www.jped.com.br
ORIGINAL
ARTICLE
Prevalence
and
factors
associated
with
vitamin
A
deficiency
in
children
and
adolescents
夽
Rita
de
Cássia
Ribeiro-Silva
∗,
Itaciara
L.
Nunes,
Ana
Marlúcia
Oliveira
Assis
SchoolofNutrition,Post-GraduationPrograminFoodandNutrition,DepartmentofNutritionalSciences,UniversidadeFederal daBahia(UFBA),Salvador,BA,Brazil
Received15October2013;accepted8January2014 Availableonline2June2014
KEYWORDS
VitaminAdeficiency; Riskfactors;
Children; Adolescents
Abstract
Objective: ToidentifytheprevalenceandfactorsassociatedwithvitaminAdeficiency(VAD)in childrenandadolescents.
Methods: Thiswas across-sectionalstudyinvolving546schoolchildren,agedbetween7and 14years,ofbothgenders,enrolledinpublicelementaryschools.Bloodwascollectedfor mea-surementofserumretinol.Theretinolconcentrationinthesampleswasdeterminedbyhigh performanceliquidchromatography(HPLC).Datawerecollectedonanthropometrics,dietary, demographic,andsocioeconomicfactors.Polytomouslogisticregressionwasusedtoevaluate theassociationsofinterest.
Results: Approximately27.5%ofthestudentshadretinolvalues<30g/dL.Themultivariate analysisshowed,aftertheappropriateadjustments,apositiveandstatisticallysignificant asso-ciationofmoderate/severeVAD(OR=2.19;95%CI1.17to4.10)andmarginalVAD(OR=2.34; 95%CI1.47to3.73)withage<10years.TherewasalsoassociationofVADmoderate/severe (OR=2.01;95%CI1.01to5.05)andborderlineVAD(OR=2.14;95%CI:1.08to4.21)withthe anthropometricstatusofunderweight.Lowerintakeofretinolwasdetectedamongthosewith severeVAD.
Conclusion: VADisahealthconcernamongchildrenandadolescents.Lowerweightandyounger schoolchildrenhadgreatervulnerabilitytoVAD.
©2014SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
夽
Pleasecitethisarticleas:deCássiaRibeiro-SilvaR,NunesIL,AssisAM.PrevalenceandfactorsassociatedwithvitaminAdeficiencyin
childrenandadolescents.JPediatr(RioJ).2014;90:486---92.
∗Correspondingauthor.
E-mail:[email protected](R.deCássiaRibeiro-Silva). http://dx.doi.org/10.1016/j.jped.2014.01.014
PALAVRAS-CHAVE
Deficiênciade vitaminaA; Fatoresderisco; Crianc¸as; Adolescentes
PrevalênciaefatoresassociadosàdeficiênciadevitaminaAemcrianc¸ase adolescentes
Resumo
Objetivo: IdentificarprevalênciaefatoresassociadosàdeficiênciadevitaminaA(DVA)entre crianc¸aseadolescentes.
Métodos: Estudotransversalenvolvendo546escolares,comidadeentre7e14anos,deambos os sexos,matriculadas na redepública doensino fundamental. Osanguefoi coletado para dosagemdos níveis séricosderetinol. Aconcentrac¸ãode retinoldas amostrasfoi determi-nada pelo método da cromatografia líquida de alta eficiência (CLAE). Coletaram-se dados antropométricos,alimentares,demográficosesocioeconômicos.Utilizou-sedaregressão logís-ticapolitômicaparaavaliarasassociac¸õesdeinteresse.
Resultados: Aproximadamente 27,5% dos estudantes apresentaram valores de retinol<30g/dL. Em análise multivariada, verificou-se, após devidos ajustes, associac¸ão positivaeestatisticamentesignificantedaDVAmoderada/grave(OR=2,19;IC95%:1,17-4,10)e daDVAmarginal(OR=2,34;IC95%:1,47-3,73)comaidade<10anos.Verificou-se,igualmente, associac¸ãodaDVAmoderada/grave(OR=2,01;IC95%:1,01-5,05)eDVAmarginal(OR=2,14; IC 95%: 1,08-4,21) com o estado antropométrico magreza. Menor consumo de retinol foi detectadoentreaquelescomDVAgrave.
