Journal
of
Coloproctology
w w w . j c o l . o r g . b r
Original
Article
Clinical,
functional
and
morphologic
evaluation
of
patients
undergoing
lateral
sphincterotomy
for
chronic
anal
fissure
treatment.
Identification
of
factors
that
can
interfere
with
fecal
continence
Graziela
Olivia
da
Silva
Fernandes
a,∗,
Sthela
Maria
Murad-Regadas
b,
Francisco
Sérgio
Pinheiro
Regadas
b,
Lusmar
Veras
Rodrigues
b,
Iris
Daiana
Dealcanfreitas
c,
Jacyara
de
Jesus
Rosa
Pereira
d,
Erico
de
Carvalho
Holanda
e,
Francisco
Sérgio
Pinheiro
Regadas
Filho
faServiceofColoproctology,HospitalUniversitárioPresidenteDutra,UnifersidadeFederaldoMaranhão(UFMA),SãoLuís,MA,Brazil bDepartmentofSurgery,UniversidadeFederaldoCeará(UFC),Fortaleza,CE,Brazil
cServiceofColoproctology,HospitalRegionaldoCariri,JuazeirodoNorte,CE,Brazil
dServiceofColoproctology,HospitalUniversitário,UniversidadeFederaldoPiauí(UFPI),Teresina,PI,Brazil eServiceofColoproctology,SantaCasadeMisericórdiadeFortaleza,Fortaleza,CE,Brazil
fServiceofColoproctology,HospitalSãoCarlos,Fortaleza,CE,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received12March2014
Accepted19May2014
Availableonline2July2014
Keywords:
Chronicanalfissure
Lateralinternalsphincterotomy
Anorectalmanometry
Anorectalthree-dimensional
ultrasound
a
b
s
t
r
a
c
t
Objective:Evaluateclinical,functionalandmorphologicoutcomesoflateralsphincterotomy
forchronicanalfissuretreatment,andcorrelatethefindingswithfactorsthatinfluencein
theanalcontinence.
Method:Inaprospectivestudy,femalepatientstreatedbylateralsphincterotomyforchronic
analfissurewereassessedusingWexner’sincontinencescoreandgroupedaccordingto
score:groupI(score=0)andgroup2(score≥1)andevaluatedwithanalmanometryand
anorectal3Dultrasonography.
Results:Thirty-sixwomenswereincluded,33%hadvaginaldelivery.Seventeenpatients
wereincludedingroupIand19ingroupII.Wefoundnodifferenceinage,parityandmode
ofdeliverybetweengroups.Asignificantdifferencewithrespecttopercentagereductionin
restingpressureswasnoted,whencomparinggroup1versusgroup2.Theanalsphincter
musclelengthwassimilarinbothgroups.However,thelengthandpercentageoftransected
internalanalsphincterwassignificantlygreateringroupII.
Conclusion:Therewasacorrelationbetweenfecalincontinencesymptomsafter
sphinctero-tomywiththepercentageofrestingpressurereduction,lengthandpercentageoftransected
internalanalsphincter.
©2014SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All
rightsreserved.
∗ Correspondingauthor.
E-mail:[email protected](G.O.d.S.Fernandes).
http://dx.doi.org/10.1016/j.jcol.2014.05.006
Avaliac¸ão
clínica,
funcional
e
morfológica
de
pacientes
submetidas
à
esfincterotomia
para
tratamento
da
fissura
anal.
Identificac¸ão
dos
fatores
que
podem
interferir
na
continência
fecal
Palavras-chave:
Fissuraanalcrônica
Esfincterotomialateralinterna
Manometriaanorretal
Ultrassonografiaanorretal
tridimensional
r
e
s
u
m
o
Objetivo: Avaliarosresultadosclínicos,funcionaisemorfológicosdepacientessubmetidas
àesfincterotomiaparatratamentodefissuraanal,correlacionandoosresultadoscomos
fatoresquepodeminterferircomacontinênciafecal.
Método: Foram avaliadas prospectivamente pacientes do sexo feminino submetidas à
esfincterotomialateralinternadevidoàpresenc¸adefissuraanalcrônicautilizandooescore
deincontinênciadeWexneredistribuídasemdoisgrupos.Grupo1–Escoreigualazero
eGrupo2–maiorouiguala1.Aspacientesforamsubmetidasàavaliac¸ãofuncionale
anatômicadocanalanalutilizandomanometriaanorretaleultrassonografiatridimensional
anorretal.
Resultados: Das36 pacientesincluídas, 33%tinham históriade partovaginal.Dezessete
pacientesforamincluídas noGrupo1e 19no Grupo2.Nãohouvediferenc¸aquantoà
idade,paridadeetipodepartoentregrupos.Houvediferenc¸asignificanteemrelac¸ãoao
per-centualdereduc¸ãonapressãoderepousoquandocomparadoogrupo1comgrupo2.Não
houvediferenc¸anocomprimentodamusculaturaesfincterianaentregrupos.Noentanto,o
comprimentoeopercentualdeesfíncteranalinternoseccionadoforamsignificativamente
maioresnogrupo2.
