SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Perilunate
carpal
dislocation.
Clinical
evaluation
of
patients
operated
with
reduction
and
percutaneous
fixation
without
capsular-ligament
repair
夽
Adriano
Bastos
Pinho
∗,
Roberto
Luiz
Sobania
UniversidadeFederaldoParaná,Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received27March2016 Accepted28July2016 Availableonline24June2017
Keywords:
Carpalbones/injuries Carpalbones/surgery Fracturefixation,internal Wristinjuries
a
b
s
t
r
a
c
t
Objective:Toqualitativelyassesssurgeriesperformedinpatientswithperilunate disloca-tionswithout associatedfractures,who wereoperatedusing theclosed reductionand percutaneousfixationmethod.Thefollow-uptimerangedfromonetosevenyears. Methods:628patientrecordswithtraumaticwristinjuries,operatedbythesamegroupof HandSurgeonsbetween2008and2014duetoacutetraumawerecollected,withamean follow-upof3.2years.Ofthese,51werecasesofperilunatefracture-dislocations,and38 werepureperilunatedislocationswithoutassociatedfractures;ofthese,only32underwent percutaneousfixationwithoutligamentousrepair,thusmeetingtheinclusioncriteria.Of theninepatientswithperilunatedislocationswhoweretreatedusingtheclosed reduc-tionandpercutaneousfixationmethod,whosemeanagewas38years(range26–49years), thedominantsidewastheleftintwo-thirdsofthecases,andthepredominanttrauma mechanismwasdirecttrauma.
Results:Thisstudy isinagreementwiththeliterature,showingthatcasestreatedearly presentgoodresults.
Conclusion:88%ofpatientswhoweretreatedbyclosedreductionandpercutaneousfixation methodmaintainedtheirdailyactivitiesandwereassessedasexcellentorgoodbythe ClinicalScoringChart.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheUniversidadeFederaldoParaná,HospitaldeClínicasdoParaná,DepartamentodeOrtopediaeTraumatologia, DisciplinadeCirurgiadaMão,Curitiba,PR,Brazil.
∗ Correspondingauthor.
E-mails:[email protected],[email protected](A.B.Pinho). http://dx.doi.org/10.1016/j.rboe.2017.06.007
Luxac¸ão
perilunar
do
carpo.
Avaliac¸ão
clínica
de
casos
operados
com
reduc¸ão
e
fixac¸ão
percutânea,
sem
reparo
cápsulo-ligamentar
Palavras-chave: Ossodocarpo/lesões Ossodocarpo/cirurgia Fixac¸ãointernadefraturas Traumatismosdopunho
r
e
s
u
m
o
Objetivo: Fazerumaavaliac¸ãoqualitativadascirurgiasfeitasempacientesquesofreram luxac¸ões perilunares, sem fraturas associadas, que foramoperados como método de reduc¸ãoincruentaefixac¸ãopercutânea.Otempodeseguimentovariouentreumesete anos.
Métodos: Foramlevantadosprontuáriosde628pacientes,sobadenominac¸ãodelesões traumáticasnopunho,operadospelomesmogrupodecirurgiõesdemão,entre2008a2014, comseguimentomédiode3,2anos,devidoatraumasagudos.Desses,51foramcasosde fraturas-luxac¸õesperilunares,38eramluxac¸õesperilunarespuras,semfraturasassociadas; dessas,apenas32tiveramfixac¸ãopercutânea,semreparoligamentar,contemplaramassim osrequisitosdapesquisa.Dosnovepacientescomluxac¸õesperilunaresqueforamtratados pelométododereduc¸ãofechadaefixac¸ãopercutânea,commédiade38anos(26a49),o ladodominantefoioesquerdoem2/3doscasos,omecanismodetraumapredominantefoi odireto.
Resultados: Esteestudoconvergiucomoutrostrabalhosnaliteratura,mostrouqueoscasos tratadosprecocementeapresentambonsresultados.
