The medication process, workload and
patient safety in inpatient units
Ana Maria Müller de Magalhães1, Gisela Maria Schebella Souto de Moura1, Simone Silveira Pasin2, Lia Brandt Funcke1, Bruna Machado Pardal1, Angélica Kreling1
Processos de medicação, carga de trabalho e a segurança do paciente em unidades de internação
Procesos de medicación, carga de trabajo y seguridad del paciente en las unidades de hospitalización
1 Universidade Federal do Rio Grande do Sul, Escola de Enfermagem, Porto Alegre, RS, Brazil. 2 Universidade Federal do Rio Grande do Sul, Hospital de Clínicas de Porto Alegre, Porto Alegre, RS, Brazil.
Received: 01/10//2015 Approved: 07/5/2015
Original article DOI: 10.1590/S0080-623420150000700007
aBStract
Objective: To conduct a survey of critical points in the medication process, its repercussions on the demands made on the nursing team and risks related to patient safety. Method: his was a qualitative descriptive study that adopted an ecological-restorative approach. he data were collected through focus groups and photographs. Participants consisted of nurses and nursing technicians. Results: hree categories emerged from the thematic analysis: challenges related to the process of prescribing and dispensing medication; medication administration with relation to work shift organization; and the use of new technologies to reduce medication errors. he results indicated that the medication process plays a central role in organizing nursing care, being that these professionals represent the last barrier for detecting medication prescription and administration errors. Conclusion: By identifying vulnerabilities in the medication administration phase, the use of technology can help ensure patient safety.
DeScriPtOrS
Workload; Nursing, Team; Medication Systems, Hospital; Medication Errors; Patient Safety.
Correspondence Addressed to: Ana Maria Müller de Magalhães
Rua Dr. Barbosa Gonçalves, 500 - Chácara das Pedras
CEP 91330-320 – Porto Alegre, Rio Grande do Sul, Brazil
INTRODUCTION
he topic of patient safety has been at the center of dis-cussions by the main health organizations in the world, es-pecially over the last two decades. Studies published by the
Institute of Medicine(1) and the World Health Organization(2) have unleashed a global movement about issues involving the risks of errors or failures that can cause harm to or even the death of patients in existing healthcare systems. he theme of patient safety refers to a broader range of themes intrinsic to and integrally related to it.
here is growing evidence that the workload of hospital nursing teams is associated with patient safety; nonetheless, there are still gaps in knowledge regarding the nature of the relationship between nursing workload and patient safety.
A study involving nursing staf found that high nurs-ing workload led to poorer surveillance of patients and greater risk of adverse events(3). However, despite these international initiatives to measure workload and estab-lish minimum nursing staf in inpatient care, this is still a distant goal in Brazil(4-5).
A Brazilian study investigated the association between nursing workload and the safety of hospitalized patients. he results showed that the nursing team reported medi-cation administration as one of the factors associated with high workload. hey also showed that the higher the num-ber of patients per professional, the greater the risk associ-ated with care, i.e., the more likely the occurrence of errors that afected patients, such as those involving medication preparation and administration(6).
Similar indings have also been emphasized in other Bra-zilian and international studies, which have demonstrated that activities related to the medication process have the most impact on nursing workload. Furthermore, these studies have also shown that timing errors are among the most common in relation to work shifts with a higher number of patients(7-9).
A Canadian study found that one in every seven hospi-talized patients in clinical inpatient units had experienced at least one adverse event related to nursing care, an incidence of 18.5 per 1000 patients per day. hese results indicated that the most common adverse events were patient falls (5.9%) and medication administration errors (5.5%)(10).
Hospital medication processes consist of several phases, starting with medical prescription, transferring or verifying prescriptions, and then dispensing and administering medica-tions. he administration of one drug alone can involve 30-40 steps, and with each step, the risk of error increases(11).