Conclusão: Hácorrelac¸ãoentreossintomasdeincontinênciafecalpósesfincterotomiacom
opercentualdereduc¸ãodaspressõesderepouso,tamanhoepercentualdoesfíncteranal
internoseccionado.
©2014SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.
Todososdireitosreservados.
Introduction
Amongthosebenigndiseasesinvolvingtheanalcanal,anal
fissureisacommonoccurrenceinproctologicpractice,
cor-respondingto 10%ofvisits tocolorectal units.1 Theinitial
approachin thetreatment ofanal fissures isconservative,
aimingtoreducetheanal restingpressurebyloweringthe
sphinctertonus andimprovingtheblood supplyatthesite
ofthefissure,thuspromotinghealing.2Patientswithchronic
analfissureareadvisedtodrinkfluidsandfibersupplements,
aswellasusingstoolbulk-formingagents,emollientlaxatives,
analgesics,andtomakeuseoftopicalanestheticsandwarm
sitzbaths.3,4
Onfailureofmedicaltreatmentwithpersistenceof
symp-toms,surgicaltreatmentshouldbeoffered.3Openorclosed
lateral sphincterotomy is considered the gold standard for
the treatmentofchronic fissures.2,3 Thisprocedure results
indecreasedanalcanalpressures,leadingtoimproved
per-fusion,decreasedpainandulcer healing.5,6 However,when
inducinga sustained reduction in anal resting pressure, a
mild,butpermanent,incontinencemayresult.7–11According
toasystematicreviewofsurgicalstudiesconductedbyNelson,
theoverallriskofacontinencedisturbanceafterthesurgery
isapproximately10%,butcanreachupto35%.12
New imaging methods have enabled the realization of
detailedanatomicstudiesoftheanalcanalandofthe
arrange-mentofsphinctermuscles,resultinginanincreasedinterest
inusingthesemethodstoobtain acomplete evaluationof
patientswithdysfunctions,aiminganadequatetherapeutic
choice.13,14Thisstudyaimstoevaluatetheclinical,functional
andmorphologicaloutcomesofpatientsundergoing
sphinc-terotomyfortreatmentofanalfissure,correlatingtheresults
withthosefactorsthatcaninterferewithfecalcontinence.
Method
FromFebruary2011toMay2013,weevaluatedfemalepatients
withameanage of42.35(21–55)years oldwhounderwent
sphincterotomy due tochronic anal fissure and withanal
sphincterhypertoniaprovenwithanorectalmanometryfrom
theDepartmentofColoproctology,HospitalUniversitário
Wal-terCantídio,UniversidadeFederaldoCeará(HUWC-UFC).The
studywasapprovedbytheEthicsCommitteeinResearchof
theHospital.
Thepatientsunderwentacompleteclinicalandproctologic
evaluation and underwent anorectal manometry. Initially,
theywereclinicallytreated,includingwithhygieneanddiet
guidelines,stoolbulk-formingagentsandtopicnitratesfor12
weeks.Thosewhoremainedsymptomaticwerereferredfor
surgical treatment.Afterpreoperativetests anda standard
flexiblesigmoidoscopy,anopen lateralinternal
sphinctero-tomywasperformedbyagroupof3surgeonswithexpertisein
colorectalsurgery,withapreviouslystandardizedtechnique,
withtransectionoftheinternalanalsphincterextendingup
totheapexofthefissure.
Thepatientswere weeklyfollowedatthecoloproctology
outpatientclinic,HUWC-UFC,untilcompletehealingofthe
woundandabsenceofsymptoms.Fourmonthsafterwound
healing,thepatientswereevaluatedforanalcontinenceby
usingtheWexnerincontinencescore,15beingdividedintotwo
groups:groupI–patientswithincontinencescoreequalto
zero,andgroupII–patientswithscoregreaterthanorequal
to1.Then,theyweresubjectedtofunctionaland
anatomi-calevaluationoftheanalcanalusinganorectalmanometry
andanorectaltridimensionalultrasonography(3DUS),
respec-tively.
Nineteenhealthy female volunteers without proctologic
orcolorectal diseases,withoutpreviousproctologic surgery
and without prior pelvic surgery, from the coloproctology
outpatientclinic,HUWC,were alsoincludedforanatomical
evaluationoftheanalcanal.
Patientsolderthan55years,obese,diabetic,sufferingfrom
acquired immunodeficiency syndrome, with complaints of
urinaryorfecalincontinence,womenwithassociatedbenign
andmalignantanorectaldiseasesorwithpreviouscolorectal
orproctologicsurgerywereexcludedfromthestudy.Women
without prior electromanometry, without evidence of anal
hypertonia,andthosewithprioranalsphincterinjuryproven
byimagingstudieswerealsoexcluded.
