REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
The
prognostic
value
of
cerebral
oxygen
saturation
measurement
for
assessing
prognosis
after
cardiopulmonary
resuscitation
Mehmet
Turan
Inal
a,∗,
Dilek
Memis
¸
a,
Ilker
Yıldırım
b,
Hüseyin
U˘
gur
a,
Aysegul
Erkaymaz
a,
F.
Nesrin
Turan
caTrakyaUniversityMedicalFaculty,DepartmentofAnesthesiology,Edirne,Turkey bUzunkopruGovermentHospital,DepartmentofAnesthesiology,Edirne,Turkey cTrakyaUniversityMedicalFaculty,DepartmentofBioistatistic,Edirne,Turkey
Received14October2015;accepted20July2016 Availableonline21August2016
KEYWORDS
Cardiopulmonary resuscitation; Cerebraloxygen saturation; Prognosis
Abstract
Background: Despitenewimprovementsoncardiopulmonaryresuscitation(CPR),braindamage isveryoftenafterresuscitation.
Objective: Toassesstheprognosticvalueofcerebraloxygensaturationmeasurement(rSO2) forassessingprognosisonpatientsaftercardiopulmonaryresuscitation.
Design:Retrospectiveanalysis.
Measurementsandresults:We analyzed 25 post-CPRpatients (12 femaleand13 male). All thepatientswerecooledtoatargettemperatureof33---34◦C.TheGlascowComaScale(GCS),
CornealReflexes(CR),PupillaryReflexes(PR),arterialBaseExcess(BE)andrSO2measurements weretakenonadmission.TherewarmingGCS,CR,PR,BEandrSO2measurementsweremade afterthepatient’stemperaturereached36◦C.
Results:In survivors,thebaseline rSO2 value was 67.5(46---70) andthe percentdifference between baseline andrewarming rSO2 value was 0.03 (0.014---0.435). In non-survivors, the baselinerSO2valuewas30(25---65)andthepercentdifferencebetweenbaselineand rewarm-ingrSO2value was0.031(−0.08to−20).Nostatisticaldifferencewasdetected onpercent changesbetweenbaselineandrewarmingvaluesofrSO2.Statisticallysignificantdifferencewas detectedbetweenbaselineandrewarmingGCSgroups(p=0.004).Nostatisticaldifferencewas detectedbetweenGCS,CR,PR,BEandrSO2todeterminetheprognosis.
Conclusion: DespitehighervaluesofrSO2onsurvivorsthannon-survivors,wefoundno statisti-callyconsiderabledifferencebetweengroupsonbaselineandtherewarmingrSO2values.Since
∗Correspondingauthor.
E-mail:[email protected](M.T.Inal). http://dx.doi.org/10.1016/j.bjane.2016.07.016
themeasurementissimple,andnotaffectedbyhypotensionandhypothermia,therSO2may beausefulpredictorfordeterminingtheprognosisafterCPR.
©2016SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVE
Reanimac¸ão cardiopulmonar; Saturac¸ãodeoxigênio cerebral;
Prognóstico
Ovalordamedidadasaturac¸ãocerebraldeoxigênioparaavaliaroprognóstico apósressuscitac¸ãocardiopulmonar
Resumo
Justificativa:Apesardosnovosavanc¸osemreanimac¸ãocardiopulmonar(RCP),odanocerebral muitasvezesocorreapósareanimac¸ão.
Objetivo:Avaliarovalor prognósticodemedirasaturac¸ãodeoxigênio cerebral(rSO2)para estimaroprognósticoempacientesapósareanimac¸ãocardiopulmonar.
Projeto: Análiseretrospectiva.
Medidaseresultados:ForamavaliadosapósRCP25 pacientes(12 dosexofemininoe 13do masculino).Todosospacientesforamsubmetidosàhipotermia(temperaturaalvode33-34◦C).
Asmensurac¸õesdaEscaladeComadeGlascow(GCS),dosreflexoscorneanos(RC),dosreflexos pupilares(RP),edoexcessodebase(EB)erSO2foramfeitasnaadmissão.Nahipertermia,as mensurac¸õesdeGCS,RC,RP,EBerSO2foramfeitasdepoisqueatemperaturaatingiu36◦C.
