w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
The
importance
of
three-dimensional
anorectal
ultrasound
in
the
study
of
patients
with
anal
pain
Doryane
Maria
dos
Reis
Lima
a,b,∗,
Univaldo
Etsuo
Sagae
a,b,
Gustavo
Kurachi
a,b,
Salua
Hamaoui
a,b,
Tomaz
Massayuki
Tanaka
a,b,
Mauro
Willemann
Bonatto
a,b,
Ricardo
Shigueo
Tsuchiya
a,b,
Carlos
Alberto
de
Carvalho
a,baMedicalCourse,FaculdadeAssisGurgacz(FAG),Cascavel,PR,Brazil
bGastroclínicaCascavelLtda.,Cascavel,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received14May2014 Accepted12September2014 Availableonline29January2015
Keywords: Analpain
Anorectalultrasound Intersphinctericsepsis
a
b
s
t
r
a
c
t
Objectives: Analpaincanbecausedbyvariousmedicalconditions;theexclusionoforganic causesforpropertreatmentisimportant.Three-dimensionalanorectalultrasoundcan iden-tifyorganiccausesofanalpain.Theobjectiveofthisstudywastoevaluatetheimportanceof three-dimensionalanorectalultrasoundinthedetectionoforganicabnormalitiesinpatients withanalpain.
Methods:Twenty-twopatients(meanage:49years;13women)withchronicanalpainwere enrolledtojoinaprospectivestudybetweenJune2009andJune2011.Acompleteproctology andcolonoscopyexaminationwasnormal.Subsequently,thepatientsunderwent three-dimensionalanorectalultrasound.
Results:Intersphinctericsepsiswasfoundin14patients(63.6%).Twofemalepatients(9.1%) hadanalsphincterinjury,oneofthemwiththepresenceofagradeII rectocele.There wasanincreaseinthethicknessofthesubepithelialtissueinthreepatients(13.6%).Inone patient(4.6%),thepresenceofahypoechoiccircularretrorectal(presacral)cystofthemiddle andlowerrectumwasobserved.Thethree-dimensionalanorectalultrasoundexamination showednoabnormalitiesintwopatients(9.1%).
Conclusion: Thethree-dimensionalanorectalultrasoundisasimple,economical,fastand usefultestforthestudyofanorectaldiseasesandshouldbeincludedintheexaminationof patientswithanalpain,toexcludeorganiccauses.
©2015SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All rightsreserved.
∗ Correspondingauthor.
E-mail:[email protected](D.M.d.R.Lima).
http://dx.doi.org/10.1016/j.jcol.2014.09.002
Palavras-chave: Doranal
Ultrasomendorretal Sepseinteresfincteriana
r
e
s
u
m
o
Objetivos: Adoranalpoderesultarváriascondic¸õesclínicasesefaznecessárioexcluir causasorgânicasparaotratamentoadequado.Aultra-sonografiaanorretaltridimensional (3D-US)podeidentificarcausasorgânicasdedoranal.Oobjetivodesteestudofoiavaliara importânciada3D-USparadetectaranomaliasorgânicasempacientescomdoranal. Métodos: Vinteedoispacientes(médiadeidade:49anos;trezemulheres)comdoranal crônicaforamincluídosemumestudoprospectivoentrejunhode2009ejunhode2011.O exameproctológicocompletoecolonoscopiaforamnormais.Posteriormente,ospacientes foramsubmetidosà3D-US.
Resultados: Sepseinteresfincterianafoievidenciadaemquatorzepacientes(63,6%).Duas pacientes(9.1%)apresentaramlesãodoesfíncteranal,sendoumacompresenc¸ade reto-celegrauII.Oaumentodaespessuradotecidosubepitelialapresentou-seemtrêspacientes (13,6%).Emumpaciente(4,6%),foievidenciadaapresenc¸adecistoretrorretalcircular hipoe-coiconoretomédioeinferior.OexamedeUS-3Dnãoevidenciouanormalidadesemdois indivíduos(9.1%).