Anorectalmanometry
Theequipmentusedtoperformanorectalelectromanometry
was Medtronic® hydropneumatic electromanometer,
com-posedofaneight-channelradialcatheter.Theexamination
wasperformedbyastaggeredmanualremovaltechniqueat
intervalsofonecentimeter,starting6.0cmcranialtotheanal
border(AB)bythesameexaminer.Theparametersevaluated
inthisstudyincludedmeanrestingpressure(Prest)and
maxi-malvoluntarypressure(MVP).
Anorectalthree-dimensionalultrasonography(3DUS)
Allparticipantsunderwent rectalenema2hoursbeforethe
examination.APro-Focusultrasoundequipmentwith
trans-ducer with 360◦, type 2052, with a frequency of 9–16MHz
and focal length ranging from 2.8 to 6.2cm (B-K Medical,
Herley,Denmark)wasused.Thistransducerperformsimage
acquisitionautomaticallyintheproximal-distaldirectionina
segmentof6.0cmfor50s.
A sequence of numerous parallel transaxial images is
acquired,resultinginavolumetricimagescannedintoacube,
enabling ananalysisonmultipleplanes. Inall tests,a
fre-quencyof16MHzandfocaldistanceof3.0cmwasused.16,17
Ascanwasperformedwiththeaimtoassessthecomplete
anatomyoftheanalcanal.Allexaminationswereperformed
byasingleinvestigatorandevaluatedbytwocoloproctologists
experiencedinthismethod.
Theacquiredimageswereanalyzedinmultipleplanes.
Theevaluatedparametersincludedmeasurements(cm)of
sphinctermuscleperformedonsagittaland coronalplanes
(Fig.1):lengthoftheexternalanalsphincter(EAS),lengthof
gap(correspondingtotheareaoftheanteriorquadrant
with-out striated muscle –between the proximalborder of EAS
and theproximalborder ofthe puborectalis(PR), lengthof
externalanalsphincter-puborectalis(posterior)complex
(EAS-PR),lengthofintactcontralateralinternalanalsphincter(IAS),
lengthofremainingIAS,lengthofIASandpercentageof
tran-sectedIASduringtheoperativeprocedure.
Incontinence scores were correlated with age, parity,
resting and maximal voluntary pressures quantified with
anorectalmanometry,andultrasound anatomical
measure-mentsofsphinctermuscle.
Theanatomicalmeasurementsoftheanalcanalobtained
by anorectal ultrasonography were compared between
patientswhounderwentsphincterotomyandfemale
volun-teers.
The intraclass correlation coefficient was evaluated to
compareultrasoundmeasurementsbetweentwoexaminers
experiencedin3DUltrasoundbothforpatientswho
under-wentsphincterotomyandforvoluntarywomen.
StatisticalanalyzeswereperformedusingGraphPadPrism
5.0and SPSSversion 17 forWindows® programs.Thedata
evaluation included descriptive statistical methods (mean,
standard deviation, median,interquartile range). Regarding
theanalyticalmethods,weappliedtheStudent’st-test,
one-way ANOVA and Fisher’s chi-squared test. p<0.05 was the
valueusedforstatisticalsignificance.
ICC (intraclass correlation coefficient) was also used
to compare ultrasonographic anatomical measurements
between examiners with a confidence interval of 95%,
and reliability was classified according to the Altmann
classification system (<0.20=poor; 0.1–0.40=reasonable;
0.41–0.60=moderate; 0.61–0.80=good; 0.81–1.00=very
good).18
Results
Thirty-six patients who underwent sphincterotomy forthe
treatmentofchronicanalfissurewereincludedinthisstudy.
Nopostoperativecomplicationswereobserved,andhealing
of wounds between 2 and 3 months postoperatively was
observed.Thefollow-uptimerangedfrom6to8monthsafter
thesurgicalprocedure.Thecontrolgroupincluded19
asymp-tomaticvolunteers.
Themeanageofpatientsundergoingsphincterotomywas
42.35(21–55)years.Themeanageofpatientsinthecontrol
groupwas38.68(21–50)years.
Regarding parity,amongthose patientswho underwent
sphincterotomy 14 (39%)were nulliparous, 12 (33%) hadat
leastonevaginaldeliverywithameanof2(1–3)births,and
10 (28%)underwentcesarean deliverywithoutlabor. Inthe
controlgroup,7(37%)patientswerenulliparous,7(37%)had
atleastonevaginaldeliverywithanaverageof2(1–3)
deliv-eries,and5(26%)underwentcesareansectionwithoutlabor.
Thedistributionofparityand typeofdeliverywere similar
betweengroups(p=0.8901).