Resultados: Emsobreviventes,ovalorbasalderSO2foide67,5(46-70)eadiferenc¸apercentual entreovalorbasaleahipertermiaderSO2foide0,03(0,014-0,435).Emnãosobreviventes,o valorbasalderSO2foide30(25-65)eadiferenc¸apercentualentreovalorbasaldehipotermia derSO2 foide 0,031(−0,08-20).Nãohouve diferenc¸aestatística nasvariac¸ões percentuais entreosvalores darSO2nafasebasaledereaquecimento.Uma diferenc¸aestatisticamente significativafoiobservadaentreosvaloresdaGCSnafasebasaledereaquecimentodosgrupos (p=0,004).Nãohouvediferenc¸aestatisticamentesignificativaentreGCS,RC,RP,EBerSO2 paradeterminaroprognóstico.
Conclusão:EmboraosvaloresdarSO2tenhamsidomaiselevadosemsobreviventesqueemnão sobreviventes,nãoobservamosumadiferenc¸aestatisticamentesignificativadosvaloresdarSO2 entreosgruposnafasebasaledereaquecimento.Comoamensurac¸ãoésimples,enãoafetada porhipotensãoehipotermia,arSO2podeserumindicadorútilparadeterminaroprognóstico apósaRCP.
©2016SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Despite recent improvements in resuscitation strategies, brain damage is very often an event after Cardiopul-monary Resuscitation (CPR) and the outcome remains poor.1---3
The early assessment of neurological outcomes after CPR is important, and there has been a growing inter-est toestimate the prognosis after CPR. In recent years, severalstudies reportedthe predictors of neurologic out-comeinsurvivorsofcardiacarrestsubmittedtotherapeutic hypothermia.4---8
Clinical neurologic examinations such as the Glasgow Coma Scale (GCS), Corneal Reflex (CR), and Pupillary Reflex (PR) tests are very simple methods and widely used. Biomarkers and electrophysiological tests are also used,but withcomplexity.Ina recentstudy,7theauthors
concludedthatpredicting neurologicaloutcomeafter car-diacarrestbybiomarkers,clinical neurologicexamination
and electrophysiological tests can be difficult. In another previous research, the authors reported that absent CR, absent PupillaryLightReflex(PLR), andabsenceof motor responses were strongly related with poor neurological outcomes.9,10 Different studies concluded that clinical
examination should becombinedwith moderntechnology forearlyprognostication.6,7
Monitoringoftheoxygensaturationofthebrainisanew method,andpreviousstudieshavedescribedthatadecrease intheregionalcerebraloxygensaturation(rSO2)isa
valu-able predictorfor postoperativecognitive dysfunction,as well as prolonged Intensive Care Unit (ICU) and hospital stays.11---16Theadvantagesofthismethodarethatthe
mea-surement is not affected by hypothermia or hypotension andthatit cangatherreal-timemeasurementsusingnear infraredspectroscopy.8,16
Theaimofthisstudywastoassesstheprognosticvalue ofrSO2toassessprognosisaftercardiopulmonary
Materials
and
methods
The Regional Ethical Committee approved the study (GOKAEK2013/191).Allnewpost-CPRpatientsadmittedto thegeneral andsurgicalICU whostayed >24h duringa 2-yearperiod(January1,2012 toDecember31,2013) were retrospectivelyenrolled.OurICUsincluded19bedsandthe physicianshadtohaveexperienceinmeasuringGCS,PR,CR, BEandrSO2.
In our study, we used the term cardiac arrest similar tothedefinitionmadebyItoetal.,16 whodefinedcardiac
arrestastheabsenceofspontaneousrespiration,palpable pulse,andresponsivenesstostimuli.
Resuscitation time and resuscitation place (the resus-citation places were divided into emergency department andmedicaldepartments) wererecorded.The illnesswas categorizedtomedicalcardiac,medicalnon-cardiac, surgi-calcardiacandsurgicalnon-cardiac.Comorbidieswerealso recorded.
Age,gender andAPACHEIIscores wereallrecordedon admission.
WeusedthefollowingresponsestocalculatetheGCS,as describedbyTeasdaleetal.17:eyesopeningresponse,
ver-balresponse,andmotorresponse.CRandPRweredescribed as present or absent. GCS,CR and PR were recorded on admission.
WeusedtheCobasb221® (Roche,Mannheim,Germany)
forarterialbloodgasesanalysisandthearterialBaseExcess (BE)wascalculatedautomaticallyaccordingtotheNational Committeefor clinical laboratory standards recommenda-tions.BEvaluewasrecordedonadmission.
TomeasuretherSO2,twosensorswereappliedbilaterally
tothepatients’foreheadafterthepatients’foreheadskin andrSO2weremeasuredbyusingtheINVOS®(Covidien,USA)
deviceonadmission.Lowervalueswererecorded.