Practical experience with nursing, teaching and research has shown that this process is organized diferently in dif-ferent health institutions, both regarding the phases of the medication process and at the level of computerization, auto-mation, and the use of technologies. he diferent realities in the hospital setting make it diicult for nursing professionals to master the knowledge and skills needed to deal with such complex processes.
In light of these considerations, it can be said that the medication process is a fundamental factor in patient care and recovery, representing a central element of work organization
in hospital nursing. he risks associated with patient safety and the high cost of medications to the system point to the need for better understanding of all the phases involved in the process in order to ind solutions that reduce medication er-rors and patient harm.
his study aimed to describe how work was organized at the teaching hospital and identify critical points in the medi-cation process, in addition to its repercussions on the job de-mands of the nursing team, which can represent risks to the safety of hospitalized adult patients.
METHOD
his was an exploratory, descriptive and qualitative study, conducted within the perspective of ecological and restor-ative thought. his study design, anchored in previous stud-ies, allowed for an in-depth analysis of the theme in focus, as new variables were explored, leaning towards the discovery of unknown dimensions that could generate hypotheses and theories for explaining the phenomenon studied(6,12-16)
. he study was developed in three clinical inpatient units at a university teaching hospital in the south of Brazil. It was approved by the institution’s ethics committee under num-ber 12-0332. he data were collected between January and June 2014 in three phases, following the assumptions of the participatory photo-elicitation methodology and adapted to the ield of ecological restoration(6, 12-14).
Each of the three units contained 45 beds. he nursing team in each unit consists of 15 nurses and 45 nursing tech-nicians, distributed among ive work shifts (morning, after-noon and three diferent nights). Among other activities, the nursing team was responsible for inding medication in the hospital pharmacy and designating an afternoon nursing technician to update and review all drug prescriptions.
Convenience sampling was used to select participants and consisted of four nurses and 14 nursing technicians who were willing to participate in the study after being invited to do so by the research team.
A focus group was conducted in the irst phase to discuss the safety of medication processes and create the itinerary of the photo walkabout. he group was encouraged to discuss how medication processes occur in their work routines, in addition to the implications that these processes bring to the organization of work shifts and the risks related to patient care. Four nurses and seven nursing technicians participated in the irst focus group.
errors. he narrative of the pictures as told by participants was recorded during the walkabout.
In the third step, a focus group was convened for the process of photo-elicitation, in which 25 pictures were se-lected for review with the participants in order to bring to light their ideas about and experiences with, the safety of the medication process in the studied units. Four nurses and nine nursing technicians took part in the second focus group. All of the nurses and some of the technicians partici-pated in both focus groups.
All of the participants read and signed an informed con-sent form before participating in the focus groups and photo walkabout. Other staf members, patients and family mem-bers also signed a consent form after being informed about the research, agreeing to have photos taken of their health-care environment. he procedures used in this study abided by Resolution no. 466 of the Brazilian National Council of Health(17) regarding research with human subjects. Group participants were identiied with the letter “P”, followed by a sequential number.
he information collected was organized into iles us-ing NVivo 10 software. his qualitative data analysis tool led to the organization of the diferent sources of data, which consisted of both the literal transcription of the focus group discussions and photograph narratives and the audio record-ings, digital photos, ield notes, forms, and itineraries that guided the image-capturing process.
Following the steps of pre-analysis, exploration of the material, result processing, inference and interpretation, the study irst sought to identify and code emerging themes and then group them by similarity of content and construct.
hese categories helped describe and comprehend the inves-tigated phenomenon(18).
he researchers aimed to immerse themselves in the data in order to codify them, using an inductive form of content analysis, and avoided using pre-conceived categories, allow-ing the themes and their groupallow-ing into categories to low di-rectly from the raw data. Categorization was conducted in-dependently by three researchers, followed by meetings with the research team to validate the relevance of the themes and the categories found.
RESULTS
he empirical material that resulted from the focus group discussions, the photographs taken during the photo walkabouts, and ield observations and notes were grouped into three categories, as described below.
he irst category – challenges related to the process of prescribing and dispensing medication – contained themes relative to the phases that precede medication administration. In the focus group and photo-elicitation process, participants discussed aspects about the partially computerized processes of medication prescription, sched-uling, and veriication. hey also discussed how medica-tions were dispensed by the pharmacy.