Conclusão: AdeficiênciadevitaminaAconfigura-secomoumproblemadesaúdepreocupante entreosescolareseadolescentes.Constatou-semaiorvulnerabilidadedosescolaresdebaixo pesoemaisjovensàDVA.
©2014SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
VitaminAdeficiency(VAD)isanutritionaldeficiencyofhigh magnitudethatcanbecausedbyinsufficientintakeof vita-minAfoodsourcesorbyvitaminabsorption,transport,or metabolismproblems.Theimportanceofadequatevitamin A nutritionalstatus is indisputable, asit has verydiverse physiologicalrolesinthevisualprocess,intheintegrityof epithelial tissue and immune system, aswell as in other metabolicfunctions.1
VAD specifically affects populations subjected to poor living conditions, in addition to other factors related to morbidity conditionsthatalsocontribute toserumretinol depletion. Among them are infections that increase the necessity or stimulate endogenouslosses of this nutrient, andprotein-energymalnutrition,whichaffectsthesynthesis ofretinolbindingprotein(RBP),therebydecreasingretinol availability.2
Children at preschoolage, pregnantwomen, and nurs-ingmothersareregardedastheclassicriskgroup.However, studieshaveindicatedotherpossibleriskgroupsforthe defi-ciency;amongthesearechildrenandadolescents.Sinceit isinvolvedingrowthandphysicaldevelopment,vitaminA alsobecomesessential at thisstage.1,3 The results of the
few studies available in the Brazilian literature generally indicatethatVADprevalencerangesfrom6.8%to34.0%in thispopulation.3
Sincetheyarenotclassicallyconsideredasariskgroup, therearenotmanystudiesonvitaminAnutritionalstatusin schoolchildren(includingadolescents),whichhasprevented aproperassessmentoftheactualmagnitudeofVADinthis
agegroupinBrazil.Therefore,thepresentstudyaimedto estimatethe prevalence of VAD and associatedfactors in childrenand adolescentsenrolledin public schoolsin the cityofSalvador,stateofBahia,Brazil.
Methods
Thiswasacross-sectionalstudyinvolving studentsofboth genders,aged7-14years.Participantswereidentifiedfroma broaderstudythataimedtoidentifyfactorsassociatedwith iron-deficiencyanemiainchildrenandadolescentsenrolled inpublicschoolsinthecityofSalvador.4
The original studysampling procedure involved a com-plexstudydesign,consideringthestratificationofschoolsat twolevels(stateandmunicipal),followedbycluster samp-lingprocedureinthreephases:thefirstphaseassessedthe healthdistricts;thesecond,theschools;thethird,the stu-dents.Duetologisticalfieldissues,theinformationonthe selectedstudentswasobtainedfromsixofthe12existing districtsinSalvador,acitythathas117stateand173 munic-ipal schools. The state schools had 58,059 students; the municipalschools, 56,555.To meetthepreviouslydefined sample size,it wasnecessary toselectten students from eachofthe58municipalschoolsand23studentsfromeach ofthe27stateschools,totaling1,200students.
basedontheprevalenceofinadequateVADidentifiedinthis study(27.5%),thepreviouslyusedsample numberallowed for the determination of the factors associated with the studiedoutcomewitherrorupto2.75%,consideringthe95% levelofconfidence.
Responsevariable
Serumretinolmeasurement
Blood samples (5mL) were collected in the early morn-ing,withthechildinfastingcondition,throughperipheral venipuncture using a disposable needle and syringe. The samples werestored in dry,clear tubes, wrapped in alu-minumfoiltominimizelossesduetolight exposure.After clotretractionandseparationbycentrifugation(1,500rpm for 10min), serum samples were packed and sent tothe Laboratory of theSchool of Nutrition of the Universidade FederaldaBahiafor serumretinolmeasurement.The pro-cedureswerestandardizedusingnationalandinternational references. The routine quality control recommended by theInternationalVitaminAConsultativeGroup(IVACG)was used.5Allhandlingofbloodsamples,fromcollectiontothe
laboratory determinations, were performed in a low-light environment.
