BrazJOtorhinolaryngol.2016;82(6):737---740
www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
CASE
REPORT
Hoarseness:
an
unusual
presentation
of
primary
thyroid
lymphoma
with
laryngeal
infiltration
夽
Rouquidão:
apresentac
¸ão
incomum
de
linfoma
primário
de
tireoide
com
infiltrac
¸ão
da
laringe
Ozan
Gökdo˘
gan
∗,
Ahmet
Koybasioglu,
Erkin
Ismail,
Timucin
Erol,
Gokcen
Alagoz,
Banu
Yagmurlu,
Seref
Komurcu
AnkaraMemorialHospital,DepartmentofOtorhinolaryngology,Ankara,Turkey
Received11February2015;accepted3May2015 Availableonline7September2015
Introduction
Primary thyroid lymphoma is a relatively rare disease of the thyroid gland. PTL represents approximately 1%---5% of thyroid malignancies and less than 2% of extra nodal lymphomas:theprognosisisgenerallygood.1Thyroid
lym-phomasaremorecommoninwomenwithapredominance of3---4:1.2
The main clinical manifestation is a rapidly enlarging thyroid mass, commonly in the seventh decade. Approxi-mately30%---50%ofpatientsmanifestcompressionsymptoms of the adjacentstructures, in additiontodysphagia, stri-dor,hoarseness,coughandapressuresensationintheneck. Symptomssuchasfever, nightsweatsand weightlossare less common.Hashimoto’sthyroiditisappears tobearisk factorforthyroidlymphomaalthoughtheassociationisstill debated.1,2
The most common histopathological type of thyroid lymphomas is non-Hodgkin’slymphoma withB cellorigin. Hodgkin’sdiseases andT-cell lymphomas areraretumors.
夽 Pleasecitethisarticleas:Gökdo˘ganO,KoybasiogluA,IsmailE,
ErolT,AlagozG,YagmurluB,etal.Hoarseness:anunusual presen-tationofprimarythyroidlymphomawithlaryngealinfiltration.Braz JOtorhinolaryngol.2016;82:737---40.
∗Correspondingauthor.
E-mail:[email protected](O.Gökdo˘gan).
Patients with pure mucosa associated lymphoid tissue (MALT) lymphomas tend to demonstrate a more indolent courseandabetterprognosiscomparedwithpatientswith diffuse large B-cell types or mixed histological subtypes, whichmayhaveamoreaggressiveclinicalcourse.3
Ageneral 5-yearsurvivalrate for PTLis approximately 90%; therefore a well-planned treatment after rapid and accuratediagnosisgenerallyresultsingoodprognosis.4
Case
report
A52-year-old-womanwasadmittedtothe otorhinolaryngo-logyservicebecauseofatwo-monthhistoryofhoarseness andleftotalgia.Nobreathingorswallowingcomplaintswere present.Priortoadmissiontoourclinic,medicaltreatment hadbeenprovidedforhertwiceforlaryngitis,buther com-plaintsdidnotimprove.
She reported a history of diabetes mellitus, hyperten-sion and hypothyroidism (chronic lymphocytic thyroiditis) andalsocholecystectomy.
On physical examination, theleftvocal cordwasfixed in themidline and fullness onleft false vocal cordcould beobserved.Thethyroidlobesdemonstratednodules bilat-erallyandwereenlarged,withthe leftlobebeingslightly firmer and larger than the right. There were no cervical palpablemassesorlymphadenopathy.
http://dx.doi.org/10.1016/j.bjorl.2015.05.006
738 Gökdo˘ganOetal.
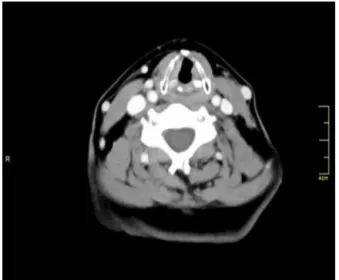
Figure1 Laryngealinfiltrationwithcartilageinvasionof thy-roidmass.