Conclusão: Mantiveramsuasatividadesdevidadiáriaeforamavaliadoscomoexcelentes oubonspeloClinicalScoringChart88%dospacientesqueforamtratadospelométodode reduc¸ãofechadaefixac¸ãopercutânea.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Carpalinstabilitystillchallengesspecialists,notonlybecause thereareaspectsofitspathophysiologythatstillneedtobe clarified,but alsobecausewhennotproperly treated, such problemscanhavesubstantialadversesocialconsequences intermsofdisability.1
Thekinematics of carpal bones are complex, and their movementsarepredominantlyguidedbythecontactofbones andbytheactionofligamentsandjointsratherthanthedirect actionofmuscularforces.Therefore,itisdifficulttopredictthe movementofcarpalbonesafterligamentlesionswithimaging studiesandclinicaltestsalone.2
Thewristisacomplexstructure,composedofbones, liga-ments,andtendonsthattogetherandharmoniouslyallows movements in the coronal and sagittal planes. Due to its positioninganditsmovementarc,thewristissusceptibleto constantaxialforcesanddeformationvectors.3
Carpal stability is defined as the ability ofthe wrist to maintainstaticanddynamicbalanceofthejointsunder phys-iologicalloadsandmovements.Inturn,carpalinstabilityis thedisturbanceofthatbalanceassociatedwithboneand/or ligamentinjuries,resultinginfailuretomaintainthe articu-laranatomicalrelationshipsandresultinginbiomechanical performancedeficit,pain,andcarpalcollapse.3
Itisbelievedthatcarpalinstabilityismorecommonthan previouslythoughtandthatdegenerativediseaseistheend resultofundiagnosedinstability.2
Perilunate dislocations are uncommon and serious injuries;61%–65%ofthecasesareassociatedwithscaphoid
fractures, referred to as “major arch injuries;” these are outsidethescopeofthisarticle,whichaddressesonlypure ligamentinjuries(“minorarchinjuries”).4
The scapholunate (SL) and lunotriquetal (LT) ligaments arethemostimportant,responsibleforstabilizingthe prox-imal row. Theyfixatethe proximalmargin ofthe scaphoid to the lunate, and the proximal lunate to the pyramidal, respectively.3
Previousstudieshaveinvestigatedthedynamicandstatic aspectsofscapholunateinstability(definedasaradiographic increaseinspacebetweenthescaphoidandthelunate)and theconsequencesforthewrist.2
Perilunatedislocationsofthecarpusarerarelesions,which may go unnoticed in 15%–50% of cases, generally result-ingfromshockorhigh-energytrauma.Theyareresponsible for severe osteochondral and capsuloligamentous lesions, whichmayleaveimportantfunctionalsequelae,dominated by chronic instability of the wrist and, in the long term, osteoarthritis.5
Perilunatedislocationsarerelativelyuncommon.Theyare seriouscarpallesionsthatoccurafterhigh-energytraumaor whenthevictimfallsontheoutstretchedhand.Theyproduce avariableinterruptionofcarpalanatomy,butitsconstantand definingcharacteristicisadislocationoftheheadofthe capi-tate,distaltothesurfaceofthelunate,mostoftendorsaland sometimesvolar.Theseareaformofprogressiveligamentand bonedamage.6
Mayfielddescribedfourstagesofpureligamentinjuries7:
- I:scapholunateinjuryordissociation
- II:ruptureordisplacementbetweenthelunateandthe cap-itate
- III:lunotriquetralinjuryordislocation
- IV:severeradiolunateinjurywithlunateenucleationand riskofnecrosis
Injurymechanisminvolvesabruptwristextension, asso-ciatedwithulnardeviationandsupinationoftheintercarpal joint.ThemostseriousoftheseinjuriesareMayfieldtypesIII andIV,whichresultfromhigh-energytrauma.8
Anatomicreductionofintercarpalrelationshipsisthekey toavoidingavascularnecrosisorcarpalinstabilityand, ulti-mately,chronicscapholunateadvancedcollapse(SLAC)and osteoarthritis.8
In addition, while spontaneous reductionsare possible, theymayunderestimatetheseverityofinjuryandligament damage.6
Three types of treatment have been described: closed reductionandcastimmobilization;closedreductionand per-cutaneousfixation,associatedwithimmobilization;and,open ligament and bone repair with fixation and postoperative immobilization. Currently, the results ofclosed reductions without fixation are unsatisfactory and do not allow the reestablishment ofthe capsuloligamentous apparatus and, therefore,carpalstability.5
Thecurrent“goldstandard”treatmentoftheselesionsis reduction,fixation,andreconstruction(mainlyofthe scaphol-unateligament),butitisobservedinclinicalpracticethatin manyofthecasesinwhichthegoldstandardisnotperformed, reconstructionsorprimarysutureoftheintercarpalligaments progresswell,andpatientsremainwithoutsignificant com-plaintsforlongperiodsoftime.