The incontinence score ranged from 0 to 7. Seventeen
patientshadanincontinencescoreofzero(groupI)and19
patientshad greaterthan orequalto1scores(groupII).In
relation to group II scores, the median was 4(3–7). When
groupsIandIIwerecomparedregardingage,parityandmode
ofdelivery,nostatisticaldifference(p=0.6361andp=0.9039,
respectively)wasobserved.
Anal restingpressures in both groups decreased
signif-icantly when preoperative and postoperative figures were
compared(p<0.0001).Therewasnosignificantdifferencein
Right
Anterior
A
B
Distal Proximal
5-EAS-PR 1-EAS
4-IAS 2-IAS
3-GAP
Posterior
1-IAS Contralateral
Proximal Left
2-IAS Remaining
3-Sectioned IAS
Distal
Fig.1–(A)Analcanaloffemalepatient(sagittalplane).Sonographicparameters:1,lengthofpreviousEAS;2,lengthof previousIAS;3,lengthofthegap;4,lengthofposteriorIAS;5,lengthofEAS-PRcomplex.(B)Analcanaloffemalepatient (coronalplane)–sonographicparameters:1,lengthofcontralateralIAS;2,lengthofremainingIAS;3,lengthoftransected IAS(dashedline).
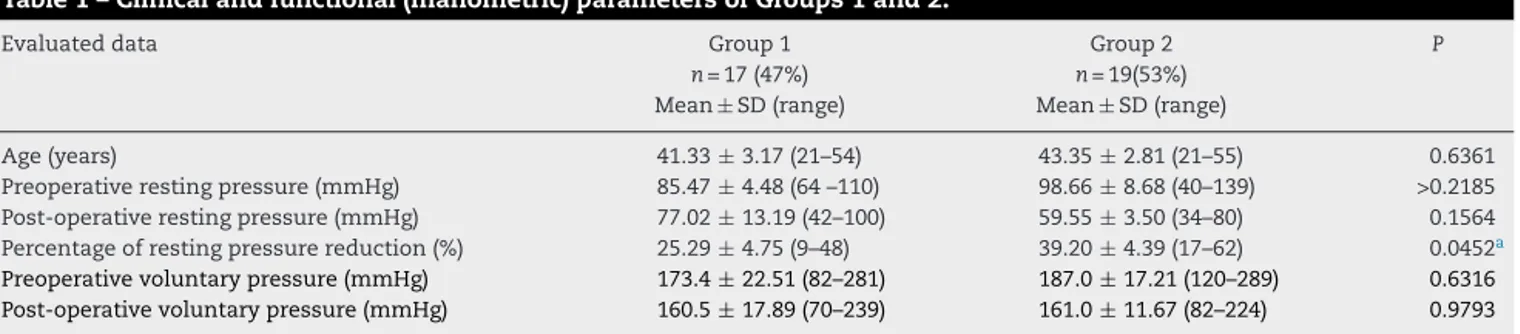
pressuresingroupIversusgroupII.However,asignificant
dif-ferencewasobservedwithrespecttopercentagedecreasein
restingpressure,whencomparingpre-versuspostoperative
valuesingroupIversusgroupII(p=0.0452)(Table1).
Therewasnosignificantdifferencebetweenpreoperative
andpostoperativemaximalvoluntarypressures(p=0.4014)in
bothgroups. Likewise,therewerenosignificantdifferences
in preoperative versus postoperative voluntary pressures
(p=0.6316)whencomparedgroup1versusgroup2(p=0.9793)
(Table1).
Theultrasoundevaluationshowedinternalanalsphincter
lesion inall 35 patients included inthe study who
under-wentlateralinternalsphincterotomy.Therewasnoevidence
ofanteriorexternalanalsphincterandposteriorpuborectalis
injury,eveninpatientsundergoingvaginaldelivery.
Themeasuresofsphinctermuscleusing3DUSarelistedin
Tables2and3.
Nosignificantdifferenceinthelengthofanteriorexternal
analsphincter,externalanalsphincter-puborectal(posterior)
complexandinthegap,whencomparinggroupIversusgroup
II.However,thelengthandpercentageoftransectedIASwere
significantlyhigheringroupIIcomparedtogroupI.No
statis-ticallysignificantdifferenceinthelengthofcontralateralIAS
wasobserved(Table2).
No significant difference in the length of the anterior
external anal sphincter, externalanal sphincter-puborectal
Table1–Clinicalandfunctional(manometric)parametersofGroups1and2.
