PREVALENCE OF VESTIBULOPATHY IN INSTITUTIONALIZED
ELDERLY PERSONS IN NATAL-RN-BRAZIL
Prevalência de vestibulopatia em idosos institucionalizados
de Natal - RN - Brasil
Lidiane Maria de Brito Macedo Ferreira(1),
Karyna Myrelly Oliveira Bezerra de Figueiredo Ribeiro (1), Kenio Costa de Lima(1)
(1) Universidade Federal do Rio Grande do Norte (UFRN), Natal, RN, Brasil.
Conlict of interest: non-existent
otoneurological symptoms, such as hearing loss, tinnitus and aural fullness, may also occur3,4.
Vestibular dysfunction is a major cause of dizziness in the elderly 5. It represents 40-50% of
cases involving elderly persons referred to otolaryn
-gologists. It is also an important diferential diagnosis when an elderly person sufers unexplained falls6,7.
The main type of vestibulopathy among elderly persons is benign paroxysmal positional vertigo (BPPV), which represents 40% of vestibular disorders in elderly persons aged over 707-9.
Vestibular neuronitis, labyrinthitis, Meniere’s disease and brain disorders are also common6.
The diagnosis of vestibular disease is based on clinical history, disease history, medication use and detailed physical examination5. Records conirm that
medical history, evaluation for nystagmus and the Dix-Hallpike Test10 are the most important tools for
the diagnosis of dizziness, especially of vestibular origin, during primary assessment8. Such tests
allow the screening of patients who require more INTRODUCTION
Body balance depends on the proper functioning of three systems, which act synergistically: vision, proprioceptive sensitivity and the vestibular apparatus. The latter consists of the labyrinth, pathways and vestibular nuclei, which interrelate in the region of the brain stem with other nuclei and neuronal pathways1,2. Changes in body balance
may result from dysfunction at any of these levels, whether related to vestibular disorders or not. When the dysfunction occurs in the vestibular system, this is known as vestibulopathy.
The main symptom of vestibulopathy is vertigo, which usually lasts from seconds to minutes, but can also last for hours or days, and is associated in most cases with neurovegetative symptoms. Other
ABSTRACT
Purpose: to assess the prevalence of vestibulopathy and associated factors in institutionalized elderly
persons through bedside clinical examination. Methods: a cross-sectional study was performed in 12
homes for aged in Natal, Brazil, regulated by the Health Surveillance Department. Elderly persons who possessed a good cognitive level and were able to walk were selected, resulting in a total sample of 115 persons. They were asked whether they had experienced dizziness in the past year, and when the answer was positive, responded to a questionnaire and underwent physical examinations for the diagnosis of vestibulopathy, in accordance with the protocol established by Johnson and Lalwani (2004). The Chi-squared or Fisher’s Exact tests were used for statistical analysis, with a signiicance level of 5%, and the Prevalence Ratio was calculated. Results: the prevalence of vestibulopathy
was 10.56%, and the condition was associated with osteoarthritis and alcohol consumption.
Conclusion: there is a low prevalence of vestibulopathy among institutionalized elderly persons in
Natal, Brazil.
the help of another person or equipment such as a walker or cane were included. Elderly persons with communication problems (for example, those who were deaf or did not speak Portuguese), as well as those with serious memory problems were also excluded. These individuals were identiied during the application of the questionnaire, in which some questions were repeated at diferent times to allow the interviewer to ascertain the attention and memory levels of the elderly person. In the event of inconsistency in the answers, the elderly person was excluded from the study. In the same way, elderly persons who were unable to complete all the physical tests were excluded. A total of 123 elderly persons met the inclusion criteria, and of these, eight refused to participate in at least one stage of the study, giving a total of 115 subjects
To identify vestibulopathy, a questionnaire of neurotological history, initially with the question about the presence of dizziness in the last year was applied. If the answer was airmative, a further questionnaire was subsequently applied, which consisted of questions regarding type of dizziness, classiied in accordance with Drachman and Hart
(1972) 17 as vertigo, presyncope, imbalance and
psychogenic (or atypical) dizziness; the duration of the dizziness; the presence of hearing loss, tinnitus, aural fullness, neurovegetative symptoms, decreased visual acuity, and the use of a hearing aid, glasses or a cane. Other questions referred to general data regarding the facility, the health of the patient and his or her general life habits. This data was collected directly from the medical records of the patients.