Thyroidfunctiontestswerewithinnormalrangealthough she wasusing thyroid hormones for hypothyroidism. Thy-roidbiopsyhadbeenperformed2yearspreviouslyandthe histopathologicreportrevealedachroniclymphocytic thy-roiditis.
On radiologic evaluation masses in the leftfalse vocal corderodingtheleftthyroidcartilage,continuouswiththe thyroidgland,wereobserved.Therewerenodulesinboth thyroidlobes(Fig.1).
Alaryngealpathologyoriginatingfromtheleftlaryngeal structuresthaterodedthyroidcartilageandextendedtothe thyroid glandwas considered after examination. A direct laryngoscopyandbiopsyprocedurefrombothleftlaryngeal ventriclesandafineneedlethyroidbiopsyfromnodulesof boththyroidlobeswasplanned.
Biopsyof theleftfalsevocal cordwasreportedas dif-fuse large B cell lymphoma. Fine needle aspiration from both thyroid lobes was reported as atypical lymphocytes (Figs.2and 3).The prognosticfactorsof lymphomawere diagnosed as follows: proliferative index of Ki 67 was 80%---90%,LDH (lactatedehydrogenase)andsedimentation wasnormal.Thepatientreportedweightlossof20kginthe
Figure 2 Diffuse lymphoid infiltrations under laryngeal mucosa(with100×magnificationonpathologicexamination).
Figure3 Tumoriscomposedofatypicallymphoidcells,which havealargevesicularnucleolusandsignificantnucleolus.These cellshavepositive membranouspositivity withCD 20marker (with400×magnificationonpathologicexamination).
last4months.Internationalprognosticindex(IPI)scorewas foundas0.
Afludeoxyglucose-positronemissiontomography (FDG-PET) scan for differentiating the lesion between primary thyroidlymphomaorthyroidinvolvementofasystemic dis-ease showedonly diffuse involvementin leftthyroid lobe (Fig.4).
As a result of these diagnostic tests patient was diagnosed as diffuse large B cell primary thyroid lym-phoma, stage 1E. She received 3 courses of R-CHOP (rituximab---cyclophosphamide,doxorubicin,vincristineand prednisolone) treatmentand involved-fieldradiation ther-apy following chemotherapy. Her treatment course was uneventful and her hoarseness improved after treatment (Fig.5).
A team including oncology, radiation oncology, oto-rhinolaryngology, endocrinology departmentsfollowed the patientevery monthafter chemoradiationtreatment. She continues thyroid replacement treatment. Her thyroid is nowgrade3palpableindiffuseandhardpattern.There can-notbeidentifiedanynodularpatterninexamination.Both
Primarythyroidlymphomawithlaryngealinfiltration 739
Figure5 Neckcomputedtomographyaftertreatmentshows onlyminimallylaryngealedema,withoutanymassinboth lar-ynxandthyroidgland(onemonthaftertreatment).
vocal cords aremobile and there is no visible pathologic findinginlaryngealevaluation.
Six monthsafter chemoradiationtherapythepatientis nowinagoodhealthwithoutanycomplaint.Herphysical, laboratory,laryngealandradiologicevaluationiscompletely normalwithoutanyevidenceofrelapse(Fig.6).
Discussion
Extranodal lymphomas are usually seen as non-Hodgkin’s lymphoma (NHL) which constitute 10%---29% of all lym-phomas. Adult NHLs commonly arise from B cells. The main clinical symptom is an enlarging mass in head and neckregion,whichmayalsomanifestadestructiveclinical progress.
ExtranodalmarginalzoneB-celllymphomaofMALTtype mayoccur in thestomach, orbit,intestine, lung, thyroid, salivarygland,skin,softtissues,bladder,kidneyandcentral nervous system. The most common extranodal extralym-phaticsites are theparanasal sinuses,the salivary glands andthethyroidgland.4
Figure6 Neckcomputedtomographysixmonthsafter treat-ment.Laryngealedemahasdecreasedalittlemoreovertime.