Conclusão: Aultra-sonografiaanorretaltridimensionaléumexamesimples,econômico, rápidoeútilnoestudodedoenc¸asanorretaisedeveserincluídonoestudodospacientes comdoranalparadescartarcausasorgânicas.
©2015SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda. Todososdireitosreservados.
Introduction
Chronicanalpaincanbecharacterizedasanoftenintense, poorlydefined,not-irradiatingand,insomecases,lancinating painwithatleastthreemonthsduration.Theprevalenceof anorectalpaininAmericanhouseholdheadswas6.6%,being morecommoninwomen1andaccountsfor30–40%ofvisits
foranalpain.2
Thisconditioncanresultfromavarietyofcausesandmay beassociatedwithproctologic,gynecological,genitourinary, traumatic,neurological or psychologicalchanges.3 In most
patients,athoroughclinicalhistorycharacterizingthenature ofanalpainanddefiningwhetherthereisornota relation-shipwithstraining,inassociationwithathoroughphysical exam,allowsthephysiciantoestablishthediagnosis.Thus, theexclusionoforganiccausesofanorectalpainnot identi-fiedafterathoroughproctologicexaminationisneeded.As anexample,wecanmention:deepperirectal postoperative sepsis,4primaryintersphinctericabscess,5hiddensphincter
injuries, and other organic diseases ofsurgical resolution. Therearealsocasesofanorectalpainoffunctionaletiology suchasproctalgiafugax,elevatorsyndromeandunspecified chronicanorectalpain. Anaccuratediagnosisisneededfor propertreatment.
Anorectalultrasonographyisanimagingdiagnostic tech-niqueindicatedinbenignandmalignantanorectaldisorders.6
Thistechniqueconstitutesanimportantallyinthedetection oforganic causesofanal painwithnochangesinphysical examination.Morerecently,duetothelimitationforviewing imagesinthelongitudinalplane,atransducerthatallowsthe three-dimensionalreconstructionofimageswhichare two-dimensionallyobtainedwasintroduced.7
Withthistypeofultrasound,thephysicalexaminationhas beenenrichedwithaccurateinformationonanalcanaland rectumonseveralplanes,andthistechniquecandemonstrate thesizeandpositionofallanatomicalstructures.
Objective
The aim of this paper is to emphasize the importanceof three-dimensionalanorectalultrasonographyinpatientswith chronicanalpainwithoutchangeintheirphysical examina-tion.
Methodology
Thisisaprospectivestudyconductedduringtheperiodfrom June 2009 to June 2011 in 22 patients with chronic anal pain suspected ofhavingafunctional diagnosis. The aver-ageagewas49years,with13women(59.1%)andninemen (40.9%).
Thisstudycomprisedpatientswithchronicanalpain last-ing more than threemonths.1 Thepain wascharacterized
byhavingdurationfrom15sto20minandwithnorelation tostraining.Inaddition,ourpatientsdidnotrequired med-ication tominimize their symptomsand the pain wasnot disablingfortheirwork.
EAEI
EAI
CAM
CAS EAI
EAE
Anterior
A
B
Posterior
EAE–PR
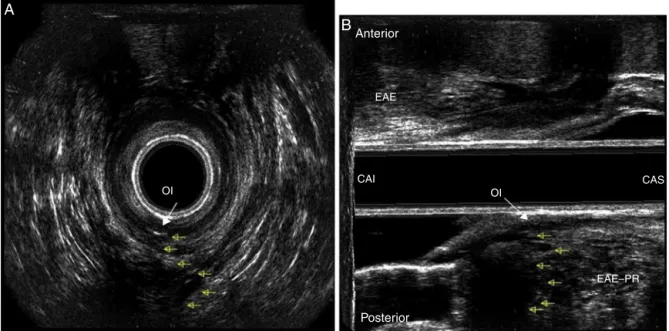
Fig.1–Presenceofanintersphinctericinflammatory-infectiousprocess(yellowarrows)inthemiddleanalcanal(MAC). EAS,externalanalsphincter;IAS,internalanalsphincter(whitearrows);A,axialsection;B,sagittallongitudinalplane.
fromColoproctologicalService,atGastroclínicade Cascavel Ltda.,byasingleexaminer(DMRL).