Serumretinolextractionwasperformedasproposedby theIVACG.5Sampleretinollevelsweredeterminedusingthe
high-performanceliquidchromatography(HPLC)method.A reversephasesystemwasused,followedbyPDAdetection at325nm.AnAlliance2695Waterschromatograph(Waters Technologies do Brasil, SP, Brazil) was used in the study, coupledtoaWaters2998photodiodearraydetector(PDA) (WatersTechnologiesdoBrasil,SãoPaulo,Brazil).The anal-ysiswasdevelopedusingXTerraMSC18(WatersTechnologies do Brasil, São Paulo, Brazil) columns and 5m pore size
(150mmx3.9mm),protectedbyaC18guardcolumn. The chromatographprogressedinisocraticelution with 100%methanolmobilephase(1mL/min).Theretentiontime ofretinolwas2.4min.Theidentificationandquantification ofserumretinolinthesampleswasestablishedby compar-isonwith the retention time andthe respective standard areaatawavelengthof325nm.Theaccuracyofthemethod wasassessedthroughanextractionrecoverytest,with95% recoveryofretinolacetate(internalstandard)addedtothe samples.Theaccuracywasevaluatedbythereproducibility test,inwhichtriplicatesofthesamesampleweremeasured forretinolforthreealternatedays.Thevaluesfoundshowed avariationoflessthanonestandarddeviation.Thestandard curvewasperformed withall-trans retinolstandard refer-ence(Sigma)atdifferentconcentrations.
The limits of detection and quantification were based on the standard curve linearity, showing values of 0.82g/dL and 2.74g/dL, respectively. The values
of serum retinol were categorized into three levels: severely/moderatelydeficient(< 20g/dL),borderline (≥
20g/dLand<30g/dL),andadequate (≥30g/dL)
(ref-erencecategory).6
Anthropometricstudy
Anthropometricdatawerecollectedintheschool environ-ment by qualified evaluators and interviewers previously trained for data collection. Weight was measured with
a microelectronic Marte scale, model PP 200-50 (Marte Balanc¸aseAparelhosdePrecisãoLtda.,SãoPaulo,Brazil), withcapacity of199.95kgand50gprecision. To measure height, aLeicester stadiometer (Height Measure,London, England)wasused,graduatedintenthsofcentimeters.All measurements were performed following the procedures recommended by theanthropometric standardization ref-erencemanual.7
Toevaluatetheanthropometricstatus,theWorldHealth Organization(WHO)8tableswereusedasthestandard
ref-erence based on percentile values of body mass index (BMI=weight [kg] / height[m]2) for age and gender. The
WHO9 classification was used to define underweight (<
3rd percentile),normalweight (≥ 3rd percentileand<85th percentile),overweight(≥ 85th percentile and<97th per-centile),andobesity(≥97th percentile).
The student’s age was obtained from the database of the State and Municipal Education Secretariats and con-firmedbythedateofbirthinthebirthcertificateoridentity card.
Foodconsumption
The 24-hour recall method was used to determine food consumption.Thecalculationofthedietcentesimal compo-sition was madeusing the Virtual Nutri software,release 1.0, developedby the Departmentof Nutrition,School of PublicHealthoftheUniversidadedeSãoPaulo(SãoPaulo, Brazil).10Retinolintakewasstratifiedaccordingtotertiles:
the 1st tertile was considered asthe lower consumption. Theothertertileswerecharacterizedbyhigherconsumption (referencecategory).
Demographicandsocioeconomicvariables
The demographic variables weregender (male [reference category],female):andage(<10years,>10years [refer-encecategory]):
Thecharacteristicsofenvironmentalandhousing condi-tions, socioeconomicstatus, andmaternal schooling were collectedthroughquestionnairesansweredbythestudents’ parents or guardiansand appliedby trainedandqualified interviewers.Theparents/guardianswereinvitedtocome to the school for interviews. Data on the characteristics of the household (ownership of residence, type of con-struction,predominant material offloor coveringand the predominant construction material, and number of peo-pleperbedroom,amongothers)andsanitationconditions (water supply,garbagecollection, sewage)were obtained forthecreationofanappropriateindexadaptedfromthe modelproposedbyIsslerandGiugliani.11
Everysituationwasassignedascore;themostfavorable receivedascoreof0;themostunfavorable,ascoreof1.The sumofthesevaluescharacterizedtheindicatorof environ-mentalandlivingconditions.Theindexwasclassifiedinto twostrata, having ascutoffthe median: adequate (score ≤4[referencecategory])andinadequate(score>4).