Medical prescription were written out electronically, however, nurses were responsible for reviewing and adjust-ing the electronic scheduladjust-ing. hey also were responsible for verifying the prescriptions, re-scheduling them man-ually, and locating medications in the pharmacy. Some of these issues are illustrated in the following excerpts and in Figure 1, which portrays the transportation of medication from the hospital pharmacy to two of the researched units:
(...) The greatest load from my point of view is the pharmacy. It stresses us out, we have to administer an injection but we have go to the pharmacy sometimes five or six times before getting that medication (P2).
One staff member is responsible for medication, she goes to the pharmacy several times, for there are many inclusions[medications] in our unit (...) she carries several super heavy bags (...) but for now that’s what we’re able to do, as the hospital has a transparent bag for carrying medications (P7).
(Source: Focus Group 1, January 28, 2014)
Figure 1 - Transporting medication from the pharmacy to the units– Porto Alegre, Rio Grande do Sul, Brazil, 2014. (Source: Photo walkabout, June 3, 2014)
he computerized prescription system resulted in a distance between the medical and nursing teams, who reported miscom-munication regarding the inclusion and removal of medication from patient prescriptions. he system had no mechanism to warn the nursing team about such changes. he participants al-so reported prescription errors in the computerized documents:
(...) But not only about error, or administering the wrong medication… Even the prescriptions, I was there with a patient whose wristband read that he was aller-gic to Plasil, with Plasil prescribed right there… (P3).
We only look at the prescription at the end of the day… nobody looks at the prescriptions all the time, if there has been a change. If you don’t inform me about the change you made this morning, there’s no way I’m going to know… (P7).
(...) he nurse arrives at 6 pm. If there is no pres-cription, she will print out the prespres-cription, then they arrive and write the prescription at 18:30. But they don’t tell us and nobody goes there to print another prescription. (...) So there’s an antibiotic missing… because we were not informed of this inclusion. hey don’t tell us, so the next morning they come in and want to know why we didn’t start the antibiotic the previous night (P7).
(Source: Focus Group 2, June 27, 2014)
he second category – medication administration in relation to work shift organization – consisted of themes that portrayed how the nursing team organized itself to carry out the inal phase in the medication process, medi-cation administration. Participants reported that
medica-tion administramedica-tion was a central task in their work shift. In general, it was always the irst activity to be veriied and carried out, as illustrated in the excerpt below:
(...) his is where shift handofs happen…and step by step, this is what we do: we arrive at the unit, check the patient transfer schedule, bed distribution, and then we get our work material: which is a spreadshe-et. hen we go through the drawers with the medical prescriptions. hen we get the prescriptions and the patient labels (P5).
(Source: Photo Walkabout, June 03, 2014)
he activities in a given nursing shift began by set-ting apart the medications to be administered to patients during their work shift. Figure 2 illustrates the packag-ing of individualized medications by patient bed, each drawer corresponding to a three-bed ward and each compartment containing a patient’s medication for a period of 24 hours. his igure also shows the nursing technician’s medication cart that is transported to the patient’s bedside.
Figure 2 - Medication drawer at the nurses’ station and a cart prepped for administration - Porto Alegre, Rio Grande do Sul, Brazil, 2014. (Source: Photo Walkabout, June 02, 2014)
he focus group discussions emphasized that organiz-ing and retrievorganiz-ing drawers and preparorganiz-ing medications took up much of the work shift. In addition to these activities, they also had set aside time to ill out each medication identiication label by hand, take the drugs to the patient and administer them. At the moment of patient admission, the labels are automatically printed out with a barcode, the patient chart number and the patient’s full name. However, nursing technicians must ill in the name of the medica-tion, dose, day, administration time and signature by hand. According to the participants, this task demands much attention and concentration, as they were responsible for verifying a great amount of medication, illing out the labels and prepping them for administration. hey did not know
the exact number of medication prepared per shift, but they knew the average number of patients cared for per shift.
he printed label contains only the patient’s name, so then we have to get it, write the name of the medica-tion, the patient’s bed, the dose, and so much time is lost writing it all down. And we have seven or eight patients… (P10).