Inourdailypractice,weusedhypothermiafor all post-CPR patients.Allthe patientswerecooled to33---34◦
Cby theuseof amattress thatusescoldair andicepacks.By cooling,wewantedtoreachthetargettemperaturewithin 4handmaintainthistemperaturefor24handthenfollow itwithpassiverewarming.Nosedativesweregiventothe patients.
After rewarming, GCS, CR, PR, BE and rSO2
measure-mentswereperformedandrecorded.
During the study, all the patients had a glucose level between 130 and 160mg.dL−1, central venous pressure
12---13mmHgandetC02 34---36mmHg.Ifnecessary,
vasoac-tiveorinotropicsupportwasgiventopatientstomaintain ameanarterialbloodpressure>65mmHg.
PatientswerefollowedupuntildeathorICU discharge. LengthofICUstayandprognosiswererecordedandpatients weredividedintosurvivorsandnon-survivors.
Exclusion criteriawere asfollows:ageunder18 years, historyofirreversiblebraindamageandatraumaticorigin.
Statisticalanalysis
Results are expressed as median (min---max) or number. Normalitydistributionofvariableswastestedusingone sam-pleKolmogorov---Smirnov test. The groups were compared by Mann Whitney U-test for non-normal distributed data.
Categoricalvariableswerecomparedby usingthe Fisher’s Chi-squareandMcNemartest.ROCanalysiswasperformed forGCSbaselineandrewarming,BEbaselineandrewarming, and rSO2 baseline and rewarming. Sensitivity and
speci-ficitywere performed for PR baselineand rewarmingand CR baseline and rewarming. A p-value<0.05 was consid-eredasstatisticallysignificant. MedCalc V13.3.3andSPSS 21statisticalsoftwareswereusedforstatisticalanalyses.
Results
Thirty-eightpatientswereadmittedtotheICUsduringthe studyperiod.Only25 ofthemwereincludedin thestudy. Thirteenpatientswereexcludedbecauseofinadequatedata likeunder18yearsold,ortheyhadsedativeinfusions.Four patientsweredischargedfromtheICUs,while21died.The medianageofthepatients inthesurvivorgroup was65.5 (20---68) years, while it was68 (22---86) years in the non-survivorgroup.TheICUstaysamongthesurvivorslasted7 (7---8) days,while non-survivors stayed for 6 (2---61) days. The resuscitation timefor survivors was27.5 (5---30) min, whileitwas15(10---45)minfornon-survivors.TheAPACHE IIscoreforsurvivorswas23(7---24),whileitwas27(7---33) fornon-survivors.Noconsiderabledifferencewasdetected betweengroupsonage,gender,ICUstay,resuscitationtime andAPACHE II scores (p>0.005) (Table1). One patientin survivor groupand 15patients in non-survivor group used vasoactive or inotropic support. The places of resuscita-tion,theillnesscategoriesandcomorbiditiesareshownin Table1.
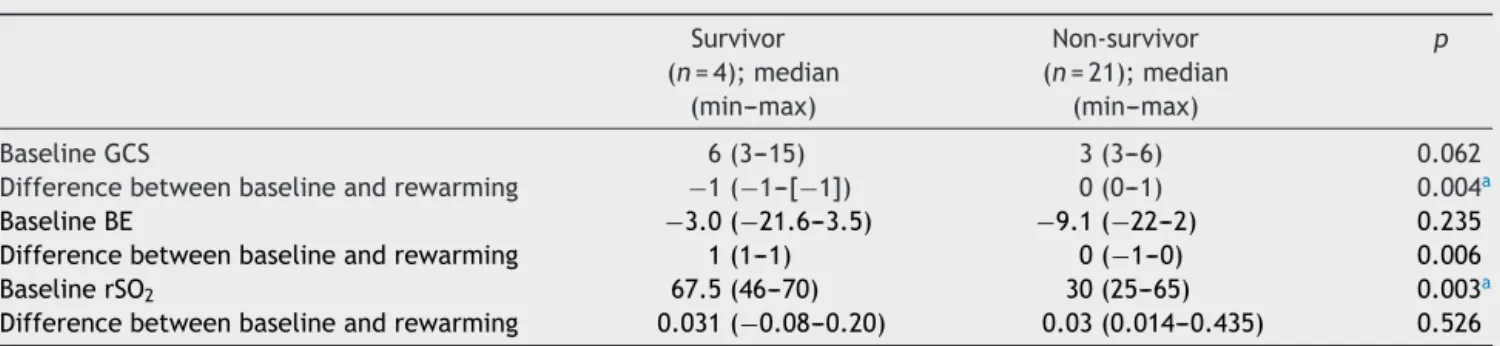
ThebaselineGCSforsurvivorswas6(3---15),whileitwas3 (3---6)innon-survivors,andnostatisticallymajordifference was detected (p=0.062). The percent changes between baselineandrewarmingGCSwasfoundas−1(−1to[−1]) insurvivorsand0(0---1)innon-survivors.Astatistical differ-encewasdetectedbetweenthegroups(p=0.004)(Table2). ThebaselineBEforsurvivorswas−3.0(−21.6to−3.5)and
−9.1(−22to−2)fornon-survivorsandnostatistically con-siderabledifferencewasdetected(p=0.235).Thepercent changesbetweenbaseline andrewarmingBEfor survivors was1(1---1)while0(−1to0)fornon-survivors.Statistically considerabledifferencewasdetected(p=0.006)(Table2). Insurvivors,thebaselinerSO2valuewas67.5(46---70),and
the percent difference between baseline and rewarming rSO2 value was 0.03 (0.014---0.435). In non-survivors, the
baselinerSO2valuewas30(25---65)andthepercent
differ-encebetweenbaselineandrewarmingrSO2valuewas0.031
(−0.08 to .20). Although statistically considerable differ-encewasdetectedbetweengroupsonbaselinerSO2values,
nostatistical differencewasdetected onpercentchanges between baseline and rewarming values of rSO2
(respec-tivelyp=0.003,0.526)(Table2).