StatisticalAnalysis
TheEpiInfosoftware,release6.04(CentersforDisease Con-trol andPrevention, Atlanta, UnitedStates) was usedfor data processing and database creation using double data entry, after reviewing the questionnaires and correcting errorscausedbythecodificationinitiallyperformedinthe field.
Populationcharacteristicswereidentifiedbydescriptive analysisusing prevalence for categorizeddata, and mean andstandarddeviationforcontinuousvariables.
Serum retinol values categorized in three levels were usedastheoutcome:levelofsevere/moderateretinol defi-ciency(<20g/dL),borderline(≥20g/dLand<30g/dL),
andadequate(≥30g/dL)(comparisoncategory).The
poly-tomouslogisticregressiontechniquewasappliedtoassess factors associated withVAD. The strength of the associa-tionswasexpressedasoddsratio(OR)andrespective95% confidenceintervals(95%CI).
The analysiswasinitiated byperformingtheunivariate polytomous logistic regression analysis to investigate the association of each of the covariates in outcome occur-rence.VariablesassociatedwithVADof20%wereselected forinclusioninthemultivariateanalysis.Forselecting varia-blesin thefinalmodel,thephasing procedure(backward) was adopted. In the adjusted model, only variables with p<0.05wereincluded.
Variables associated with 20% VAD were selected for inclusion in the multivariate analysis. The backward pro-cedure wasusedfor theselectionof variablesinthefinal model.Only thosevariableswithp<0.05 remainedin the adjustedmodel.
Statisticalanalyseswereadjustedforthecomplex sam-pledesign, by usingthesvy commandsinStata software, release9.0(StataCorp,CollegeStation,UnitedStates).
Ethicalquestions
The study protocol was submitted to the Ethics Commit-teeoftheInstitutodeSaúdeColetiva oftheUniversidade FederaldaBahia,whichevaluatedandapprovedits perfor-mance.
Results
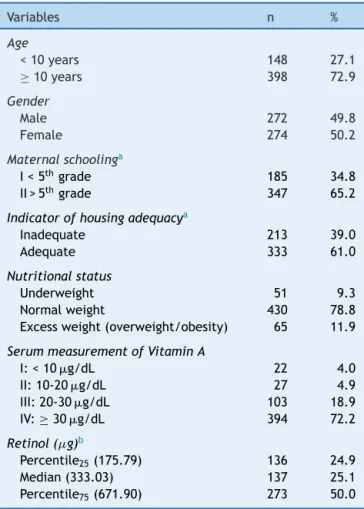
Ofthetotalnumberoftheinitiallyselectedstudents(600), 54 did not participate in the study (due to refusal, fam-ily moving to another city, or transfer of the student to anotherschool),totaling546studentsaged7to14years, witha slightly higherpercentage of females (50.2%).The other characteristics are shown in Table 1. Although the study population is originally from another study,no sta-tistically significant differencewasobserved between the sociodemographiccharacteristicsoftheoriginalsampleand thesubsampleusedinthisstudy(datanotshown).
The frequency distributionof mean serum retinol val-uesshowedsomedegreeofasymmetry;thedeviationwas morepronouncedtotheleft,suggestingahighpercentage ofchildrenandadolescentswithlowmeanserumretinol lev-els(mean=39.6±19.25g/dL).Theprevalenceof27.8%of
VAD(<30g/dL)wasobservedamongtheschoolchildrenand
Table1 Characteristicsofthestudypopulation.Salvador, BA,Brazil,2009.