Although the literature presents great variation in the resultsofperilunatecarpaldislocations,long-termexperience andprognosisare notnecessarilysatisfactory. Wrist move-mentisimpaired,and arthrosisofthemediocarpaljoint is common.9
Astudydemonstrated thatthereflexesoriginatingfrom themusculoskeletalsystem,whichinvolvesthewrist,playa roleinprotectingthejoint andpreventingexcessive excur-sionofthe carpal bones, havinga protectiveeffect onthe developmentofpost-traumaticosteoarthritis.10
Theresultsofsurgicaltreatmentforperilunatedislocations andfractures-dislocationsremainedbelowidealinpatients whoweretreatedwithinfourweeksofinjuryusingsimilar reductionandfixationprinciplesinaspecializedcenter.11
Mediannervelesionsmaybepresentatthetimeofinitial careduetocompressionofthenerve;itusuallyregressesafter reduction.Theliteraturereportspersistenceofsymptomsup tosixmonthsafterthereduction.12
Astudyonfracturesofthedistalendoftheradius,focusing oncarpalinstabilities,demonstratedthatcarpalinstabilities duetomisalignmentoftheradial-lunate-capitateaxisshould becorrected,asinthelongtermtheywillberesponsiblefor degenerativewristalterations.13
Somefactorsthataffectprognosisarestillbeingdiscussed; thisstudyaimedtocollectqualitativedata,bothclinicaland
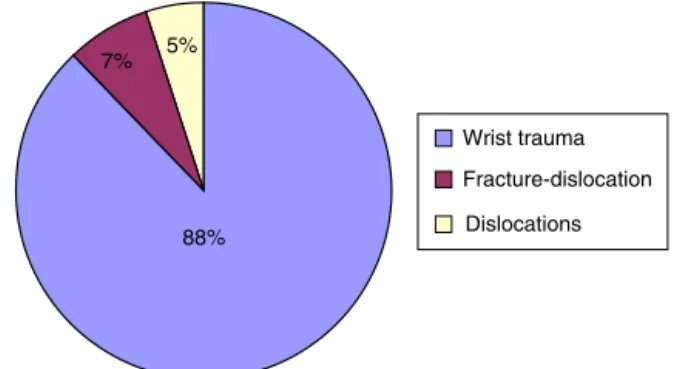
Wrist trauma
Fracture-dislocation
Dislocations 88%
7% 5%
Fig.1–Totalpercentageofmedicalrecords,accordingto pathologies.
radiographic,inordertoassesstheoutcomeofpatientswho wereoperatedforperilunatelesionsofthecarpususingclosed reductionandpercutaneousfixation.
Patients
and
methods
Atotalof628medicalrecordsofpatientsdiagnosedwith trau-maticwristinjuriesduetoacutetrauma,operatedbythesame groupofhandsurgeonsbetween2008and2014,witha follow-upbetweenoneandsevenyearswereselected.Ofthese,51 werecasesofperilunatefracture-dislocations;38werepure perilunatedislocations,withoutassociatedfractures,andof these,only32hadbeentreatedwithpercutaneousfixation, withoutligamentrepair,meetinginclusioncriteria(Fig.1).
The 628 records were divided into three groups: wrist trauma (distal radius fractures, physeal injuries, and car-pometacarpal lesions), fracture-dislocations (trans styloid perilunatefractures,transcaphoid-perilunateand transcap-itate fractures, or combinations of these); and perilunate dislocationsorminorcarpalarchinjury.
Of the 38 patients withperilunate dislocations without associatedfracture,thosewhounderwentsurgeryafterover sevendaysofinjuryorwhounderwentcapsuloligamentrepair orreconstruction(includingthescapholunateligament)and patientsunder18yearsofageattimeofinjurywereexcluded fromthestudy;32casesremained.
Therewassomedifficultyinlocatingpatients,sincethe telephonenumberregisteredinthemedicalrecordswasno longervalidinmanycases.Inothercases,evenwhencontact wasachieved,manyreportedthattheywerewellandthusdid notcooperate,becauseparticipationinthestudyrequireda returntotheclinic.Insomecasestherewaslosstofollow-up, changeofaddress,orrefusaltocollaboratewiththeresearch. Thus,thisstudyincludedninepatients.