Table1 Demographicdata.
Survivor (n=4)
Non-survivor (n=21)
p
Gender(F/M) 1/3 11/10 0.593
Age,median(min---max) 65.5(20---68) 68(22---86) 0.331
ICUstay(day),median(min---max) 7(7---8) 6(2---61) 0.709
Resuscitationtime(min),median(min---max) 27.5(5---30) 15(10---45) 0.497
Resuscitationplaces
Emergencydepartment 4 8
Medicaldepartments 0 13
Illnesscategory
Medicalcardiac 2 9
Medicalnon-cardiac 2 8
Surgicalcardiac 2 0
Surgicalnon-cardiac 1 0
Comorbidities
Cerebrovasculardiseases 1 1
Hypertension 2 9
COPD 1 0
Chronicrenaldisease 1 4
Diabetesmellitus 0 7
Other 0 6
APACHEII(mean±SD);median(min---max) 23(7---24) 27(7---33) 0.110
Dataarepresentedasmedian(min---max).
APACHEII,acutephysiologyandhealthevaluation;ICU,intensivecareunit;COPD,chronicobstructivepulmonarydisease.
Table2 GCS,BEandrSO2values.
Survivor (n=4);median
(min---max)
Non-survivor (n=21);median
(min---max)
p
BaselineGCS 6(3---15) 3(3---6) 0.062
Differencebetweenbaselineandrewarming −1(−1---[−1]) 0(0---1) 0.004a
BaselineBE −3.0(−21.6---3.5) −9.1(−22---2) 0.235
Differencebetweenbaselineandrewarming 1(1---1) 0(−1---0) 0.006
BaselinerSO2 67.5(46---70) 30(25---65) 0.003a
Differencebetweenbaselineandrewarming 0.031(−0.08---0.20) 0.03(0.014---0.435) 0.526
GCS,GlascowComaScale;BE,baseexcess;rSO2,regionalcerebraloxygensaturation. ap<0.005.
Table3 Cornealandpupillaryreflexes.
Survivor (n=4)
Non-survivor (n=21)
pa
baselinePR(+/−) 3/1 6/15 0.116
RewarmingPR(+/−) 0/4b 6/15b 0.540
baselineCR(+/−) 3/1 15/6 0.116
RewarmingCR(+/−) 0/4b 6/15b 0.540
PR,pupillaryreflex;CR,cornealreflex;+,present;−,absent.
PR. No statistically considerable difference wasdetected betweengroups (p=0.540).The PR andCRmeasurements areshowninTable3.Nostatisticallyconsiderabledifference wasdetectedbetweengroupsonbaselineandrewarmingCR (respectivelyp=0.186,0.540).Nostatisticallymajor differ-encewasdetectedbetweenpercentchangesonsurvivorand non-survivorsgroups (respectively p=1.000, 1.000, 1.000, 1.000).ThebaselineandrewarmingmeasurementsofGCS and BE values belonging to the percent changes are cal-culated, in the survivors group, and for GCS the median (min−max) was −1 (−1 to [−1]) and for BE the median was 1 (1---1). In the non-survivors group, for GCS, the median (min---max) was 0 (0---1) and for BE, the median (min---max)was0(−1to0).Statisticallyconsiderable differ-encewasdetected(respectivelyp=0.040,0.006)(Table2). In the survivors group, for rSO2, the median (min---max)
was0.031(−0.08to0.20),andinnon-survivorsgroup,for GCS,themedian(min---max)was0.03(0.014---0.435). Statis-tically considerable differencewasnot detectedbetween thegroups(p=0.526).