Thedeviceused wastype 2050BKMedical® ultrasound
withafull360◦fieldprobe.Afterundergoingbowelpreparation
withafleetenema2hbeforethetest,thepatientswere exam-inedintheleftlateralposition.Digitaltouchwasperformed and then the transducer was inserted and positioned into theanalcanal.Theimageswereacquiredbytwoautomatic
scans inmen–corresponding tothe anal canalandlower rectum,respectively–andthreeinwomen–corresponding totheanalcanal,lowerrectumanddynamicexamination.8
Theanalcanalscanningwasperformedwiththetransducer at6cmfromtheanalmargin;thedynamicexaminationwas performedat7cmfromtheanalmargin;andthelowerrectum scanningwasheldatapoint10cmfromtheanalmargin.The cube-view3Dimageswereanalyzedintheaxial,transverse,
OI
OI CAS
CAI EAE Anterior
A
B
Posterior
EAE–PR
EAI
CAS EAI
1
1 2
EAI CAI
EAE
EAE
A
Posterior
EAE–PR
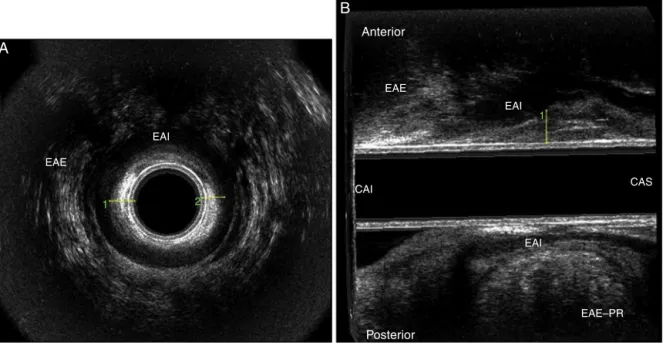
Fig.3–Increaseinthethicknessofthesubepithelialtissue(mucosalprolapse)inmiddle(MAC)andupper(UAC)analcanal. A,axialsectioninMAC;B,sagittalsection.
sagittaland diagonalplanes.Thesphincterintegrityinthe anal canal and walls of the rectum and perianorectal tis-suewasevaluated.Theidentificationofasubepithelialtissue thickeningwithmeasurementsexceeding0.3cmmay corre-spondtoamucous-haemorrhoidalprolapse.9Thismeasure
wasobtainedinthemiddleandupperpartsoftheanalcanal, atthe9and6o’clockpositions.
The sonographic findings indicative of an intersphinc-tericinflammatory-infectiousprocesswerecharacterizedby ahypoechoic,irregular,heterogeneouscavity,oftenwithpoor echoesinside,betweentheexternalandinternalanal sphinc-ters in the middle anal canal, between the internal anal sphincter and the puborectalis muscle in the upper anal canal, and in the ischiorectal fossa in the lower rectum.
EAI
1
3 2
1
EAI
EAE EAE
Vagina
Repouso Repouso
Esforco evacuatorio
A
B
Fig.5–Presenceofahypoechoiccircularimageinmiddleandlowerrectum–retrorectal(presacral)cyst:delimitationofthe cyst(arrows).A,axialsection;B,sagittallongitudinalplane.
Theretrorectalcystwascharacterizedforbeinganirregular, hypoechoic,cysticimagelocatedposteriortothewallsofthe middleandlowerrectum.10Theimageobtainedbydynamic
echodefecographywasconsideredasarectocelewhena differ-enceintheposteriorvaginalwallpositionatrestandduring strainingwasnoted.8Sphincterinjurywascharacterizedas
a hypoechoic interruption of muscle fibers of the internal anal sphincter and a hyperechoic interruption of external sphincter.11
Thefollowingvariableswereassessed:age,gender,parity, andprevioushistoryofanorectaldiseaseand/orsurgery.