Methods
Theselectedpatientswerethosesubmittedtoclosed reduc-tion and percutaneous fixation between the scaphoid and thelunate,scaphoidandcapitate,pyramidalandlunate,and betweentheradiusandlunate,withsomevariations,aswillbe shown.MeantimeforK-wiresremovalwas10weeks,aswas alsodemonstratedinotherstudies,2,9,14butK-wiresbetween
Fig.2–Saehandynamometer,usedintheresearch.
Forallpatients,clinicalandradiographicevaluationwas madeusingtheClinicalScoringChart,6andepidemiological
profilewasassessed(age,sex,occupation,associatedtrauma); thestudywasapprovedbytheEthicsCommittee(No.999,765), CAAE:43106315800005225,andpatientssignedaninformed consentform.
The Jamar dynamometer is an instrument for manual grip strength validation, having been the most accepted instrument since1954,and is recommended bythe Amer-ican Society of Hand Therapists (ASHT) to measure grip strength in patients with various disorders that compro-mise theupperlimbs. Onearticleshowed the validityand
Fig.4–Gilula’sarcs.15
reliabilityoftheSaehandynamometer,basedoncomparative andforcetestsbetweentheJamarandSaehanmodels.The Saehandynamometerwasusedinthepresentstudy(Fig.2).14
Patients were evaluated ina seated position,with their armsrestingontheirthighs,asrecommendedbytheASHT. Threegripstrengthmeasurementsweremadeoneachside, alternatingsides;patientswereinstructedtoperform maxi-malcontractionforthreesecondsandat30-secondintervals betweeneachtest(Fig.3).Meanvaluesofthethreetests,for eachhand,wereusedfordataanalysis.14
Theradiographicassessmentincludedwascomposedby theanalysisofGilula’sarcs(Fig.4),posteroanterior(PA) radio-graphs,andthescapholunateangle,measuredthroughprofile radiography.
OnthePAradiographs,thefollowingcanbeobserved: ArcI –articularsurfaceproximaltothe firstrow ofthe carpus;
ArcII–articularsurfacedistaltothefirstrowofthecarpus;
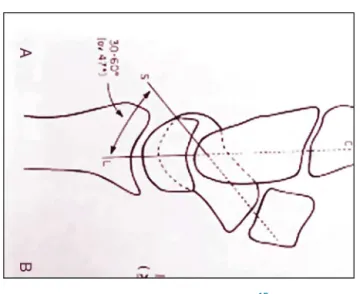
Fig.5–Schematicdrawing.15
ArcIII–articularsurfaceproximaltothesecondrowofthe carpus.15
Thescapholunateangleismeasuredattheprofile radio-graphs,andisconsiderednormalwhenbetween30◦and60◦.
Fig. 5 shows a representation of how the scapholunate anglewasevaluatedinprofileradiographs.
Currentradiographicassessment
• MaintenanceofGilula’sarcs.
• Scapholunateangle,indegrees(profileradiograph). • Scapholunateinterval:lessthanorequalto3mmorlarger
than3mm(comparativeradiographswiththecontralateral side).
Evaluationparametersofcarpalperilunatedislocations:
ClinicalScoringChart6
Pain:
- Nopain...25points.
- Occasionalpain...20points.
- Severepain...10points.
- Constantpain...0point.
ROM:sumofthedegreesofwristflexionandextension.
- Greaterthan140◦...25points.
- Between100◦and140◦...20points.
- Between70◦and99◦...15points.
- Between40◦and69◦...10points.
- Lessthan40◦...0points.
Grip strength: assessed through a dynamometer (the healthysidewasusedasareference).
- Normal...25points. - Decreased,but greater than50% fromnormal...15
points.
- Lessthan50%ofnormal...0points.
Table1–Firstpartofpatientoutcomes.
Demographics
Patient Sex Month/year Trauma
mechanism
1 M Nov/13 Crushing
2 M Jul/13 Directtrauma
3 M Oct/13 Directtrauma
4 M Sept/13 Directtrauma
5 M May/13 Directtrauma
6 M Jun/14 Directtrauma
7 M Sept/12 Directtrauma
8 M Feb/12 Directtrauma
9 M Apr/08 Directtrauma
Activity
- Performed the same activities... 25 points.
- Restrictedactivitiesduetoinjury...15points. - Changeofworkorsportduetoinjury...0points.