Of the initial 115 elderly persons, only 51 complained of at least one bout of dizziness in the inal year.
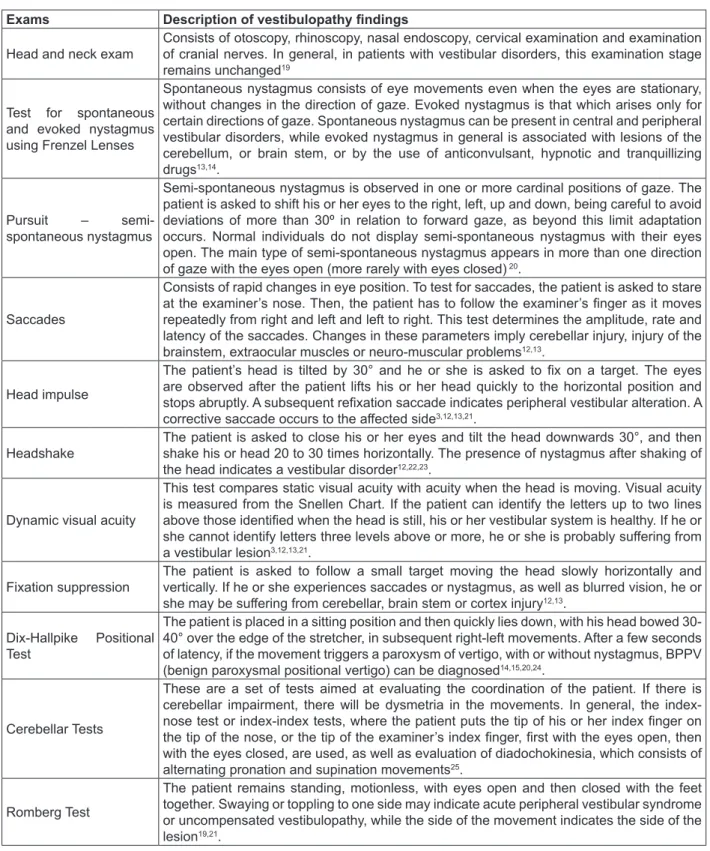
The physical diagnostic exam for vestibu
-lopathy of these 51 elderly persons was therefore performed, in accordance with the procedures proposed by Johnson and Lalwani18. This consists
of 11 physical examination tests of the patient with suspected vestibulopathy (Figure 1). In the event that a disorder was identiied in one of the tests, a inding suggestive of vestibular injury, the patient was diagnosed as having vestibulopathy.
extensive examination or assessment at secondary and tertiary care levels.
Clinical examination1,11, as the initial clinical
evaluation of a patient is known, can also be used to distinguish peripheral or central vestibular problems, the degree of injury and whether the condition of the patient is acute or chronic10,12-15.
There are several tests included in this assessment which, depending on the author in question, vary in number and type. All, however, propose a battery of tests through physical examination only, without additional diagnostic tests2,16. This deinition is
useful for epidemiological evaluation, as minimal resources are necessary for the diagnosis of the maximum possible number of patients. This type of diagnosis uses simple equipment and can be performed quickly.
The aim of this study was to assess the preva
-lence of vestibulopathy and associated factors in institutionalized elderly persons by clinical bedside examination.
METHODS
The study complied with the criteria and require
-ments established by Resolution No. 466/12 of the National Health Council (CNS) and followed the recommendations of the Federal University of Rio Grande do Norte (UFRN) Research Ethics Committee (CEP), and was approved under protocol number 309/2012. All the elderly persons voluntarily agreed to participate and signed Letters of Free and Informed Consent.