Variables n %
Age
<10years 148 27.1
≥10years 398 72.9
Gender
Male 272 49.8
Female 274 50.2
Maternalschoolinga
I<5thgrade 185 34.8
II>5thgrade 347 65.2
Indicatorofhousingadequacya
Inadequate 213 39.0
Adequate 333 61.0
Nutritionalstatus
Underweight 51 9.3
Normalweight 430 78.8
Excessweight(overweight/obesity) 65 11.9
SerummeasurementofVitaminA
I:<10g/dL 22 4.0
II:10-20g/dL 27 4.9
III:20-30g/dL 103 18.9
IV:≥ 30g/dL 394 72.2
Retinol(g)b
Percentile25(175.79) 136 24.9
Median(333.03) 137 25.1
Percentile75(671.90) 273 50.0
SD,standarddeviation.
a missingdata.
b meanretinol,
g,(±SD)=960.06(±2,418.89).
ofthese,4.0%wascharacterizedbysevere(<10g/dL),and
4.9%bymoderatedeficiency(≥10g/dLand<20g/dL).
The univariate analysisshowed a positive and statisti-callysignificantassociation betweenmoderatesevereVAD and age<10 years (OR=2.20, 95% CI: 1.18 to 4.10) and underweight(OR=2.09,95%CI:1.02to5.08).Moreover, bor-derlineVADwasassociatedwithage<10 years(OR=2.29, 95%CI:1.45 to3.64) andunderweight (OR=2.14, 95%CI: 1.10 to 4.17). Regarding the other variables, no distinc-tivedistributionwasobservedregardingserumretinollevels (Table2).
The multivariate analysis confirmed, after appropriate adjustments, a positive and statistically significant asso-ciation between moderate/severe VAD(OR=2.19,95% CI: 1.17to 4.10) andborderline VAD(OR=2.34, 95% CI:1.47 to3.73)withage<10years.Therewasalsoanassociation betweenmoderate/severe(OR=2.01,95%CI:1.01to5.05) andborderline VAD (OR=2.14, 95% CI: 1.08 to4.21) with underweight(Table3).
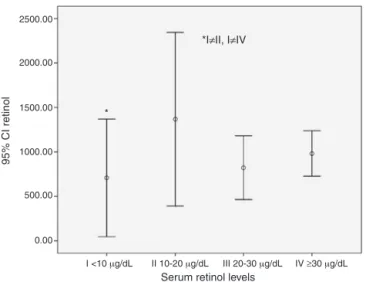
Alowerretinolconsumptionvaluewasdetectedamong those with severe VAD (serum retinol levels<10g/dL)
Table2 ORraw andrespective95%confidenceintervals(95%CI)oftheassociationbetween vitaminA deficiency(VAD)and selectedvariablesinchildrenandadolescentsfrompublicschoolsinthecityofSalvador,BA,Brazil,2009.
Variables Univariatemodel
(moderate/severeVAD)a
Univariatemodel (borderlineVAD)a
OR 95%CI OR 95%CI
Age
<10years 2.20 1.18-4.10 2.29 1.45-3.64
≥10years Reference Reference
Gender
Male 0.93 0.54-1.68 0.91 0.59-1.41
Female Reference Reference
Maternalschooling
<5thgrade 0.91 0.48-1.73 1.09 0.69-1.72
≥5thgrade Reference Reference
Indicatorofhousingadequacy
Inadequate 1.14 0.79-1.65 1.07 0.81-1.40
Adequate Reference Reference
Nutritionalstatus
Underweight 2.09 1.02-5.08 2.14 1.10-4.17
Normalweight+excessweight Reference Reference
RetinolA(g)
<1sttertileofconsumption(231.94) 0.97 0.35-1.33 0.89 0.56-1.41
≥1sttertileofconsumption Reference Reference
OR,oddsratio.
aAdequatelevelsofvitaminA:retinollevels≥30
g/dL(comparisongroup).
Discussion
Theprevalenceoflowserumretinollevels(<20g/dL)was
approximately9.0%(95%CI:6.5to11.3),characterizingVAD asa minor public health problem, according to the WHO criteria.1 This result is consistent with that observed by
Gonc¸alves-Carvalhoetal.12(10.7%)inCampinas,SP,Brazil;
andlowerthanthatidentifiedbyGraebneretal.13(33.55%)
inBrasília, DF,Brazil. Conversely, 18.5%(95% CI:15.23 to 21.19)ofchildrenandadolescentsshowedborderlinelevels (20-30g/dL)ofserumretinol.