TheAreaUndertheCurve(AUC)valuefor baselineGCS was 0.78 withan optimal cut-off point of 5 according to YadenIndex.Thesensitivitywasfoundtobe85.7%andthe specificitywas75%.ThePositivePredictiveValue(PPV)was 94.7%,whiletheNegativePredictiveValue(NPV)wasfound tobe49.9%.Nostatisticallymajordifferencewasdetected (p=0.1114).TheAUCmeasurementfortherewarmingGCS was0.958withan optimalcut-off point of7according to YadenIndex.The sensitivityandspecificitywerefound to be90.4%and100%.ThePPVwas100%,while theNPVwas 66.6%.Astatisticallyconsiderabledifferencewasdetected (p<0.0001) (Table4). The optimalcut-off point for base-line BE was −7.5 according to Yaden Index with 0.69 as an AUCvalue. Thesensitivitywasfound tobe76.19% and thespecificitywas75%.ThePPVwas94.1%,whiletheNPV wasfoundtobe37.5%.Nostatisticallysignificantdifference wasdetected (p=0.390).The AUCvalue forrewarmingBE was0.976withanoptimalcut-offpointof−1.2according toYadenIndex.The sensitivitywas90.4%while specificity was100%.The PPVwas100%,while theNPVwasfoundto be66.7%.Statistically,differencewasdetected(p<0.0001) (Table4).TheAUCvalueforbaselinerSO2 was0.964.The
optimalcut-offpointwasfoundtobe41accordingtoYaden Index.Thesensitivityandspecificitywerefoundtobe90.4% and100%.ThePPVwas100%,whiletheNPVwas66.6%.A statisticallysignificantdifferencewasdetected(p<0.0001). The AUC measurement for therewarming rSO2 was0.976
with an optimal cut-off point of 38 according to Yaden Index.Thesensitivitywasfoundtobe90.4%andthe speci-ficitywas100%.ThePPVandNPVwere100%and66.6%.A statisticallysignificantdifferencewasdetected(p<0.0001) (Table4).
The sensitivityforbaselinePRandCRwas71.4%,while the specificity was22% and 25%. The PPV and NPV were 83.3%and14.3%,respectively(p>0.05).Thesensitivityfor rewarmingPRandCRwas71.4%,whilethespecificitywas0 and100.0%.The PPVwere78.9%and100.0%,andtheNPV were0.0%and40.0%(p=0.508)(Table4).
On comparison of alltests witheach other no statisti-cally considerable difference was detected (respectively; p=0.754,0.508,0.754).
Discussion
We aimed to evaluate the prognostic value of cerebral oxygensaturation measurement to assess prognoses after CPR.Despite highervalues ofrSO2 onsurvivors than
non-survivors,wefoundnostatisticallyconsiderabledifference betweengroupsonbaselineandtherewarmingrSO2values.
Also,nodifferencewasdetectedbetweenothertests. Itoetal.16definedcardiacarrestastheabsenceof
spon-taneousrespiration,palpablepulse,andresponsivenessto stimuli,andwealsousedthisdefinitioninourstudy.
Despite improvements on resuscitation and ICU proto-cols,the rateof survivalwaslow.Peberdy etal.3 carried
outastudyon14,720cardiacarrestpatientsandreported that17%survivedhospitaldischarge.AnotherstudybyGreer etal.7demonstratedagoodoutcomeof9.9%survivalamong
patients.Inourstudy,wefounda16%survivalrate. Therapeutichypothermiaisoneofthetreatment meth-ods for patients surviving cardiac arrest. Therapeutic hypothermia was defined as cooling of the patient to 32---34◦Cfor12---24h.Differentstudiesreportedthe
advan-tages and disadvantages of therapeutic hypothermia.18,19
Due to the uncertain recommendations on therapeutic hypothermia,we routinely used it for ourpatients in our intensivecare.
