o h g u o r h t s n i a r r e t y t p m e d n a . g n il c y c e r f o k c a l d n a e l b a l c y c e r r o f t s e u q e R n i s n a c n o it c e ll o c e g a b r a g ; r e t n e c y t i n u m m o c e h t f o t n o r f d e t t i m s n a r t e l p o e p y t i n u m m o C . s r e h t o e h t o t e c n a d i u g e h t e h t , d e c a l p e r e w s n a c e h T e h t d n a d e d i u g e r e w e l p o e p s m r o f r e p fl e s t i y t i n u m m o c s a w e r e h T . n o i s i v r e p u s e h t e h t n i d e s a e r c e d d e k r a m a . d a e r p s e g a b r a g g n i h t o l C m r a W n g i a p m a C e h t n i s r e n n a b f o t n e m e c a l P m r a w e h t r o f r e n i a t n o c d n a t i n u . g n i h t o l c d e t a n o d g n i h t o l c m r a w e h T y d e e n e h t o t d e t u b i r t s i d s a w . n o it a l u p o p e v it c e ll o C n o it a t r o p s n a r t d a b e h t t u o b a n o i s s u c s i D ' s r e v i r d d n a n o it a z il a n g i s . e c n e d u r p m i e c n a d i u g d n a s e l c a t s b O e l b a t e g e v y t i n u m m o C n e d r a g e h t m o r f t s e u q e r t r o p p u S f o t n e m t r a p e D l a p i c i n u M y t i n u m m o c d n a e r u tl u c i r g A t n e m e r i u q c a e h t n i t n e m e v l o v n i . d n a l d n a s d e e s f o e v a g n a i c i n h c e t e r u tl u c i r g A f o r o b h g i e n a ; n o it a t n e i r o e h t d n a l e h t d e d i v o r p t i n u e h t d e t u b i r t n o c s e i n a p m o c d n a . s d e e s h t i w t n a r G y li m a
F Clariifcaitonsregardingthe d n a n o i s u l c n i r o f a i r e t i r c . m a r g o r p e h t n i e c n e n a m r e p . s n o it s e u q o N e v i s n e h e r p m o C c if f a r T e h t y b t c e j o r p g n i d i v o r p , r e b m a h C r o f s e c r u o s e r o t d e t a l e r s m e l b o r p d n a t n e m e v a p e h t . s t e e r t s f o n o it a z il a n g i s e h t h t i w r e h t e g o t e d a m t r o p e R e h t g n i n i a t n o c y t i n u m m o c g n i r i u q e r s e c a l p e h t d n a s t n e m e v o r p m i e h t h t i w p a m e h t f o n o it a r o b a l e . s e it l u c if f i d f o g n i r o c s , s n g i s c if f a r t f o t n e m e c a l P s e l c a t s b o d n a n o it a z il a n g i s k e e w " a il í r a M e li m S
" Communityinvited. Thirtypeopleattended h tl a e h l a r o t u o b a s e r u t c e l . s t f i g d e v i e c e r d n a . y a D S D I A d l r o
W Invitaitontoparitcipateinthe . p u o r g n o it a t n e i r o t i n u d n a s p u o r g n o it a t n e i r O . s m o d n o c f o n o it u b i r t s i d t n e d i c c a l a n o it a p u c c O k e e w n o it n e v e r p e h t n i e t a p i c it r a p o t n o it a t i v n I p u o r g n o it a t n e i r o t i n u y t i n u m m o c e lt t i L . n o it a p i c it r a p
This discussion leads to the belief that the
population and the team are getting closer and
understand the health concept in a broader sense,
including environment, housing, education, work and
transportation and others.