(Source: Focus Group 1, January 28, 2014)
(...) Filling out all that information which, I re-peat, brings us security, but this process of illing them out takes up time that is later relected at the patient’s beside (P1).
Medication was prepared at the nurses’ station, close to the medication drawers. he pills were dispensed by the hospital’s pharmacy in individual packages. Other types of medication were aspirated, reconstituted, diluted, fractioned or ground by nursing technicians for adminis-tration. In this phase, there were many doubts about drug dilution, dose calculation and the instructions contained in the pharmacy manual, which were not easy to understand, as shown in the following excerpts:
(...) hat little book on drug dilution is sort of compli-cated too… Granted, we need to think, but you have to think too much with that thing. You even have to ask the university students for help (P2).
(...) No, it’s the instruction. You can’t cut the medica-tion, you have to dilute the whole thing and aspirate the content that you need. hat’s the right way to do it, that’s what the instructions say. (P7).
(Source: Focus Group 1, January 28, 2014)
(...) How are we supposed to dilute the drug if the powder falls under the syringe when you’re doing it, how are you going to dilute the right dose? (P5).
(Source: Focus Group 2, June 27, 2014)
After this phase, medications were ready to be taken and administered to patients. During the group discus-sions, participants underscored that this process required a high level of concentration, but that the workplace dy-namics usually did not allow nursing technicians to follow through with their initial plan and meet all of them with-in the established deadlwith-ines, resultwith-ing with-in delays with-in medi-cation administration. hese interruptions and changes in the shift activities were due to patient and family requests, changes in medication prescription, lack of availability of equipment or materials, in addition to other patient care procedures, such as baths, hygiene, dressings, and feeding.
hen we’re going to administer an injection, we have to put everything away or else it’s not possible: let the phone ring… sometimes you have the medication, the phone is ringing, a family member is calling, then you drop everything to do something else and in the me-antime you forget what you were doing (P2).
Because it’s a very complex process, you take a shift, then you go see a patient, you prepare administration, then you have to administer it, then there’s the bath, diaper change, you lots of things to do (P11).
(Source: Focus group 1, January 01, 2014)
(...) We have many tasks, many tasks to carry out at the same time…hen you leave with that tray, with a whole bunch of medication, and sometimes you end up mixing up patients, mixing up the medication, because it’s a lot to do at the same time (P5).
(Source: Focus Group 2, June 27, 2014)
According to the technicians, the hospital had made some improvements, but several structural aspects still
needed to be reviewed in order lend more precision to the administration phase. he new compartments for the trays used to separate the medications were mentioned as a positive strategy. However, the quality of the com-partments and the size of the trays were still inadequate for patient safety considering the amount of patients and medication administered.
here’s this one patient that has ten little medication cups for just him alone, each one has to be diluted, ea-ch pill in a separate cup (P9).
(Source: Focus Group 1, January 28, 2014)
he trays are too small for such big compartments. So we have to get three trays in order for the compart-ments to it and then we place a whole lot of medi-cation. And three trays don’t it on these carts (P2).