Patientswithanalpaincomplaintsandwithproctologic orcolonoscopicfindingswhichwouldjustifythepain,such ashemorrhoids,fissures,fistulae,hypertrophicpapillaeand inflammatoryboweldisease,aswellaspatientswithahistory ofpreviousorificialsurgeryandfemalepatientswithchanges ingynecologicalexaminationswereexcludedfromthestudy.
Results
The results indicated an intersphincteric inflammatory-infectiousprocessoftheupperanalcanalandlowerrectum andinthemiddleanalcanalin14patients(63.6%)(Fig.1).In onepatient,aninternalfistulaopeningat6o’clockpositionin themiddleanalcanalwasfound,suggestingthepresenceof analfistula(Fig.2).
Thethicknessofthesubepithelialtissuewashigherthan normal,suggestingahaemorrhoidalmucousprolapseinthe middleand upperanal canalin threepatients (13.6%)The thicknessofthesubepithelialtissuewashigherthannormal, suggestingthepresenceofahaemorrhoidalmucousprolapse inthemiddleandupperanalcanalinthreepatients(13.6%)
(Fig. 3). Two female patients(9.1%) presentedwithananal sphincterinjury,oneofthembeingintheinternalanal sphinc-terinthepresenceofagradeIIrectocele,andtheotherinthe externalanalsphincterinthedistalandanteriorpartsofthe middleanalcanalnotaccompaniedbyarectocele(Fig.4).
Inonepatient(4.6%),theexaminationrevealedthe pres-ence ofahypoechoiccircularretrorectalcyst inthemiddle andlowerrectum(Fig.5).The3D-USexaminationrevealedno abnormalitiesintwosubjects(9.1%).
Discussion
Ultrasonographyhasawell-definedroleintheevaluationof benignandmalignant anorectaldiseases,becausethis pro-ceduredemonstratespreciselytheanatomicalstructuresthat formtheanalcanal,rectumandperi-anorectaltissues.Inthis study,anorectalchangeswereidentifiedin91.9%ofpatients and adiagnosis ofidiopathic proctalgia wasestablishedin 9.1%.Inastudypublishedin2008,theauthorsidentifiedthe causesofpainin82%ofcases.12In2010,anotherstudy
iden-tifiedspecificorganiccausesofdiseasein49%ofcases.13
Thedifficulties indiagnosingintersphinctericsepsisare welldocumented,thankstotheabsenceofexternalclinical signs suchasswelling,indurationorperianal hyperemia.14
Thus,anearlydiagnosisandeffectivetreatmentofferbetter postoperative functional outcomes.15 In this study,
inter-sphinctericsepsiswasdiagnosedin14patients(63.6%),and the path and internalfistulous orifice were evidenced ina patient.
Beer-Gabel et al.16 demonstrated that changes such as
identified inrelation todefecation was asubepithelial tis-suethickening,suggestingmucous-haemorrhoidalprolapse in 13.6%,and this may be the cause ofanal pain. In two femalepatients,thepresenceofananalsphincterinjurywas evidenced.
Other causes of anal pain that should be considered, despite its low incidence, are perianal endometriosis and perinealorretrorectal tumors.Inonepatient, thepresence of a retrorectal cyst of the middle and lower rectum was evidenced.
Mostofthetime,analpaindoesnotmeanalesionof malig-nantnature,however,itdecreasesthepatient’squalityoflife ifnotdiagnosedandwithout propertreatment.Ultrasound helpstodemonstratethewholeanatomyoftheanalcanal, allowingaclearunderstandingofpossiblecausesofanalpain, hencetheusefulnessofthetest.Thus,functionalcausesare removedfromanatomicalcauses,allowingtheestablishment ofaspecifictherapyforeachcase.