A population-based cross-sectional study was performed of elderly residents of both private and non-proit Nursing Homes, registered by the Health Surveillance Department, in the city of Natal, Brazil. The municipality has 12 Nursing Homes, six of which are private and six of which are nonproit, which resulted in a total of 386 elderly persons.
Exams Description of vestibulopathy indings
Head and neck exam Consists of otoscopy, rhinoscopy, nasal endoscopy, cervical examination and examination of cranial nerves. In general, in patients with vestibular disorders, this examination stage remains unchanged19
Test for spontaneous and evoked nystagmus using Frenzel Lenses
Spontaneous nystagmus consists of eye movements even when the eyes are stationary, without changes in the direction of gaze. Evoked nystagmus is that which arises only for certain directions of gaze. Spontaneous nystagmus can be present in central and peripheral vestibular disorders, while evoked nystagmus in general is associated with lesions of the cerebellum, or brain stem, or by the use of anticonvulsant, hypnotic and tranquillizing
drugs13,14.
Pursuit – semi-spontaneous nystagmus
Semi-spontaneous nystagmus is observed in one or more cardinal positions of gaze. The patient is asked to shift his or her eyes to the right, left, up and down, being careful to avoid deviations of more than 30º in relation to forward gaze, as beyond this limit adaptation occurs. Normal individuals do not display semi-spontaneous nystagmus with their eyes open. The main type of semi-spontaneous nystagmus appears in more than one direction of gaze with the eyes open (more rarely with eyes closed) 20.
Saccades
Consists of rapid changes in eye position. To test for saccades, the patient is asked to stare at the examiner’s nose. Then, the patient has to follow the examiner’s inger as it moves repeatedly from right and left and left to right. This test determines the amplitude, rate and latency of the saccades. Changes in these parameters imply cerebellar injury, injury of the brainstem, extraocular muscles or neuro-muscular problems12,13.
Head impulse
The patient’s head is tilted by 30° and he or she is asked to ix on a target. The eyes are observed after the patient lifts his or her head quickly to the horizontal position and stops abruptly. A subsequent reixation saccade indicates peripheral vestibular alteration. A corrective saccade occurs to the afected side3,12,13,21.
Headshake The patient is asked to close his or her eyes and tilt the head downwards 30°, and then shake his or head 20 to 30 times horizontally. The presence of nystagmus after shaking of the head indicates a vestibular disorder12,22,23.
Dynamic visual acuity
This test compares static visual acuity with acuity when the head is moving. Visual acuity is measured from the Snellen Chart. If the patient can identify the letters up to two lines above those identiied when the head is still, his or her vestibular system is healthy. If he or she cannot identify letters three levels above or more, he or she is probably sufering from
a vestibular lesion3,12,13,21.
Fixation suppression The patient is asked to follow a small target moving the head slowly horizontally and vertically. If he or she experiences saccades or nystagmus, as well as blurred vision, he or she may be sufering from cerebellar, brain stem or cortex injury12,13.
Dix-Hallpike Positional
Test
The patient is placed in a sitting position and then quickly lies down, with his head bowed 30-40° over the edge of the stretcher, in subsequent right-left movements. After a few seconds of latency, if the movement triggers a paroxysm of vertigo, with or without nystagmus, BPPV (benign paroxysmal positional vertigo) can be diagnosed14,15,20,24.
Cerebellar Tests
These are a set of tests aimed at evaluating the coordination of the patient. If there is cerebellar impairment, there will be dysmetria in the movements. In general, the index-nose test or index-index tests, where the patient puts the tip of his or her index inger on the tip of the nose, or the tip of the examiner’s index inger, irst with the eyes open, then with the eyes closed, are used, as well as evaluation of diadochokinesia, which consists of alternating pronation and supination movements25.