e m e h
T Action Result
t u o b a s t n e m il p m o C k r o w m a e t m a e t e h t n i g n i d a e R e v it n e c n i n a s a g n it e e m d n a d e if s it a s e b o t d e w o h s m a e T n o it a m r o f n i e h t h ti w d e t a v it o m y t i n u m m o C m a e t n i n o it a p i c it r a p t n e m e v o r p m i k r o w a f o t n e m e c a l P e h t t a x o b s n o it s e g g u s t i n u e h t f o y r t n e t a h t s n o it s e g g u s d d a s r e s u e h T m a e t e h t n i d e s s u c s i d e r a . s g n it e e m m a e t f o e g n a h C . s r e b m e m w e n e h t f o n o it c u d o r t n I . y t i n u m m o c e h t o t n a i c i s y h p o t d e e n e h t f o n o it a c if i r a l C t s i g o l o h c y s p e h t e g n a h c . r e k r o w l a i c o s d n a e h t d e m o c l e w n o it a l u p o p e h T d o o g d e w o h s d n a n a i c i s y h p . e c n a t p e c c a e h t h t i w d e e r g a s t n a p i c it r a p e h T . n o i s i c e d s g u r d c i s a b f o k c a L . F S U e h t t a e g r a h c n i t s i c a m r a h p e h T e h t t a g n i s n e p s i d s g u r d f o d n a h tl a e H f o t n e m t r a p e D p u o r g t n e m e g a n a m e h t . d e t c a t n o c e r e w , d e z i m o t s u c e r e w s g u r d e m o S , e m it e m o s e r i u q e r s r e h t o d n a n o it c a f s it a s s i d g n i s u a c g n i n o it s e u q e h t f o y c a u q e d a n I a e r a l a c i s y h p s 't i n u e h t o t d e d r a w r o f t r o p e R . t n e m t r a p e D l a p i c i n u M e r o m d n a r e d i w a o t e g n a h c A e r a c e h t r o f e c a p s e t a i r p o r p p a s r a e y o w t r e t f a , d e d i v o r p s a w . g n i n o it c n u f f o fl a h a d n a
The continuous crisis in the health sector
interferes in the care process and quality in an important way. In spite of the advanced technology
existing for health and life preservation and the
existence of laws and principles ensuring people’s rights, the fact that they are not made effective and
the population’s suffering are seen as consequences.
The population questioned the inadequacy of the physical area, due to the waiting room’s exposure
to sunlight in the afternoon, causing discomfort,
especially on hot days. The team also appoints
discomfort with the size of the meeting room, location and size of the vaccination room, lack of appropriate
space to perform inhalation therapy and insufficient
number of offices, especially for residents and students visits. After insistent claims of the community together
with the team, the site was changed, improving the
quality of care and users’ satisfaction.
In one of the meetings, satisfaction with the
connection and respect developed were indicated. This
was discussed in a team meeting, and was considered
a motivation and stimulation to work. Additionally, as
a way to expand the community’s participation in the
improvement of team work, a suggestion box was used
for the people to contribute to the development of
activities. The team collects the suggestions on a weekly
basis and discusses them in the meetings. In some
cases, the subject is discussed in community meetings.
The team members change, in some cases
for personal reasons, and in others due to the
managers’ needs. This was another theme of
discussion with the community. Even though some
losses were identified, this need was understood.
The discussions regarding material and human
resources seem to reinforce the bond and complicity
in the search for alternatives viewing to meet the
needs, although they have not always been met.
The organization of the healthcare service
structure, even if represents the first step in the search
for healthcare quality, guarantees a satisfactory
process and results.
FINAL CONSIDERATIONS
To reach the full exercise of citizenship in the
search for worthy living conditions represents a challenge
to the healthcare professionals and the community. The
great advance in the team meetings with the community,
whose minutes were analyzed in this study, represent
the elaboration of a democratic and humanitarian
system, aimed at improving people’s quality of life.
The theme classified from the records of these
team-community meetings - “material and human
resources”, “access to more complex health services”,
“community adherence to the activities provided by
the unit” and “health promotion and disease
prevention” - permit the understanding that the
population and the team are seeking new alternatives
to make health easier, through the proposals aimed
at changing the health/disease concept. To obtain the
community’s involvement in the actions is an important
step to achieve the goals.