(Source: Focus Group 2, June 27, 2014)
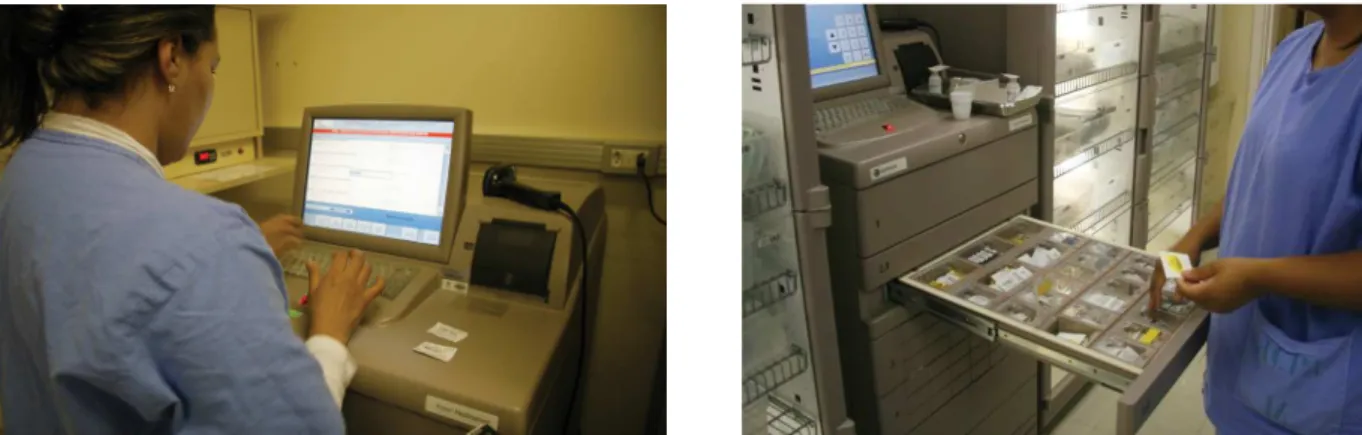
he third category, the use of new technologies to reduce medication errors, contained ideas relative to computerized records on patient medication, in addition to the automated medication dispensing system in the inpatient units. he par-ticipants reported that the introduction of these dispensing systems had improved the safety of the medication process. Such equipment was irst used in one of the researched units. he machines had helped reduce trips to the pharmacy for medication and increased precision when retrieving drugs from the equipment drawers, through the barcode veriica-tion of each medicaveriica-tion prescribed to each patient, including controlled substances such as psychotropic drugs. his system had also made it easier to be aware of drug exclusions, as the prescription reading were always up to date. he following ex-cerpts and Figure 3 illustrate these points:
(...) Even the controlled ones, now we don’t have to do all that distribution, just some dilutions. But the pills too, they are all in the dispensing machine. We count them: if we need to remove a “diazepam”, open the drawer, count how many pills will stay, close it and there you go (P4).
(...) his has really reduced traic to the pharmacy; problems with medications have decreased (P6).
She said that it makes it so much easier, at irst it’s a bit complicated to adapt to, but then it’s the best thing ever. We don’t have to keep fetching medication, we just scan the barcodes and the exact number comes out, correct for each patient (P8).
(Source: Focus Group 1, January 28, 2014)
(...) In this regard, the machine improved things. Be-cause if a drug [prescription] is removed, for example, which the resident [doctor] did not prescribe, it won’t be dispensed (P4).
(Source: Focus Group 2, June 27, 2014)
com-plementary information about the administered drugs and assessing their efectiveness were tools that helped improve patient safety. However, participants also pointed out issues that inluenced nursing work organization and workload.
We spend more time today recording things on the com-puter…you spend more time in front of the computer than with the patient, that’s true. We spend more time prescribing, scheduling and updating charts, you know. It’s recording, recording, recording… (P7).
(…) here’s the machine, there’s the computer sys-tem, the labels (...) and there’s patient care, at the bedside (…) you’re leaving the room and answering the patient’s questions at the same time, because you have to be somewhere else, there’s someone calling you… We have become very bureaucratic and pa-tient care is reduced…there are papa-tients who feel better after a conversation (P8).
(Source: Focus Group, June 27, 2014)
Figure 3 - Withdrawing medication from the automated dispensing machine – Porto Alegre, Rio Grande do Sul, Brazil, 2014. (Source, Photo Walkabout, June 03, 2014)
DISCUSSION
he results of the present study point to the central role and complexity of the medication process in hospital in-patient units. Medication management and administration has become one of the increasingly complex activities in organizing patient care, and are factors that can contribute to increasing demands on the nursing team.