Romberg Test
The patient remains standing, motionless, with eyes open and then closed with the feet together. Swaying or toppling to one side may indicate acute peripheral vestibular syndrome or uncompensated vestibulopathy, while the side of the movement indicates the side of the
lesion19,21.
identiied by the Snellen Chart screening exam, with detection of visual acuity lower than 0.1. In these cases the disorders identiied were due to deiciency in the visual, rather than the vestibular, system. As there was no other alteration in the vestibular test, the hypothesis of an injury associated with both systems was excluded. These persons, in spite of testing positive in some aspects of the physical examination, were not considered to have vestibulopathy.
According to these criteria, 13 elderly persons had an epidemiological diagnosis of vestibulopathy, representing a prevalence of 10.56%.
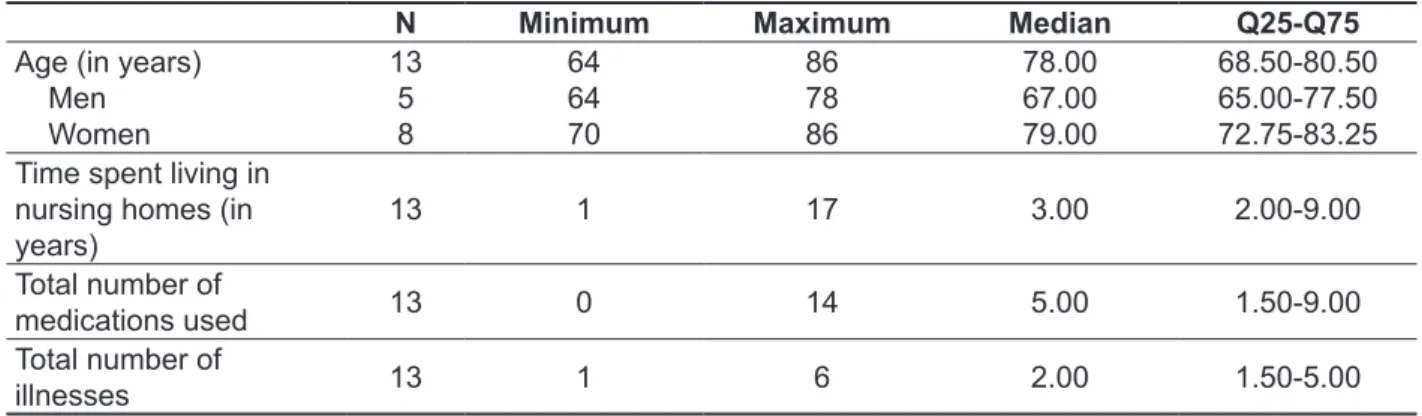
Of the thirteen patients with vestibulopathy, the majority were female (61.5%) and were considered to be very old, or in other words, older than 75 years, with female patients more than a decade older than male patients. With respect to the characteristics of the institution, 76.9% of the patients were residents of non-proit nursing homes and the median length of time for which they had lived at the residence was short. The elderly persons had few associated pathologies and were treated using a polypharmacy program (Table 1).
For the evaluation of visual acuity in the elderly, a screening test was performed with a Snellen Chart26
positioned ive meters from the individual, with normal vision identiied as being able to read the 20/20 line with both eyes, corresponding to a visual acuity of 0.8. The test was performed with correction for those elderly persons who used glasses
After data was collected, descriptive analysis was performed to identify the elderly persons with vestibulopathy, as well as bivariate analysis using the Chi-squared or Fisher’s Exact tests for a signii
-cance level of 5%. The Prevalence Ratio (PR) was calculated and the conidence interval was 95%.