Despite the low population participation,
different subjects are discussed, promoting
co-responsibility among the different actors involved in
the process, contributing to improve care quality.
Additionally, the meetings have constituted a space
for information exchange and search for joint solutions.
In the meetings, complicity, trust and respect
have been established between the community and
the team, which start to face together the limitations
imposed by the current health policy, whose difficulties
seem to be more evident for those who are at the
system’ “front door”.
However, the discussions still show
characteristics of information sharing with little decision
power, as they are still centralized, and the population
needs to wait for the right time for decisions about
the requests.
The need to advance in this construction is
observed, in a way that the population understands
the right to act in the co-management of the health
system through effective participation in decision
processes and claims, more consciously and with more
political strength.
We believe that the population must be
encouraged and well received by the team to extend
its participation, as illustrated by the relevance of the
contributions and the reinforcement in the team’s
decision making, in addition to the bond established.
It is expected that the meetings constitute an
increasing participation process in the development of
team work and obtain a care that meets the real needs
of the population and achieves their actual participation.
REFERENCES
1. Viana V. A universidade e o controle social do Sistema Único de Saúde no Estado de Pernambuco. Cad Extensão: saúde [periódico online]. [acessado 2005 outubro 11]. Disponível em: http://www.proext.ufpe.br/cadernos/saude/controle.htm 2. Constituição 1988 (BR). Constituição: República Federativa do Brasil.Brasília (DF): Centro Gráfico do Senado Federal; 1988. Art. 196-200, p. 133-4: Da saúde. 3. Briceño-León R. El contexto político de la participación comunitaria en América Latina. Cad Saúde Pública 1998;14(supl2):141-7.
4. Crevelim MA. Participação da comunidade na equipe de saúde da família: é possível estabelecer um projeto comum entre trabalhadores e usuários?. Cienc Saúde Coletiva 2005 abril-junho; 10(2):323-31.
5. Rodrigues CG. Democracia Y participation cidadana: em busca de la equidad de nuevos recursos?. Rev Mex Sociol 1994; 3:192-204.
7. Matumoto S. Encontros e desencontros entre trabalhadores e usuários na saúde em transformação: um ensaio cartográfico do acolhimento. [Tese] Ribeirão Preto (SP): Escola de Enfermagem de Ribeirão Preto/USP; 2003.
8. Carvalho MCAA. Participação social no Brasil hoje. São Paulo (SP): Polis; 1998.
9. Bardin L. Análise de conteúdo. Lisboa: Edições 70; 1979. 10. Merhy EE. E daí surge o PSF como uma continuidade e um aperfeiçoamento do PACS. Interface Comun Saúde Educ 2001 agosto; 5(9):147-9.
11. Cecílio LCO. Modelos tecno-assistenciais em saúde: da pirâmide ao círculo, uma possibilidade a ser explorada. Cad Saúde Pública 1997 julho-setembro; 13(3):469-78. 12. Silveira LMC, Ribeiro VMB. Grupo de adesão ao tratamento: espaço de “ensinagem” para profissionais de saúde e pacientes. Interface Comunic Saúde Educ 2004 setembro-2005 fevereiro; 9(16):91-104.
13. Da Matta R. A casa e a rua. Rio de Janeiro (RJ): Guanabara-Koogan; 1991.
14. Nunes MO, Trad LB, Almeida BA, Homem CR, Melo MCIC. O agente comunitário de saúde: construção da identidade desse personagem híbrido e polifônico. Cad Saúde Pública 2002 novembro-dezembro; 18(6):1639-46.
15. Ministério da Saúde (BR). Carta de Ottawa. In: Ministério da Saúde (BR). Promoção da Saúde. Brasília: Ministério da Saúde; 2001. p.13-24.