Thus,27.5%ofstudentsenrolledinpublicschoolsin Sal-vador, state of Bahia, Brazil, showed inadequate retinol levels(<30g/dL);ahigherpercentagethanthatfoundby
de Souza Valente daSilvaet al.14 (10.0%)in a study
con-ductedin Rio deJaneiro, RJ, Brazil. This is the cutoff(< 30g/dL) that is beingused withincreasingfrequency to
defineVADinschoolchildren,includingadolescents.3,6 Itis
noteworthy that thiscutoff hasbeen inter-validated with thetherapeutictest(+S30DR)andwithRDR,15 inaddition
toshowinganassociationwithvisualfunctionalterations.16
The present study was performed to investigate fac-torsassociatedwithVAD.Itwasobservedthatunderweight
Table3 ORadjustedandrespective95%confidenceintervals(95%CI)oftheassociationbetweenvitaminAdeficiency(VAD)and selectedvariablesinchildrenandadolescentsfrompublicschoolsinthecityofSalvador,BA,Brazil,2009.
Variables Multivariatemodel
(moderate/severeVAD)a
Multivariatemodel (borderlineVAD)a
adjustedOR 95%CI adjustedOR 95%CI
Age
<10years 2.19 1.17---4.10 2.34 1.47---3.73
≥10years 1 1
Nutritionalstatus
Underweight 2.01 1.01---5.05 2.14 1.08---4.21
Normalweight+excessweight 1 1
OR,oddsratio.
aAdequatelevelsofvitaminA:retinollevels≥30
2500.00
2000.00
* 1500.00
1000.00
500.00
0.00
I <10 μg/dL II 10-20 μg/dL III 20-30 μg/dL *I≠II, I≠IV
IV ≥30 μg/dL
95% CI retinol
Serum retinol levels
Figure 1 Mean valuesof retinol consumption according to serum retinol levels inchildren andadolescents from public schoolsinthecityofSalvador,BA,2009.
95%CIRetinol,confidenceinterval(95%CI)forthemeanretinol level.
resultedina2.01-fold(95%CI:1.01to5.05)greaterchance ofschoolchildrenhavingmoderate/severeVADand2.14-fold (95%CI:1.08to4.21)greater chanceofhavingborderline VAD.
These results corroborate those described in other studies,13,17,18 whichisajustifiedassociation,as
malnutri-tionmakestheindividualvulnerabletomultiplenutritional deficiencies. It should be noted that although the preva-lenceofchildhoodmalnutritionhasdeclinedgloballyover thepastfewdecades,thisreductionhasoccurredunevenly and the problem has persisted in some countries.19 It
hasbeen estimated thatin Brazil, amongschool-age chil-dren,thedescribedprevalenceofmalnutritionassessedby weight/heightindex,isapproximately6.8%,andamong ado-lescents, assessed by BMIfor age, is approximately 3.4%, varyingaccordingtoincomestrata.20
Itwasalsoobservedthatschoolchildrenaged<10years presented a 2.19-fold greater chance of having moder-ate/severeVAD(95%CI:1.17to4.10)anda2.34-fold(95% CI: 1.47-3.73) greater chance of having borderline VAD. These results areconsistent withthoseobserved in other studies,21,22 suggesting greater vulnerability of younger
schoolchildren.Itis possiblethat thistrendoccursdueto physicalgrowth,adverseeffectsofvirusandbacterial infec-tions, as well as parasitic infections common in this age group,orevenduetothegreaterdiversificationofdietary patternobservedin olderchildren.Inagreementwiththe findingsbyRamalhoetal.,22althoughthefrequencyoflow
serumretinollevelstendstodeclinewithage,asobserved inthisstudy,itisstillhighenoughtowarrantattentionto thispopulationsegment.