Drug transport, organization, storage, preparation, disposal, and records are part of the nursing professional’s routine, taking up a signiicant portion of the work shift. In each of these phases, there is the chance for medication error to occur.
he perception of the participants in this study converg-es with data from other studiconverg-es that show that 40% of the nursing team’s time in clinical inpatient units is dedicated to the medication administration process, throughout which nurses can administer up to 50 medications. Actions related to medication administration represent an important com-ponent when measuring nursing workload and when deter-mining adequate nursing staf allocation in order to comply with the correct times for administrating patient care. hese studies have shown that more appropriate staf allocation re-sults in lower rates of adverse events(20-22).
he diiculties described in this study in terms of the number of patients, amount of prescribed medication, the need for manual labeling, drug preparation and dilution, in addition to errors in medical prescriptions and diiculties in communication between doctors and the nursing teams were also indicated in other studies, which identiied that
errors in the medication process of hospitalized patients are a consequence of numerous factors(23-24).
When commenting on the workplace dynamics, partici-pants considered that the medication process and its impact on workload, in addition to the high demand of other tasks and caring for a large number of patients had a negative im-pact on the timeliness of the medication schedule. Other risks listed were those related to wrong dose errors and mix-ing up drugs, labels, syrmix-inges or bottles on the medication tray. hese indings corroborate the results of a study that indicated that wrong dose errors (24.3%) and wrong time errors (22.9%) were among the most common types of med-ication errors in a Brazilian university hospital(25).
he nursing staf plays a primary role in the medica-tion process and, more speciically, at the end of the process, when medication is administered to patients. his phase consists of preparing, administrating and determining the efectiveness of the drug regimen and documenting all care activities conducted.
his phase represents the last chance to prevent pre-scription and dispensing errors from afecting patients, in-creasing the responsibility of nursing professionals involved in the process. Furthermore, it is considered more diicult to detect and intercept errors in this phase, as there are few electronic or computerized systems at the patient’s bedside that can help professionals identify errors in the processes that precede medication administration or prevent human error when performing this type of patient care(26-27).
easily detected and intercepted in the initial phases, those of medication prescribing and dispensing, due to the use of electronic and computerized systems that verify medica-tion, including potential drug interactions(27).
Employing new technologies can contribute to increas-ing precision and reducincreas-ing error in medication processes, as illustrated in this study. However, these processes must be closely monitored in order to determine strategies that can diminish their impact on nursing workload and to re-design care processes in order to avoid reducing time for direct patient care activities.
he medication process involves professionals from at least three diferent areas: medical, nursing and pharmacy. Investigating the theme based only on the perspective of the nursing staf was one limitation of this study. Another lim-itation relates to the impossibility of generalizing our results, as they are limited to the characteristics in a speciic context.
CONCLUSION
By means of the ecological restorative approach and the combined use of focus groups and participatory
photo-elicitation methods, participants pointed to the hospital’s medication prescription and dispensing sys-tem and situations of risk in medication administration phase as system vulnerabilities. he central role of the medication process, which acts as an organizing element based on which all other nursing care were aligned was recognized as a factor that increased the demands on the nursing team. Automated dispensing machines, equip-ment that were impleequip-mented to confer greater precision and, consequently, greater safety to the process, were as-sessed favorably by their users. However, this equipment alone cannot eliminate all error from the process.