The larynx is a rare site for localization of a primary NHL because of relatively low lymphoid content. In the literature,there arefewer than 100 cases of lymphopro-liferative tumors arising from the larynx (including both NHL and immunosuppression-related lymphoproliferative diseases)andfewcasesoflaryngealinfiltrationofPTLhave beenreported.ThereisnoreportedcaseofPTLpresenting with hoarseness and diagnosed through direct laryngo-scopic biopsy, since it typically does not erode thyroid cartilage.
Primaryorsecondarylaryngealpathologiesmaymanifest similarsymptomsincludingdysphonia,hoarseness, dyspha-gia:a cervical mass can be found. A smooth submucosal swellingorpolypoidmasswithout ulcerationaretheusual physical examination findings of primary laryngeal lym-phomas. Primary laryngeal lymphomas usually arise from thesupraglotticregion,specificallyfromtheepiglottisand aryepiglotticfolds.5Ourcasealsodemonstratessupraglottic
infiltrationespecially inleftlaryngeal ventricule. Extrala-ryngealtumorextensionismostfrequentlynotedtoinvolve the hypopharynx, and less commonly the oropharynxand strapmuscles.
PTL is a lymphamatous process which develops in the thyroid without involvement of primary lymphoid organs or distant metastasis at the time of diagnosis. PTL com-prises2%---8% of thyroidmalignancies. It ismostly seen in a middle-aged elderly women with a median age of 56 years. Patients usually have a history of hypothyroidism orthyroiditisand massin thyroidglandwhich canrapidly grow.Dyspnea,stridor,dysphagia,andhoarsenessare com-monsymptoms in patients with thyroid lymphoma, while mainfindingmayonlybeanenlargingcervicalmasswhich presentsinover87%ofpatients.HoweverPTLmaysuddenly growandcompromisetheairway.
Themajorityof PTLsarehighgradewhile only30%are low-grade.Earlydiagnosisandappropriatetreatmentof thy-roidlymphomascanprovidelongtimesurvival.3
Anaplastic thyroid cancers (ATC) also present with a rapidlygrowing large mass in elderly patients. Anaplastic thyroidcancers,whichcompromise1%---2%ofthyroid malig-nancies,havesimilarclinicalprogressandmustbeincluded in the differential diagnosis of thyroid lymphomas. ATC’s mayrapidlyprogress andcompromisetheairwaywithan averagemeansurvivalof6---7months.Onradiologic evalu-ationATCispresentsasalarge,solidmassaccompaniedby necrosis, hemorrhage, dense calcification, directinvasion ofadjacentstructuresandcervicallymphnodemetastasis. Tumornecrosishasbeenknowntobeoneofthemost valu-ableparametersin differentiatingATC fromother thyroid masses, and low attenuation value on post contrast scan (attenuationvalue<100HU)isanotherpredictorof anaplas-ticcarninoma.6
740 Gökdo˘ganOetal.
Fineneedleaspirationwithor without ultrasonography isthefirststepindiagnosticstrategyforathyroidnodule, butaccuracyisquitelowinthyroidlymphomaoranaplastic cancer. The diagnostic approaches for an enlarging thy-roidmassareFNA,core needlebiopsy(CNB),openbiopsy, and/orsurgical intervention.Thediagnostic effectof FNA identifies30%---80%ofthyroidlymphomapatients;therefore furtherdiagnostic approaches maybe useful when FNAis inconclusive.8Coreneedlebiopsy(CNB)generallyprovides
enoughtissueneededforthecertaindiagnosisofaggressive thyroidcancerslikelymphomaorATC.ThereforeCNBmay bethefirstdiagnosticstepwhenalargeaggressivethyroid massisencounteredonradiologicevaluation.