Although the low consumption of foods rich invitamin Awasnotacomplementaryinformationintheexplanatory VADmodel,lowretinolintakewasverifiedamongpatients withsevere VAD when consumption was comparedto the otherlevelsofdeficiency. Theperceptionoftheinfluence ofvitaminAintakeonserumretinollevelshasbeenshared bysomestudies.17,23
Inadequate dietary habits can greatly influence the onset of nutritional deficiencies, particularly in children and adolescents.24 Thus, at a time when an epidemic of
overweight/obesity is emerging, there are still endemic nutritionaldeficiencies,suchasVADandanemiainseveral areasoftheBrazil.25Suchpictureisexplained,inpart,by
theadoptionofunhealthyeatinghabits, especiallyamong youngerindividuals,whichindicatesthenecessityof imple-mentingpublicstrategiestostoptheadvanceofnutritional disordersandtheircomplicationsinthislifecycle.
It is important toemphasize that the main study lim-itation is its cross-sectional design, which affects the interpretationofresults;itsdesignallowsonlyforthe obser-vation of associations between the studied events; it is not possible to demonstrate a cause and effect associa-tionbetweenthem.Thepresentstudy,althoughconsistent withitspurpose,andhavingusedaprobabilisticsampleof adequatesizeandinternationallyrecommendedlaboratory techniques,hasthelimitationoflackofdataregarding gas-trointestinaland respiratory infections, which reduce the absorptionandconsiderablyincreasethebiological utiliza-tionandexcretionofthismicronutrient,regardlessofliver reserve.1Moreover,datawerenotobtainedonclinicalsigns
ofVAD.26
Additionally,the24-hourrecallmethodusedinthisstudy toinvestigate food intake also has some limitations. The food intake investigation, in addition tobeing limited to dataonvitaminAconsumption,withoutinformationonthe absorption and biological utilization, has received heavy criticismduetotheextremevariabilityonthemeasurement ofthisvitaminfromfoodsources,aswellasthemultiplicity oftables,oftenwithoutadequateinformationoncontentof regionalfoodsconsumedbythetargetpopulation.However, thismethodprovidesinformationontheestimatedaverage intakeofpopulations,evenwhenappliedonlyonce,when themethodologicalassumptionsareobservedandanalytical resourcesareappropriate.27 Thus,foodconsumption
stud-iescanprovideimportantinformation,atanearlystage,on theriskofnutritionaldeficiency,beforetheclinicalformis established.
VADisanimportanthealthprobleminchildrenand ado-lescents.AgreaterVADvulnerabilitywasobservedinlower weightandyoungerchildren.Theschoolhasanimportant roleinVADpreventionbypromotingnutritionaleducation, aimedparticularlyatriskgroups.
Funding
Fundac¸ãodeAmparoàPesquisadoEstadodaBahia(Fapesb; process No. 1431040053551) and Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq; process No.402462/2005-0).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
2.Lee RD, Nieman DC. Nutritional assessment. London: WCB McGrawHill;1993.
3.RamalhoA,PadilhaP,SaundersC.CriticalanalysisofBrazilian studiesaboutvitaminAdeficiencyinmaternal-childgroup.Rev PaulPediatr.2008;26:392---9.
4.BorgesCQ,SilvaRdeC,AssisAM,PintoEdeJ,FiacconeRL, PinheiroSM.Factors associatedwith anemiain childrenand adolescentsin publicschools inSalvador,Bahia State. Brazil CadSaudePublica.2009;25:877---88.
5.InternationalVitaminAConsultativeGroup(IVACG).TheAnnecy Accords toassessand controlvitaminAdeficiency:summary ofrecommendationsandclarifications.Washington,DC:IVACG; 2003.
6.World Health Organization (WHO). Indicators for assessing vitamin Adeficiency and theirapplicationinmonitoring and e valuating intervention programmes: micronutrient series. Geneva:WHO;1996.
7.LohmanTG,RocheAF,MartorellR.Anthropometric standard-izationreferencemanual.Illinois:HumanKineticsBooks;1988. p.1---124.
8.deOnisM,OnyangoAW,BorghiE,SiyamA,NishidaC,Siekmann J.DevelopmentofaWHOgrowthreferenceforschool-aged chil-drenandadolescents.BullWorldHealthOrgan.2007;85:660---7.