Due to its interface with other areas involved in the process and especially due to its front-line position in health care delivery, being in direct contact with pa-tients, the nursing team carries great responsibility re-garding medication administration. hese professionals must be supported by the hospital structure and orga-nization in order to ensure patient safety. Furthermore, new studies must be conducted to underline strategies that can help improve the process.
reSUMO
Objetivo: Levantar pontos críticos do processo de medicação, suas repercussões nas demandas de trabalho da equipe de enfermagem e riscos para a segurança dos pacientes. Método: Estudo descritivo, com abordagem qualitativa, na perspectiva ecológico-restaurativa. Os dados foram coletados por meio de grupos focais e fotograias. Participaram enfermeiros e técnicos de enfermagem. Resultados: Três categorias emergiram da análise temática: Desaios nos processos de prescrição e dispensação de medicamentos; Administração de medicamentos – organização no turno de trabalho; Uso de novas tecnologias para diminuir erros de medicamentos. Os resultados apontam que o processo de medicação assume um caráter de centralidade na organização do trabalho da equipe de enfermagem, sendo que estes proissionais coniguram-se como a última barreira para detectar falhas de prescrição e dispensação de medicamentos. Conclusão: Para a identiicação de vulnerabilidades na etapa de administração de medicamentos, o uso de tecnologias, sem dúvida, agrega valor para o processo de cuidado seguro.
DeScritOreS
Carga de Trabalho; Equipe de Enfermagem; Sistemas de Medicação no Hospital; Erros de Medicação; Segurança do Paciente.
reSUMen
Objetivo: Tuvo por objetivo levantar los puntos críticos del proceso de medicación, sus repercusiones en las demandas de trabajo del equipo de enfermería y los riesgos para la seguridad de los pacientes. Método: Estudio descriptivo, con abordaje cualitativa en la perspectiva ecológico restaurativa. Los datos fueron recolectados por medio de grupos focales y fotografías. Han participado enfermeros y técnicos de enfermería. Resultados:Del análisis temática han emergido tres categorías: Desafíos en los procesos de prescripción y despacho de medicamentos; Administración de medicamentos – organización en el turno de trabajo; Uso de nuevas tecnologías para disminuir los errores de medicación. Los resultados apuntan que el proceso de medicación asume un carácter de centralidad en la organización del trabajo del equipo de enfermería, siendo que estos profesionales se coniguran como la última barrera para detectar fallas de prescripción y despacho de medicamentos. Conclusión: Para la identiicación de vulnerabilidades en la etapa de administración de medicamentos, el uso de tecnologías, sin duda, agrega valor para el proceso del cuidado seguro.
DeScriPtOreS
Carga de Trabajo; Grupo de Enfermería; Sistemas de Medicación en Hospital; Errores de Medicación; Seguridad del Paciente.
REFERENCES
1. Kohn LT, Corrigan JM, Donaldson MS; Institute of Medicine, Committee on Quality of Health Care in America. To err is human: building a safer health system. Washington: National Academy Press; 2000.
2. World Health Organization. World alliance for patient safety: forward program 2006-2007 [Internet]. Geneva: WHO; 2007 [cited 2010 Oct 08]. Available from: http://www.who.int/patientsafety/enf
3. Needleman J, Buerhaus P, Pankratz S, Leibson CL, Stevens SR, Harris M. Nurse stafing and inpatient hospital mortality. N Engl J Med.
2011;364(11):1037-45.
4. Aiken LH, Ciomiotti JP, Sloane DM, Smith HL, Flynn L, Neff DF. The effects of nurse stafing and nurse education on patient deaths in
hospitals with different nurse work environments. Med Care. 2011;49(12):1047-53.
5. O’Brien-Pallas L, Li XM, Wang S, Meyer RM, Thomson D. Evaluation of a patient care delivery model: system outcomes in acute cardiac
6. Magalhães AMM, Dall’Agnol CM, Marck PB. Nursing workload and patient safety - a mixed method study with an ecological restorative
approach. Rev Latino Am Enfermagem. 2013;21 (n.spe):146-54.
7. Panunto MR, Guirardello EB. Nursing workload in an intensive care unit of a teaching hospital. Acta Paul Enferm. 2012;25(1):96-101.
8. Leite IRL, Silva GRF, Padilha KG. Nursing Activities Score e demanda de trabalho de enfermagem em terapia intensiva. Acta Paul Enferm.
2012;25(6):837-43.