Outcome prediction is an important component of the managementofpost-CPRpatients.MonitoringGCSisavery useful method and is frequently used in ICUs; moreover, hospitalstaffmembersarewelltrainedincalculatingGCS scores.SeveralpreviousstudiesreportedtheusageofGCS asaprognosticfactorinpost-CPRcriticallyillpatients.10,20
Schefoldetal.10designedastudytoanalyzetheusefulness
ofGCSforoutcomepredictioninsurvivorsofcardiacarrest treatedwiththerapeutichypothermia.TheyfoundthatGCS scoresweresignificantlyhigherinpatientswithagood out-comecomparedwiththosewithan unfavorableoutcome. Theauthorsreportedthatascoreof>3onthemotor com-ponentpointedgoodoutcomeswithaspecificityof100%on thefirstday. Mullieetal.20 suggestedthatthe GCS-based
rulecanbehelpfulinpredictingoutcomesinpatients resus-citatedafterout-of-hospitalcardiacarrest.Inanotherstudy, Bouwesetal.4found thatthemotorscores72hafterCPR
werenotvaluablewhenitcametodeterminingthe progno-sisafterCPR.InareviewbyWijdicksetal.,21theGCSwas
dividedintoamotorpartandbrainstem reflexes,andthe authorsfoundthattheprognosiswaspoorwithabsentPRor CRorabsentorextensormotorresponses3daysafter car-diacarrest.Inourstudy,wecalculatedtheGCStwice.The medianbaselineGCSforsurvivorswas6(3---15),whileitwas 3(3---6)in non-survivors.The percentdifferencesbetween baselineandrewarmingvaluesforGCSwere−1(−1to[−1]) insurvivorsand0(0---1)innon-survivors.
CRandPRhavealsobeenwidelyused.Astudymadeby Greeretal.7demonstratedthatPRmaybeabsent
immedi-atelyafterpost-arrestandmaysubsequently recover.The authorsconcludedthat the absenceof PR and CR onday 3remained highlyvaluable for predicting poor outcomes. Moreover,Bouwesetal.4reportedsimilarresultsand
Table4 Theoptimalcut-off,AUC,sensitivity,specificity,PPVandNPVvalues.
Optimalcut-off AUC (95%CI)
p Sensitivity (95%CI)
Specificity (95%CI)
PPV (95%CI)
NPV (95%CI) RewarmingGCS 7 0.958(0.794---0.999) <0.0001a 90.4(69.6---98.8) 100(39.8---100.0) 100(82.35---100.0) 66.6(18.73---96.88) RewarmingBE −1.2 0.976(0.822---1.000) <0.0001a 90.4(69.6---98.8) 100(39.8---100.0) 100(82.4---100.0) 66.7(22.3---95.7) BaselinerSO2 41 0.964(0,803---0.999) <0.0001a 90.4(69.6---98.8) 100(39.8---100.0) 100(82.35---100.0) 66.6(18.73---96.88) RewarmingrSO2 38 0.976(0.822---1.000) <0.0001a 90.4(69.9---98.8) 100(39.8---100.0) 100(82.4---100.0) 66.6(22.3---95.7) BaselinePR 0.508 71.4(47.8---88.7) 22.0(0.6---80.5) 83.3(58.5---96.4) 14.3(0.4---57.8) RewarmingPR 0.754 71.4(47.8---88.7) 0.0(0.0---60.2) 78.9(54.4---93.9) 0.0(0.0---45.9) BaselineCR 0.508 71.4(43.8---88.7) 25.0(0.63---80.5) 83.3(58.5---96.4) 14.3(0.3---57.8) RewarmingCR 0.754 71.4(47.8---88.7) 100.0(39.7---100.0)100.0(78.2---100.0) 40.0(12.1---73.7) GCS,GlascowComaScale;BE,BaseExcess;rSO2,regionalcerebraloxygensaturation;PR,PupillaryReflexes;CR,CornealReflex;AUC,AreaUnder theCurve;CI,ConfidenceInterval;PPV,PositivePredictiveValue;NPV,NegativePredictiveValue.
ap<0.001.
notareliablefactor.Theauthorsconcludedthatthe possi-bleexplanationoftheirobservationmightbeanoverrating ofthemotorscore.Maiaetal.5enrolled26patientsintheir
studyandreportedthatabsentPLRandabsentCRshowed nofalse-positivesinpredictingpooroutcomes.Inourstudy, inthesurvivorgroup,3patientshadapositivebaselinePLR whileonehadanegativebaselinePLR.Inthenon-survivor group,6patientshadapositivebaselinePLR,while15had anegative baselinePLR. Nostatistically considerable dif-ference was detected between groups. After rewarming, thePLRvalueswereasfollows:Inthesurvivorgroup,zero patientshadapositivePLR,whilefourhadanegativePLR.In thenon-survivorgroup,6patientshadapositivePLR,while 15hadanegativePLR.Nostatisticalmajordifferencewas detectedbetweengroups.Moreover,nostatistically signif-icantdifferencewasdetectedbetweengroupsonbaseline andrewarmingCR.