Finalscoreofthepatient:thesumoftheprevious ques-tions.
- Excellent:greaterthanorequalto95points. - Good:greaterthanorequalto75points. - Regular:greaterthanorequalto60points. - Poor:lessthan60points.
Clinical and radiographic evaluations were performed comparatively.Thecontralateralside,normalandinjury-free, wasusedasaparameterofnormalityforeachpatient.
After completion of the Clinical Scoring Chart,6 each
patient’s result was classified according to the criteria describedabove(excellent,good,fair,orpoor).
Fig.6showsaradiographofacaseofperilunatedislocation orminorarchinjury.
Fig. 7shows an example ofa patient’s radiographafter closedreductionandpercutaneousfixation.Inthiscase,the scaphoid was fixated percutaneously with the lunate, the scaphoidwiththecapitate,thepyramidalwiththelunate,and thepyramidalwiththecapitate.
Results
Allninepatientsevaluatedweremale,withameanageof38 years(26–49)andameanfollow-upof3.2years(1.5–7years); leftsidewasthedominantsideintwo-thirdsofthecases,and directtraumawasthepredominantmechanismoftrauma.
Gilula’sarcsweremaintainedintheradiographic evalua-tionof88%ofpatients(Table1).
Themean scapholunate anglewas 54◦ (35◦–70◦); 67%of
caseswerewithinnormallimits.
Fig.6–Radiographofacaseofcarpalperilunatedislocation.
Fig.7–Radiographofacasetreatedbyclosedreductionandpercutaneousfixation.
Ofthepatientsevaluated,fourcontinuedtopractice physi-calactivitieswithminoradaptationsorlimitations(44%ofthe total).
TheresultoftheScoreChartshowedthat88%ofpatients presentedgoodorexcellentresults,andonlyonepatient pre-sentedpooroutcome(Table2).
Fig. 8 shows the radiograph of a case of perilunate dislocation of the carpus, treated by closed reduc-tion and percutaneous fixation, seven years after injury.
Table2–Secondpartofpatientoutcomes.
Searchresults Radiographicandclinicalresults
Patient SLinterval SLangle ScoreChartresults RemovaloftheKW,weeks Fixatedjoints MaintenanceofGilula’sarc
1 Greaterthan3mm 50◦ Poor 8w RL/SL Yes
2 Greaterthan3mm 50◦ Excellent 8w RL/SL/SC Yes
3 Greaterthan3mm 50◦ Excellent 10w SL/PL Yes
4 Greaterthan3mm 70◦ Excellent 10w RL/SL/SC Yes
5 Greaterthan3mm 56◦ Good 8w RL/SL/SC Yes
6 Lessthan3mm 70◦ Good 10w RL/SL/SC/PL No
7 Greaterthan3mm 40◦ Good 10w RL/SL/SC/PL Yes
8 Greaterthan3mm 35◦ Excellent 12w RL/SL/SC/PL Yes
9 Lessthan3mm 67◦ Good 10w SL/SC/PL Yes
SC,fixationbetweenthescaphoidandcapitate;SL,fixationbetweenscaphoidandlunate;KW,Kirschnerwire;PL,fixationbetweenpyramidal andlunate;RL,fixationofthejointbetweentheradio-lunate;w,weeks.
Fig.8–Radiographaftersevenyearsofinjury.
45%
Excellent
Good
Fair
Poor 11%
44%
Fig.9–AssessedpatientsandresultsofClinicalScoring Chart.
Discussion
Main problemofcarpal ligament injuriesistheir potential to develop arthritis over time7; perilunate dislocations are
complexand,duetotheirinherentinstability,aresurgically treated.1
Clinicalpracticesometimesshowsadivergencebetween clinicalstatusofthepatient’swristanditsradiographic eval-uation,sothistypeofstudyhasbecomeimportant.