9. Ball JE, Murrells T, Rafferty AM, Morrow E, Grifiths P. ‘Care left undone’ during nursing shifts: associations with workload and perceived
quality of care. BMJ Qual Saf. 2014;23(2):116-25.
10. D’Amour D, Dubois C, Tchouaket E, Clarke S, Blais R. The occurrence of adverse events potentially attributable to nursing care in medical
units: cross sectional record review. Int J Nurs Stud. 2014;51(6):882-91.
11. Levine S, Cohen MR. Medications errors. Washington: American Pharmacists Association; 2007. Preventing medication errors in pediatric and neonatal patients; p. 469-92.
12. Raduenz AC, Hoffmann P, Radunz V, Dal Sasso GT, Maliska IC, Marck PB. Nursing care and patient safety: visualizing medication
organization, storage and distribution with photographic research methods. Rev Latino Am Enfermagem. 2010;18(6):1045-54.
13. Marck P, Molzahn A, Berry-Hauf R, Hutchings LG, Hughes S. Exploring safety and quality in a hemodialysis environment with a
participatory photographic methods: a restorative approach. Nephrol Nurs J. 2014;41(1):25-35.
14. Gimenes FRE, Marck PB, Atila EG, Cassiani SHB. Engaging nurses to strengthen medication safety: fostering and capturing change with
restorative photographic research methods. Int J Nurs Pract. 2014 Apr 14. [Epub ahead of print]
15. Creswell JW. Projeto de pesquisa: métodos qualitativo, quantitativo e misto. Porto Alegre: Artmed; 2010.
16. Polit DF, Beck CT. Fundamentos de pesquisa em enfermagem: avaliação de evidências para a prática da enfermagem. Porto Alegre: Artmed; 2011.
17. Brasil. Ministério da Saúde; Conselho Nacional de Saúde. Resolução n. 466, de 12 de dezembro de 2012. Dispõe sobre diretrizes e normas regulamentadoras de pesquisas envolvendo seres humanos [Internet]. Brasília; 2012 [citado 2014 out. 11]. Disponível em: http://conselho.saude.gov.br/resolucoes/2012/Reso466.pdf
18. Minayo MCS. O desaio do conhecimento: pesquisa qualitativa em saúde. São Paulo: Hucitec; 2010.
19. Moretti F, Van Vliet L, Bensing J, Deledda G, Mazzi M, Rimondini M, et al. A standardized approach to qualitative content analysis of
focus group discussions from different countries. Patient Educ Couns. 2011;82(3):420-8.
20. Armitage G, Knapman H. Adverse events in drug administration: a literature review. J Nurs Manag. 2003;11(2):130-40.
21. Sears K, O’Brien-Pallas L, Stevens B, Murphy GT. The relationship between the nursing work environment and the occurrence of reports pediatric medication administration errors: a pan Canadian study. J Pediatr Nurs. 2013;28(4):351-6.
22. Gonçalves LA, Andolhe R, Oliveira EM, Barbosa RL, Faro ACME, Gallotti RMD, et al. Nursing allocation and adverse events/incidents in
intensive care units. Rev Esc Enferm USP. 2012;46(n.spe):71-7.
23. Elliott M, Liu Y. The nine rights of medication administration: an overview. Br J Nurs. 2010;19(5):300-5.
24. Paranaguá TTB, Bezerra ALQ, Santos ALM, Silva AEBC. Prevalence and factors associated with incidents related to medication in surgical
patients. Rev Esc Enferm USP. 2014;48(1):41-7.
25. Teixeira TCA, Cassiani SHB. Root cause analysis: evalutaion of medication errors at a university hospital. Rev Esc Enferm USP.
2010;44(1):139-46.
26. Brasil. Ministério da Saúde; Agência Nacional de Vigilância Sanitária. Anexo 03: Protocolo de segurança na prescrição, uso e administração de medicamentos [Internet]. Brasília; 2013 [citado 2015 jan. 24]. Disponível em: http://proqualis.net/sites/proqualis.net/
iles/000002490IQmwD8.pdf