Monitoringof arterial base excessis usedfor assessing outcome after CPR.22 In their study,Takasu et al.22
mea-suredarterialbase excess afterCPR on87 patients.They reportedsignificantlyhighBEvaluesinthesurvivorsgroup andconcludedthatBEcoulddistinguishsurvivorsfrom non-survivors,butBEwasnotfoundasapredictorformortality inresuscitatedpatients.TheauthorsconcludedthatBE val-ues were well correlated with resuscitation time. In our study,wefoundhigherBEvaluesinsurvivorsinbaselineand rewarmingperiods.
The measurement of the saturation of the brain is a recent method, and previous studies have reported that a decline in the value of rSO2 is a significant predictor
forpostoperativecognitive dysfunctionandprolonged ICU and hospital stays.12---16 The advantage of this method is
thatthedeviceisnotaffectedbyhypothermiaor hypoten-sionandreal-timemeasurementsarecollectedusingnear infrared spectroscopy.17 Murkin et al.15 monitorized brain
oxygen saturation during coronary bypass surgery on 200 patientsand reportedthat patients whohadmajor organ morbidity or mortality had lower rSO2 values. Moreover,
theauthors reportedthat length of hospitalstay and ICU stay was prolonged with lower rSO2 values. They
con-cludedthatinmaneuversduringcoronaryrevascularization surgery, pump flow is often decreased and caused a pro-found decrease in rSO2. The goal of another study made
bySlateretal.11wastodetermineifmaintenanceof
cere-bralperfusionwiththeuseofcerebraloximetrymonitoring
hadanimpactonearlypostoperativeoutcomes.Theauthors demonstratethatintraoperativerSO2desaturationis
signifi-cantlyassociatedwithdemonstrableneurocognitivedecline inaprospectivelyrandomizedcoronaryarterybypass graft-ingpopulation.
The clinical value of rSO2 was already demonstrated
in previous studies.8,16 Ito etal. investigatedthe
associa-tion between rSO2 and neurological outcomesin patients
without-of-hospitalcardiacarrest.Theauthorsenrolled92 patientsintheirstudyandfoundthattheoverallrateofgood neurologicaloutcomewas14%.Theyclassifiedtheirpatients into three categories and found that 0% of patients with rSO2≤25%,22.2%ofpatientswithanrSO2of 26---40%,and
50%ofpatientswithrSO2≥40%hadgoodneurological
out-comes.TheauthorsconcludedthatrSO2onhospitalarrival
may beapredictive factor for assessing neurological out-come.InanotherstudymadebyStormetal.,8theauthors
aimedtoinvestigatetheprognosticvalueofrSO2oncardiac
arrestpatients,andtheyfoundsignificantlyhigherrSO2
val-ues on survivorsthan non-survivors. They also found that the rSO2 ranges largely overlapbetween outcomegroups,
andconcludedthattherSO2valueshavelimitedpotentialto
predictpooroutcome.Theyconcludedthatnormalranges of rSO2 is based on a stable cerebral physiology, but the
effectsoftheimpairmentoftheblood---brainbarriercaused by global hypoxia due tocardiac arrestonrSO2 dynamics
remains unclear. Inour study,we found thatthe baseline rSO2 value was67.5 (46---70) and the difference between
baselineandrewarmingrSO2valuewas0.031(−0.08to0.20)
insurvivors.Innon-survivors,thebaselinerSO2valuewas30
(25---65)andthedifferencebetweenbaselineand rewarm-ingrSO2valuewas0.03(0.014---0.435).Althoughstatistically
considerable differencewas detected between groups on baselinerSO2values,nostatisticaldifferencewasdetected
onpercentchangesbetweenbaselineandrewarmingvalues ofrSO2(respectivelyp=0.003,0.526).
Inconclusion,therSO2 measurementissimple,andnot
affectedbyhypotensionorhypothermia;thus,therSO2may
be a useful predictorfor determining the prognosis after CPR.
Conflicts
of
interest
References
1.AtwoodC,EisenbergMS,HerlitzJ,ReaTD.IncidenceofEMS treatedout-of-hospitalcardiacarrestinEurope.Resuscitation. 2005;67:75---80.
2.NicholG,ThomasE,CallawayCW,etal.Regionalvariationin out-of-hospitalcardiacarrestincidence and outcome.JAMA. 2008;300:1423---31.