Despitethesmallnumberofpatientsevaluated,thisstudy aimedtoqualitativelyevaluatecasesoperatedduetocarpal perilunatedislocationstreatedacutely,inuptosevendays, bythesameteamofsurgeons.Patients,withamean follow-upof3.2years(1.5–7),underwentnon-invasivereductionand percutaneousfixationwithoutrepairofthescapholunate liga-ment,witha10-weekmeanintervaluntilremovalofK-wires. Theliteratureindicatesasimilarintervalforremovalofthe K-wires,rangingfrom8to12weeks.1,6,9
Regardingdemographic characteristics,therewasa pre-dominanceofphysicallyactiveyoungmenandlesionsdue tohigh-energytrauma(mostofwhichweremotorcycle acci-dents).In77%ofthepatients,theradiuswasfixatedtothe lunate,whichisalsosuggestedbysomestudiesasawayof avoidinglossofreduction.7
MaintenanceofGilula’sarcswasobservedin88%ofthe casesinthepresentstudy,andthescapholunateanglein lat-eralview was withinthe normalrange (30◦–60◦) in67% of
cases.15
Of the nine patients evaluated, four practiced physical activity(twoare inthe military,oneisanamateurathlete, andoneisamartialartsteacher).Theycontinuedtoperform theirexerciseactivities,withminorchangesoradaptations.
Onlyonepatienthadapoorscore,havingtodiscontinue hisphysicalactivities(motocross)infavoroflighteractivities, duetowristROMlimitations.
Conclusion
Resultsofthepresentstudyareinagreementwiththe litera-ture,showingthatcasestreatedearlyhavegoodresults.6
Thestudydemonstrated that88% ofpatientswho were treatedbyclosedreductionandpercutaneousfixationwere abletomaintaintheirdailyactivitiesand wereassessedas excellentorgoodbytheClinicalScoringChart.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
ToDr.LucianoDrigoPeresandtotheoccupationaltherapist DéboraMachadofortheirsupportandencouragement.
r
e
f
e
r
e
n
c
e
s
1.WolfeSW,PedersonWC,HotchkissRN,KozinSH.Green’s operativehandsurgery.6thed.Philadelphia:Churchill Livingstone;2010.
2.PattersonRM,YazakiN,AndersenCR,ViegasSF.Predictionof ligamentlengthandcarpaldiastasisduringwrist
flexion-extensionandaftersimulatedscapholunate instability.JHandSurgAm.2013;38(3):509–18.
3.SugawaraLM,YanaguizawaM,IkawaMH,TakahashiRD, NatourJ,FernandesARC.Instabilidadedocarpo.RevBras Reumatol.2008;48(1):34–8.
4.BudoffJE.Treatmentofacutelunateandperilunate dislocations.JHandSurgAm.2008;33(8):1424–32. 5.ElouakiliI,OuchrifY,NajibA,OuakrimR,LamraniO,
KharmazM,etal.Anexceptionalformofperilunarcarpal dislocation.PanAfrMedJ.2014;18:108.
6.HerzbergG,ComtetJJ,LinscheidRL,AmadioPC,CooneyWP, StalderJ.Perilunatedislocationsandfracture-dislocations:a multicenterstudy.JHandSurgAm.1993;18(5):768–79. 7.ChantelotC.Post-traumaticcarpalinstability.Orthop
TraumatolSurgRes.2014;1001Suppl.:S45–53.
8.SotereanosDG,MitsionisGJ,GiannakopoulosPN,Tomaino MM,HerndonJH.Perilunatedislocationandfracture dislocation:acriticalanalysisofthevolar–dorsalapproach.J HandSurgAm.1997;22(1):49–56.
9.VitaleMA,SeetharamanM,RuchelsmanDE.Perilunate dislocations.JHandSurgAm.2015;40(2):358–62. 10.Salva-CollG,Garcia-EliasM,HagertE.Scapholunate
instability:proprioceptionandneuromuscularcontrol.JWrist Surg.2013;2(2):136–40.
11.HildebrandKA,RossDC,PattersonSD,RothJH,MacDermid JC,KingGJ.Dorsalperilunatedislocationsand
fracture-dislocations:questionnaire,clinical,and
radiographicevaluation.JHandSurgAm.2000;25(6):1069–79. 12.GreenDP,O’BrienET.Openreductionofcarpaldislocations:
indicationsandoperativetechniques.JHandSurgAm. 1978;3(3):250–65.
13.BarbieriCH,MazerN,SantiagoGR.Avaliac¸ãotardiade fraturasdaextremidadedistaldorádio,comparticular atenc¸ãoparaasinstabilidadescarpaisassociadas.RevBras Ortop.1994;29(8):591–6.
14.ReisMM[dissertac¸ão]Estudodavalidadeeconfiabilidade, entreosdinamômetrosSaehaneJamar.SãoJosédos Campos:UniversidadedoValedoParaíba,Institutode PesquisaeDesenvolvimento;2009.