Evaluateddata Group1 Group2 P
n=17(47%) n=19(53%)
Mean ± SD(range) Mean± SD(range)
Age(years) 41.33± 3.17(21–54) 43.35± 2.81(21–55) 0.6361
Preoperativerestingpressure(mmHg) 85.47± 4.48(64–110) 98.66± 8.68(40–139) >0.2185 Post-operativerestingpressure(mmHg) 77.02± 13.19(42–100) 59.55± 3.50(34–80) 0.1564 Percentageofrestingpressurereduction(%) 25.29± 4.75(9–48) 39.20± 4.39(17–62) 0.0452a
Preoperativevoluntarypressure(mmHg) 173.4±22.51(82–281) 187.0±17.21(120–289) 0.6316
Post-operativevoluntarypressure(mmHg) 160.5±17.89(70–239) 161.0±11.67(82–224) 0.9793
Table2–Measuresofsphinctermusclesusing3DanorectalultrasonographyinGroups1and2.
Evaluatedparameters Group1 Group2 P
n=17(47%) n=19(53%)
Mean± SD(range) Mean ± SD(range)
SectionedIAS(cm) 0.59± 0.04(0.4–1) 0.87± 0.06(0.4–1.3) 0.0024a
PercentageoftransectedIAS(cm) 18.71±1.57(9–30) 25.65±2.14(10–37) 0.0138a
ContralateralIASlength(cm) 3.14±0.10(2.7–4.3) 3.39±0.08(3.0–4.0) 0.0721
AnteriorEAS(cm) 1.89±0.04(1.6–2.3) 1.90±0.07(1.6–2.6) 0.9464
EAS-PR(cm) 3.38±0.11(2.9–4.3) 3.66±0.09(3.0–4.5) 0.0840
Gap(cm) 2.01±0.13(1.1–3.2) 1.90±0.07(1.6–2.6) 0.4795
a p<0.05.
Table3–Comparisonbetweenlengthsoftheanalsphincters(EAS–externalanalsphincter,EAS-PR–externalanal sphincter-puborectalcomplex)andofthegapbetweenpatientswhounderwentsphincterotomyandvoluntary participants.
Controlgroup Sphincterectomygroup P
n=24 n=36
Mean(standarddeviation) Mean(standarddeviation)
EAS,anterior(cm) 1.83± 0.234(1.6–2.5) 1.89± 0.263(1.6–2.6) 0.3456
EAS-PR(cm) 3.47± 0.449(2.6–4.4) 3.49± 0.360(2.9–4.5) 0.3870
Gap(cm) 2.00± 0.535(0.9–3.2) 1.98± 0.504(1.1–3.2) 0.4786
(posterior)complexandinthegap,whenpatientsundergoing sphincterotomywerecomparedwithvolunteers(Table3).
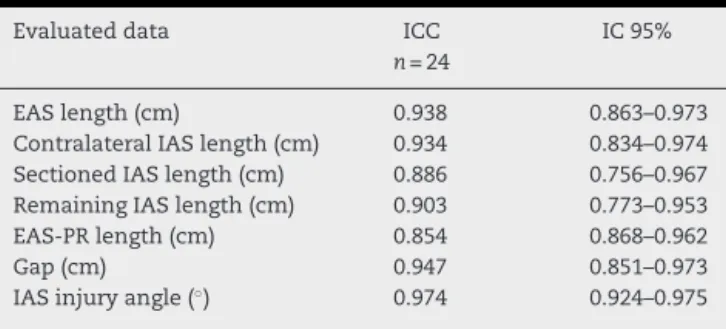
The intraclass correlation coefficient for measures by
anorectal three-dimensional ultrasonography evaluated 30
patients:20patientswhounderwentsphincterotomyand10
volunteerspresentingaverygoodresult,rangingfrom0.756
to0.975(Table4).
Discussion
Thisstudy evaluated the clinical, morphologicaland
func-tional results after sphincterotomy for treatment of anal
fissureexhibitinghighlevelsoffecalincontinence(inabout
halfofpatients)comparedwiththeliterature.Thetrue
inci-denceoffecalincontinenceisunderestimatedandonlyfew
doctorsactivelyquestionthissubject,especiallyinpatients
who do not provide this informationvoluntarily.19 In this
study,changesinfecalcontinencewereevaluatedafter
com-pletewoundhealing,usingtheWexnerincontinencescore.15
Itispossiblethatthehighfrequencyobservedisduetothefact
ofconsideringasincontinentthosepatientswithascoreequal
toorgreaterthan1,bytheinclusionofonlywomen(whohave
Table4–Distributionaccordingtotheintra-class correlationcoefficientforultrasoundmeasures.