Conclusion
Thethree-dimensionalanorectalultrasoundisasimple, cost-effective,fast and usefulmethod inthe studyofanorectal diseasesandshouldbeincludedinthestudyofpatientswith analpain,withtheaimtoruleoutorganiccauses.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. BharuchaAE,WaldA,EnckP,RaoS.Functionalanorectal
disorders.Gastroenterology.2006;130:1510–8.
2. SwashM.Chronicperianalpain.In:HenryM,SwashM,
editors.Coloproctologyandthepelvicfloor.London:
Butterworths;1985.p.388–92.
3. CheungO,WaldA.Managementofpelvicfloordisorders.
AlimentPharmacolTher.2004;19:481–95[Review].
haemorrhoidectomy.BrJSurg.1998;85:1522–4.
5.MillanM,García-GraneroE,EsclápezP,Flor-LorenteB,EspíA,
LledóS,etal.Managementofintersphinctericabscesses.
ColorectalDis.2006;8:777–80.
6.TarantinoD,BernsteinMA.Endoanalultrasoundinthe
stagingandmanagementofsquamous-cellcarcinomaofthe
analcanal:potentialimplicationsofanewultrasoundstaging
system.DisColonRectum.2002;45:16–22.
7.KimJC,ChoYK,KimSY,ParkSK,LeeMG.Comparativestudy
ofthree-dimensionalandconventionalendorectalultra
graphyusedinrectalcancerstaging.SurgEndosc.
2002;16:1280–5.
8.Murad-RegadasSM,RegadasFSP,RodriguesLV,EscalanteRD,
SilvaFRS,LimaDMR,etal.Ecodefecografiatridimensional
dinâmica.Novatécnicaparaavaliac¸ãodasíndromeda
defecac¸ãoobstruída(SDO).RevBrasColoproct.
2006;26:168–77.
9.Murad-RegadasSM,RegadasFSP.Ultra-sonografiaanorretal
bietridimensional.In:Murad-RegadasSM,RegadasFSP,
editors.DistúrbiosFuncionaisdoAssoalhoPélvico-Atlasde
Ultra-sonografiaAnorretalBieTridimensional.RiodeJaneiro:
Revinter;2006.p.51–78.
10.Murad-RegadasSM,RegadasFSP.Miscelanias.In:
Murad-RegadasSM,RegadasFSP,editors.Distúrbios
funcionaisdoassoalhopélvico-AtlasdeUltra-sonografia
AnorretalBieTridimensional.RiodeJaneiro:Revinter;2006.
p.342–62.
11.SantoroGA,DiFalcoG.Basicanatomy.In:SantoroGA,Di
FalcoG,editors.Atlasofendoanalandendorectal
ultrasonography.Milán:Springer;2004.p.25–42.
12.PascualI,García-OlmoD,Martínez-PuenteC,
Pascual-MonteroJA.Ultrasoundfindingsinspontaneous
andpostoperativeanalpain.RevEspEnfermDig.
2008;100:764–7.
13.VieiraAM,Castro-Poc¸asF,LagoP,PimentelR,PintoR,Saraiva
MM,etal.Theimportanceofultrasoundfindingsinthestudy
ofanalpain.Ultrasoundfindingsinthestudyofanalpain.
RevEspEnfermDig.2010;102:308–13.
14.OnacaN,HirshbergA,AdarR.Earlyreoperationforperirectal
abscess–apreventablecomplication.DisColonRectum.
2001;44:1469–73.
15.Garcia-AguilarJ,BelmonteC,WongWD,GoldbergSM,Madoff
RD.Analfistulasurgery.Factorsassociatedwithrecurrence
andincontinence.DisColonRectum.1996;39:723–9.
16.Beer-GabelM,TeshlerM,SchechtmanE,ZbarAP.Dynamic
transperinealultrasoundvs.defecographyinpatientswith