Histological and phenotypic analyses such as flow cytologyorimmunohistochemistryareveryhelpfulin patho-logicalevaluation.MostthyroidlymphomasareB-cellorigin withdiffuselarge-celltype.
Mostpatientspresent withearlystagesIE(30%---66%)or stageIIE(25%---66%)disease.9Forstaging,CTscansofhead,
neck,chest,abdomenandpelvisorFDG-PETscanshouldbe performed.
Treatmentoptionsconsistofchemotherapyalone, radia-tiontherapyaloneandcombinedchemo-radiationtherapy. Although there are some articles that advise thyroidec-tomy followed by radiation therapy, the series reported aretoosmalltoacceptaswidespreaduse asatreatment option.
The overall relapse rates are 7.7%, 37.1% and 43% for chemoradiation therapy, radiation therapy alone, and chemotherapy alone respectively. Local relapse rates are 2.6%,12.6%and23%forchemoradiationtherapy,radiation therapyalone,andchemotherapyalonerespectively.1
The most common chemotherapy regimen is R-CHOP (rituximab---cyclophosphamide,doxorubicin,vincristineand prednisolone).Thebiologicagentrituximab,amonoclonal antibody directed against B-cell-specific antigen CD 20 is generallyusedwithCHOP chemotherapyin thetreatment ofthyroidlymphoma.
Radiotherapyisgenerallychosenafter3---6CHOPcourses intheformofmodifiedmantleirradiation,includingthyroid, bilateralneck,supraclavicularareaandmediastinum.
Age(>60years),elevatedlevelsofserumlactate dehy-drogenase (LDH), and 2 macroglobulin, extra nodal site
involvementandstageIII---IVclassificationarepoor progno-sticfactors.10
Ourpatientreceived R-CHOP basedchemotherapy and radiotherapyandisalivewithoutanysignofdisease.
Conclusion
The present reportdetails the firstknowncase diagnosed with thyroid lymphoma through direct laryngoscopy and biopsy.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.MackLA,PasiekaJL.Anevidence-basedapproachtothe treat-mentofthyroidlymphoma.WorldJSurg.2007;31:978---86. 2.RuggieroFP,FrauenhofferE,StackBC. Thyroidlymphoma:a
single institution’sexperience. Otolaryngol Head Neck Surg. 2005;133:888---96.
3.SteinSA, Wartofsky L. Primary thyroid lymphoma:a clinical review.JClinEndocrinolMetab.2013;98:3131---8.
4.AlzouebiM,GoepelJR,HorsmanJM,HancockBW.Primary thy-roid lymphoma: the 40 year experience of a UK lymphoma treatmentcentre.IntJOncol.2012;40:2075---80.
5.Siddiqui NA, Branstetter BF, Hamilton BE, Ginsberg LE, Glastonbury CM, Harnsberger HR, et al. Imaging character-istics of primary laryngeal lymphoma. Am J Neuroradiol. 2010;31:1261---5.
6.GreenLD,MackL,PaseiekaJL.Anaplasticthyroidcancerand primarythyroidlymphoma:areviewoftheserarethyroid malig-nancies.JSurgOncol.2006;94:725---36.
7.PedersenRK,PedersenNT.Primarynon-Hodgkin’slymphomaof thethyroid gland: a populationbased study.Histopathology. 1996;28:25---32.
8.CooperDS,DohertyGM,HaugenBR,KloosRT,LeeSL,Mendel SJ,etal.Revised AmericanThyroidAssociationmanagement guidelinesforpatientswiththyroidnodulesanddifferentiated thyroidcancer.Thyroid.2009;19:1167---214.
9.Graff-BakerA, RomanSA,ThomasDC,Udelsman R,Sosa JA. Prognosisofprimarythyroidlymphoma:demographic,clinical, andpathologicalpredictorsofsurvivalin1408cases.Surgery. 2009;146:1105---15.