Evaluateddata ICC IC95%
n=24
EASlength(cm) 0.938 0.863–0.973
ContralateralIASlength(cm) 0.934 0.834–0.974 SectionedIASlength(cm) 0.886 0.756–0.967 RemainingIASlength(cm) 0.903 0.773–0.953
EAS-PRlength(cm) 0.854 0.868–0.962
Gap(cm) 0.947 0.851–0.973
IASinjuryangle(◦) 0.974 0.924–0.975
ashorteranalcanal)andalsobythewayofquestioningabout incontinence,whichwasperformedactively:eachpatientwas individuallyassessedbyacoloproctologistnotparticipatingin hercolorectalsurgicalprocedure,sothatthewomancouldfeel morecomfortableinheranswer.Casillasetal.demonstrated
thatpatientsmayfeelembarrassedanddenysomesymptoms
inthepresenceoftheirsurgeons,andthattheytendtoignore subtleproblemsaftersurgery,suchasgasincontinence.20
Althoughcontroversial,severalfactorsseemtoaffectthe
final postoperative result. Amongthese, the surgical
tech-nique (open or closed),21 type of anesthesia (general or
local),22 lengthofthesphincterotomy,23,24 additional
proce-duresperformed,25presenceofpreviousanorectalsurgeryand
obstetrichistoryareincluded.26,27 Inthisstudy,the
sphinc-terotomywasofopen-typeandaccordingtothelengthofthe
analfissure,showingexcellentresultswithrespecttowound
healing.Theratesofpostoperativeincontinencearesimilar
whenopenversusclosedtechniquewerecompared.8,11
Sul-tanetal.suggestintheirstudythatthesphincterotomyends
upimplyingproportionallygreaterextensionofIASthanthe
surgeon’s initialintentionofperforming.23 Inourstudy,we
observed that in patients with symptomsof fecal
inconti-nence,thesizeandpercentageofthetransectedinternalanal
sphincterweresignificantlyhigher,around25%,andthiswas
theonlyfactorthatinterferedwithfecalincontinence.Ithas
beenshownalsothatthemeasurementsoftheanal
sphinc-ters(EAS,EAS-PRandcontralateralIAS)andofthegapwere
similarinpatientswithandwithoutsymptomsoffecal
incon-tinence,excludinganymorphologicalchangeadditionaltoIAS
injurythatcouldinterferewiththeresultsofthisproblem.
When comparing age, parity and type of delivery
between continent and incontinent groups, no difference
wasobserved.Asymptomaticanalsphincterdefectsare
com-mon inwomenaftervaginalchildbirth.23 Inthis study,we
chosetoexcludepatientsalreadywithpreoperatively
postoperatoryultrasonography,inordertotrytoevaluatethe
resultsoftheisolatedtransectionoftheinternalanal
sphinc-terasafactorthatinterfereswiththelossoffecalcontinence.
Acareful patient selection, the absence of preoperative
problemsofcontinenceandameticulouslyperformed
surgi-caltechniquebysurgeonsskilledinproctologicsurgeryare
necessarytoachievegoodresults.28
Theendoanalultrasoundandanorectalmanometryhave
beenfrequentlyusedtoevaluatepatientswithfecal
incon-tinence. Tjandra et al. compared patients who underwent
sphincterotomy and that have become incontinent versus
thosesubjectedtothesameprocedure,butwithoutsymptoms
ofanorectalincontinence,usinganorectalultrasound
evalu-ation.ThosepatientswithWexnerincontinencescoreabove
4wereconsideredasincontinent.15,26,27Themedianscoreof
incontinencewas9(6–13)andallwomenhadundergone
pre-viousvaginalbirthandhad ahistoryofpreviousanorectal
surgery.26,27 Inthepresent study,thescoreofincontinence
rangedfrom 0to7,withamedianof4forthe incontinent
group,andthoseparticipantswithascore≥1wereconsidered
asincontinent.Thesedifferencesinmethodologyand
assess-mentmayexplainthedifferencesinresultsinthecomparison
amongstudies.
The sphincterotomy permanently decreases the resting
pressurethatiselevatedinmostpatientswithanalfissures,
with anorectal manometry being able to demonstrate this
reduction,whentheprocedureisperformedinthepre-and
postoperativeperiodinpatientsundergoingthisoperation.29
Inourpatients,themanometricfindingsalsodemonstrated
thatlateralsphincterotomysignificantlyreducedanalresting
pressuresinpatientswithchronicanalfissureinthegroup
withandwithoutsymptomsoffecalincontinence.However,
thepercentageofreductioninrestingpressureswas
signif-icantlyhigherintheincontinentgroup.Ontheotherhand,
Garcia-Aguilaretal.foundnostatisticallysignificant
differ-encebetweenrestinganal pressuresinpatientsundergoing
sphincterotomyand who became incontinentversus those
whoremainedcontinent.24Studiesshowthatthemanometric
findingsandfecalincontinencesymptomsmaynotpresent
acorrelation,becausemanyfactorscaninterferewithfecal
continenceandpresentdivergentresults.24,26
Imaging procedures in anatomical studies of the anal
canal are being increasingly used, broadening our
knowl-edge and providing details often not visible in classical
anatomicaldissections.Anorectalultrasound,specificallythe
three-dimensionalmodewithautomaticacquisition,enables
a complete morphological evaluation of the anal canal in
multipleplanes,beingpossibletoperformaccurate
measure-mentsofthelongitudinallengthofthesphinctermuscle.16,17
Regadasetal.demonstrated,bycomparingthelongitudinal
lengthofsphinctermuscleintheanterioranalcanalbetween
genders,thatEASandIASaresmallerinwomen;andthatthe
areadeprivedofEAS,theso-calledgap,locatedintheproximal
andsuperiormiddleanalcanal,islargerinwomen.16,17Thus,
thislessresistantandsignificantlylargerareacouldexplain
thehighprevalenceofdisordersofcontinenceandevacuation
infemales.