9.WHOMulticentreGrowthReferenceStudyGroup.ChildGrowth Standards:length/height-for-age,weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: methodsanddevelopment.Geneva:WHO;2006.
10.Philippi ST, Szarfarc SC, Laterza CR. Virtual Nutri - v.1 for Windows.In:SistemadeAnáliseNutricional.SãoPaulo: Depar-tamentodeNutric¸ão,FaculdadedeSaúdePública,Universidade deSãoPaulo;1996.
11.IsslerRM,GiuglianiER.Identificac¸ãodegruposmaisvulneráveis àdesnutric¸ãoinfantilpelamedic¸ãodoníveldepobreza.J Pedi-atr(RioJ).1997;73:101---5.
12.Gonc¸alves-CarvalhoCM,Amaya-FarfanJ,WilkeBC,Vencovsky R. Prevalence ofhypovitaminosis A inchildrenof peripheral districts of Campinas, São Paulo. Brazil Cad Saude Publica. 1995;11:85---96.
13.GraebnerIT,SaitoCH,deSouzaEM.Biochemicalassessmentof vitaminAinschoolchildrenfromaruralcommunity.JPediatr (RioJ).2007;83:247---52.
14.de Souza Valente da Silva L, Valeria da Veiga G, Ramalho RA. Association of serum concentrations of retinol and
carotenoidswithoverweightinchildrenandadolescents. Nutri-tion.2007;23:392---7.
15.FloresH,AzevedoMN,CamposFA,Barreto-LinsMC,Cavalcanti AA,SalzanoAC,etal.SerumvitaminAdistributioncurvefor childrenaged2-6yknowntohaveadequatevitaminAstatus: areferencepopulation.AmJClinNutr.1991;54:707---11.
16.SaundersC,doCarmoLealM,GomesMM,CamposLF,dosSantos SilvaBA,ThiapódeLimaAP,etal.Gestationalnightblindness amongwomenattendingapublicmaternityhospitalinRiode Janeiro.BrazilJHealthPopulNutr.2004;22:348---56.
17.CaoJ,WeiX,TangX,JiangH,FanZ,YuQ, etal.Effectsof eggandvitaminAsupplementationonhemoglobin,retinol sta-tusand physicalgrowth levelsofprimary and middleschool students inChongqing,China. AsiaPacJ ClinNutr.2013;22: 214---21.
18.SommerA.Vitaminadeficiencyandclinicaldisease:an histor-icaloverview.JNutr.2008;138:1835---9.
19.WorldHealthOrganization(WHO).WorldHealthStatistics2010. Geneva:WHO;2010.
20.InstitutoBrasileirodeGeografiaeEstatística(IBGE).Pesquisa deOrc¸amentoFamiliar2008-2009.In:Antropometriaeestado nutricionaldecrianc¸as,adolescenteseadultosnoBrasil.Riode Janeiro:IBGE;2010.
21.BreidenasselC,Valtue˜naJ,González-GrossM,BenserJ, Spin-nekerA, MorenoLA, et al.Antioxidantvitamin status(A,E, C,and beta-carotene)inEuropeanadolescents- theHELENA Study.IntJVitamNutrRes.2011;81:245---55.
22.RamalhoRA,SaundersC,NataliziDA,Cardoso LO,AcciolyE. Serumretinollevelsinschoolchildren,7to17yearsoldinRio deJaneiro,Brazil.RevNutr.2004;17:461---8.
23.AhmedF,Rahman A, NoorAN, AkhtaruzzamanM, HughesR. AnaemiaandvitaminAstatusamongadolescentschoolboysin DhakaCity,Bangladesh.PublicHealthNutr.2006;9:345---50.
24.Davison KK, Birch LL. Childhood overweight: a contextual model and recommendations for future research. Obes Rev. 2001;2:159---71.
25.Batista Filho M, Rissin A. Nutritional transition in Brazil: geographic and temporal trends. Cad Saude Publica. 2003;19:S181---91.
26.DinizAS,SantosLM.HipovitaminoseAexeroftalmia.JPediatr (RioJ).2000;76:S311---22.