3.PeberdyMA,KayeW,OrnatoJP.Cardiopulmonaryresuscitation ofadultsin thehospital: a reportof 14,720cardiac arrests fromtheNationalRegistryofCardiopulmonaryresuscitation. Resuscitation.2003;58:297---308.
4.BouwesA,BinnekadeJM,VerbaanBW,etal.Predictivevalue of neurological examination for early cortical responses to somatosensoryevoked potentialsinpatientswithpostanoxic coma.JNeurol.2012;259:537---41.
5.MaiaB,RoqueR,Amaral-SilvaA,etal.Predictingoutcomeafter cardiopulmonaryarrestintherapeutic hypothermia patients: clinical,electrophysiologicalandimagingprognosticators.Acta MedPort.2013;26:93---7.
6.Sandroni C, Cavallaro F, Callaway CW, et al. Predictors of poorneurologicaloutcomeinadultcomatosesurvivorsof car-diac arrest: a systematic review and meta-analysis. Part 2: patientstreatedwiththerapeutichypothermia.Resuscitation. 2013;84:1324---38.
7.GreerDM,YangJ,ScripkoPD,etal.Clinicalexaminationfor prognosticationincomatosecardiacarrestpatients. Resuscita-tion.2013;84:1546---51.
8.StormC,LeithnerC,KrannichA,etal.Regionalcerebraloxygen saturationaftercardiacarrestin60patients---aprospective outcomestudy.Resuscitation.2014;85:1037---41.
9.Booth CM, Boone RH, Tomlinson G, et al. Is this patient dead,vegetative,orseverelyneurologicallyimpaired?Assessing outcome for comatose survivors of cardiac arrest. JAMA. 2004;291:870---9.
10.SchefoldJC,StormC,KrügerA,PlonerCJ,HasperD.The Glas-gowComaScoreisapredictorofgoodoutcomeincardiacarrest patientstreatedwiththerapeutichypothermia.Resuscitation. 2009;80:658---61.
11.SlaterJP,GuarinoT,StackJ,etal.Cerebraloxygendesaturation predictscognitivedeclineandlongerhospitalstayaftercardiac surgery.AnnThoracSurg.2009;87:36---44.
12.Yao FS,Tseng CC,Ho CY,Levin SK,Illner P.Cerebraloxygen desaturationisassociatedwithearlypostoperative neurophy-chologicaldysfunctioninpatientsundergoingcardiacsurgery.J CardiothoracVascAnesth.2004;18:552---8.
13.HigamiT,KozawaS,AsadaT,etal. Retrogradecerebral per-fusion versus selective cerebral perfusion as evaluated by cerebraloxygensaturationduringaortic archreconstruction. AnnThoracSurg.1999;67:1091---6.
14.Edmonds HL. Multi-modality neurophysiologic monitoring for cardiacsurgery.HeartSurgForum.2002;5:225---8.
15.MurkinJM,AdamsSJ,NovickRJ,etal.Monitoringbrain oxy-gensaturationduringcoronarybypasssurgery:arandomized, prospectivestudy.AnesthAnalg.2007;104:51---8.
16.ItoN,NantoS,NagaoK,HatanakaT,NishiyamaK,KaiT.Regional cerebral oxygen saturation on hospital arrival is a potential novelpredictorofneurologicaloutcomesathospitaldischarge inpatientswithout-of-hospitalcardiacarrest.Resuscitation. 2012;83:46---50.
17.TeasdaleG,JennettB.Assessmentandprognosisofcomaafter headinjury.ActaNeurochir(Wien).1976;34(1---4):45---55. 18.NolanJP,MorleyPT,HoekTL,HickeyRW.Therapeutic
hypother-mia after cardiac arrest. An advisory statement by the Advancement Life support Task Force of the International Liaison committee on Resuscitation. Resuscitation. 2003;57: 231---5.
19.Morrison LJ, DeakinCD,Morley PT, et al.2010 International Consensus on Cardiopulmonary Resuscitation and Emergency CardiovascularCareScienceWithTreatmentRecommendations. Circulation.2010;122:345---421.
20.MullieA, Verstringe P,BuylaertW, et al.Predictivevalueof Glasgowcomascore forawakening afterout-of-hospital car-diacarrest.CerebralResuscitationStudyGroupoftheBelgian SocietyforIntensiveCare.Lancet.1988;1:137---40.
21.WijdicksEF,HijdraA,YoungGB,BassettiCL,WiebeS.Practice parameter:predictionofoutcomeincomatosesurvivorsafter cardiopulmonary resuscitation (an evidence-based review): reportoftheQualityStandardsSubcommitteeoftheAmerican AcademyofNeurology.Neurology.2006;67:203---10.