The preoperative endoanal ultrasound can identify an
inadvertenttransectionofEASoraninadequatetransection
ofIASasreasonsforthefailureoffissurehealing.30Thus,this
proceduremaybeindicatedinpatientswithhighriskofanal
incontinence,andinmultiparouswomenandinthosewith
suspectedorknownsphincterinjury.21
In the present study, we used the three-dimensional
mode withautomaticacquisition,enabling theassessment
of the length of the sphincter muscle and the
percent-ageoftransectedmuscle,comparingthetransectedinternal
anal sphincterwith its contralateral counterpart,to
corre-late withthe presenceof symptomsoffecal incontinence.
Exactmeasurementofthe lengthofthe sphinctermuscles
wasperformedinallpatientsundergoingsphincterotomyand
comparedtothosehealthyvolunteerswithoutpriorsurgery,to
assesstheanatomicalstructuresrelatedtocontinenceandnot
onlytheinternalanalsphinctertransectedduringthe
sphinc-terotomy.Ourmeasurementsofmusclelengtharecomparable
tothosemadebyRegadasetal.,consideringthattheseauthors
usedsimilar devicesand anatomicalreferences.17 All
mea-surementstakenbyultrasoundwerecomparedbetweentwo
observerswithexperienceinperformingtheprocedure;avery
goodintraclasscorrelationcoefficientwasobserved,similarly
toother studiesintheliterature,sincesimplemeasuresof
lengthofsphinctermuscleswereperformed, withuseofa
transducerwithautomaticacquisition,excludingthe
inter-ferenceofmovementoftheprobe.13,14
Thisstudy waslimitedbythesmall numberofpatients
andtheexclusivereviewoffemalepatients.Furtherstudies
evaluatingtheresultsinmalesareneededtoverifytheeffect
ofsphincterotomyinbothgenders.
Thepostoperative anal incontinenceis awell-described
complaint among patients who underwent lateral internal
sphincterotomy for anal fissure.21 Thus, all these clinical,
manometricandultrasounddataaddimportantnew
informa-tionandperspectivesonthepre-andpostoperativeevaluation
of patients with anal fissure. This joint evaluation could
providedatatoplanquantitativelythemusclesectionduring
sphincterotomy,avoidingchangesinfecalcontinence,since
patientsmayaddcumulativedamagethroughouttheirlives,
especiallyfemales,forinstance,byvaginalchildbirth,other
proctologicsurgeriesandmenopause.
Conclusion
Femalepatientsundergoinglateralinternalsphincterotomy
presentsignificantreductioninrestingpressureoftheanal
canalassociatedwithinjurytothe internalanalsphincter.
There is acorrelation between symptoms offecal
inconti-nenceaftersphincterotomywiththepercentageofreduction
inrestingpressuresandsizeandpercentageofthetransected
internalanalsphincter.Nootherfactorsaffectingtheresults
wereidentified.
Funding
CNPQ.
Conflicts
of
interest
r
e
f
e
r
e
n
c
e
s
1. GarnerJP,McfallM,EdwardsDP.Themedicalandsurgical managementofchronicanalfissure.JRArmyMedCorps. 2002;148:230–5.
2. PohA,TanKY,Seow-ChoenF.Innovationsinchronicanal fissuretreatment:asystematicreview.WorldJGastrointest Surg.2010;2:231–41.
3. AltomareDF,BindaGA,CanutiS,LandolfiV,TrompettoM, VillaniRD.Themanagementofpatientswithprimarychronic analfissure:apositionpaper.TechColoproctol.
2011;15:135–41.
4. SharpFR.Patientselectionandtreatmentmodalitiesfor chronicanalfissure.AmJSurg.1996;171:512–5.
5. AbcarianH.Surgicalcorrectionofchronicanalfissure:results oflateralinternalsphincterotomyvsfissurectomy-midline sphincterotomy.DisColonRectum.1980;23:31–6.
6. HawleyPR.Thetreatmentofchronicfissure-in-ano:atrialof methods.BrJSurg.1969;56:915–8.
7. ChowcatNL,AraujoJG,BoulosPB.Internalsphincterotomy forchronicanalfissure:longtermeffectsonanalpressure.Br JSurg.1986;73:915–6.
8. ArroyoA,PerezF,SerranoP,CandelaF,CalpenaR.Open versusclosedlateralsphincterotomyperformedasan outpatientprocedureunderlocalanesthesiaforchronicanal fissure:prospectiverandomizedstudyofclinicaland manometriclongtermresults.JAmCollSurg.2004;199:361–7.
9. AysanE,ArenA,AyarE.Aprospective,randomized, controlledtrialofprimarywoundclosureafterlateral internalsphincterotomy.AmJSurg.2004;187:291–4.
10.KaramanlisE,MichalopoulosA,PapadopoulosV,MekrasA, PanagiotouD,IoannidisA,etal.Prospectiveclinicaltrial comparingsphincterotomy,nitroglycerinointmentand xylocaine/lactulosecombinationforthetreatmentofanal fissure.TechColoproctol.2010;14:S21–3.
11.WileyM,DayP,RiegerN,StephensJ,MooreJ.Openvs.closed lateralinternalsphincterotomyforidiopathicfissure-in-ano: aprospective,randomized,controlledtrial.DisColon Rectum.2004;47:847–52.
12.NelsonRL.Operativeproceduresforfissureinano.Cochrane DatabaseSystRev.2005:CD002199.
13.Murad-RegadasSM,RegadasFS,RodriguesLV,KenmotiVT, FernandesGO,BuchenG,etal.Effectofvaginaldeliveryand ageingontheanatomyofthefemaleanalcanalassessedby three-dimensionalanorectalultrasound.ColorectalDis. 2012;14:1521–7.
14.KnowlesAM,KnowlesCH,ScottSM,LunnissPJ.Effectsofage andgenderonthree-dimensionalendoanalultrasonography measurements:developmentofnormalranges.Tech Coloproctol.2008;12:3–9.
15.JorgeJMN,WexnerSD.Etiologyandmanagementoffecal incontinence.DisColonRectum.1993;36:77–97.
16.RegadasSMM,RegadasFSP,RodriguesLV,SilvaFR,LimaDMR, Regadas-FilhoFSP.ImportânciadoUltra-somTridimensional naAvaliac¸ãoAnorretal.ArqGastroenterol.2005;42:226–32.
17.RegadasFS,Murad-RegadasSM,LimaDMR,SilvaFR,Barreto RGL,SouzaMHLP,Regadas-FilhoFSP.Analcanalanatomy showedbythree-dimensionalanorectalultrasonography. SurgEndosc.2007;21:2207–11.
18.AltmannDG.Practicalstatisticsformedicalresearch.London: Chapman&Hall;1991.
19.JohansonJF,LaffertyJ.Epidemiologyoffecalincontinence: thesilentaffliction.AmJGastroenterol.1996;91:33–6.
20.CasillasS,HullTL,ZutshiM,TrzcinskiR,BastJ,XuM. Incontinenceafteralateralinternalsphincterotomy:arewe underestimatingit?DisColonRectum.2005;48:1193–9.
21.Garcia-AguilarJ,BelmonteC,WongD,LowryAC,AdoffRD. Openvs.closedsphincterotomyforchronicanalfissure.Dis ColonRectum.1996;39:440–3.
22.KeighleyMR,GrecaF,NevahE,HaresM,Alexander-WilliamsJ. Treatmentofanalfissurebylateralsubcutaneous
sphincterotomyshouldbeundergeneralanesthesia.BrJ Surg.1981;68:400–1.
23.SultanAH,KammMA,NichollsRJ,BartramCI.Prospective studyoftheextentofinternalanalsphincterdivisionduring lateralsphincterotomy.DisColonRectum.1994;37:1031–3.
24.Garcia-AguilarJ,BelmonteC,PerezJJ,JensenL,MadoffRD, WongWD.Incontinenceafterlateralinternal
sphincterotomy:anatomicandfunctionalevaluation.Dis ColonRectum.1998;41:423–7.
25.LeongAFPK,HusainMJ,Seow-choenF,GohHS.Performing internalsphincterotomywithotheranorectalprocedures.Dis ColonRectum.1994;37:1130–2.
26.TjandraJJ,HanWR,OoiBS,NageshA,ThorneM.Fecal incontinenceafterlateralinternalsphincterotomyisoften associatedwithcoexistingoccultsphincterdefects:astudy usingendoanalultrasonography.AustNZJSurg.
2001;71:598–602.
27.TjandraJJ,MilsomJW,SchroederT,FazioVW.Endoluminal ultrasoundispreferabletoelectromyographyinmapping analsphincterdefects.DisColonRectum.1993;36:689–92.
28.ElsebaeMM.Astudyoffecalincontinenceinpatientswith chronicanalfissure:prospective,randomized,controlledtrial oftheextentofinternalanalsphincterdivisionduringlateral sphincterotomy.WorldJSurg.2007;31:2052–7.
29.McnamaraMJ,PercyJP,FieldingIR.Amanometricstudyof analfissuretreatedbysubcutaneouslateralinternal sphincterotomy.AnnSurg.1990;211:235–8.