RESULTS
Elderly persons who complained of dizziness in the last year underwent physical examination for the diagnosis of vestibulopathy. Among those where disorders were detected, an epidemio
-logical diagnosis of vestibulopathy was conirmed. Exceptions were made for those elderly persons who only displayed disorders in ocular-motor tests, but who had greatly reduced bilateral visual acuity,
Table 1 – Median, quartiles, minimum and maximum age, length of time spent living in Nursing homes, total number of medications and total number of pathologies presented by all elderly patients with
dizziness from Nursing homes in Natal. Natal-Brazil, 2013.
N Minimum Maximum Median Q25-Q75
Age (in years) Men Women
13 5 8
64 64 70
86 78 86
78.00 67.00 79.00
68.50-80.50 65.00-77.50 72.75-83.25
Time spent living in nursing homes (in
years) 13 1 17 3.00 2.00-9.00
Total number of
medications used 13 0 14 5.00 1.50-9.00
Total number of
illnesses 13 1 6 2.00 1.50-5.00
The results of the physical exam conirming the presence of vestibulopathy are described in Figure
2.
Of these disorders, ten patients had Peripheral Vestibular Syndrome (76.92%) and three were diagnosed with Mixed Vestibular Syndrome (23.07%). The disorders that suggested the elderly persons had sufered a central lesion with mixed disorders were identiied by the Romberg Test, where there was backward toppling, the presence of visual acuity in the ixation suppression test, and the presence of miosis with dizziness in the Dix-Hallpike
Test in a patient with migraines. A diagnosis of BPPV (benign paroxysmal positional vertigo), identiied through positivity in the Dix-Hallpike Test, was found for eight patients, representing a prevalence of 61.53%.
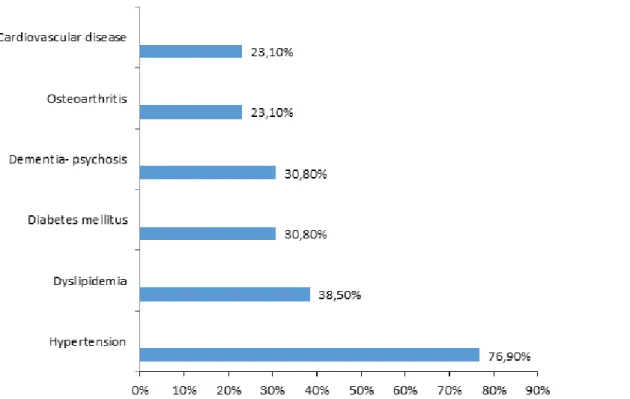
egarding the distribution of the diseases which elderly persons with vestibulopathy sufered from, it was observed that most had Systemic Arterial Hypertension, according to information collected from medical records, all with the use of antihyper
The main characteristics of dizziness among elderly persons with vestibulopathy were as follows. Imbalance was the most common type of dizziness, generally lasting seconds, and the majority of persons did not have associated neurovegetative symptoms. In terms of otoneurological symptoms, In relation to lifestyle, only 23.1% of institu
-tionalized elderly persons consumed alcoholic beverages the period in which the data were collected. The same percentage smoked, while 76.9% did not perform any type of physical activity. All of those that did exercise, walked.
Exam Patient
1 2 3 4 5 6 7 8 9 10 11 12 13
Examination of the head and neck - - -
-Test for spontaneous and gaze evoked
nystagmus using Frenzel goggles - - - -Pursuit (semi-spontaneous nystagmus) - - -
-Saccades + + - - - + - -
-Head impulse - - + + - + - + - - + -
-Headshake - - - + - - - +
-Dynamic visual acuity - - - + - - + - +
Fixation Suppression - - - + - - - -
-Dix-Hallpike Positional Test - + + + + + + - + + - -
-Cerebellar tests - - -
-Romberg test + - - + + - - + - - + -
-Key: +: results showing disorders; -: normal results
Figure 2 – Results of the evaluation of vestibulopathy in elderly persons with dizziness, in
accordance with the criteria of Johnson and Lalwani (2004). Only elderly persons considered to have vestibulopathy are shown.
used hearing aid ampliication and only two elderly persons needed a cane or walker to walk (Table 2).
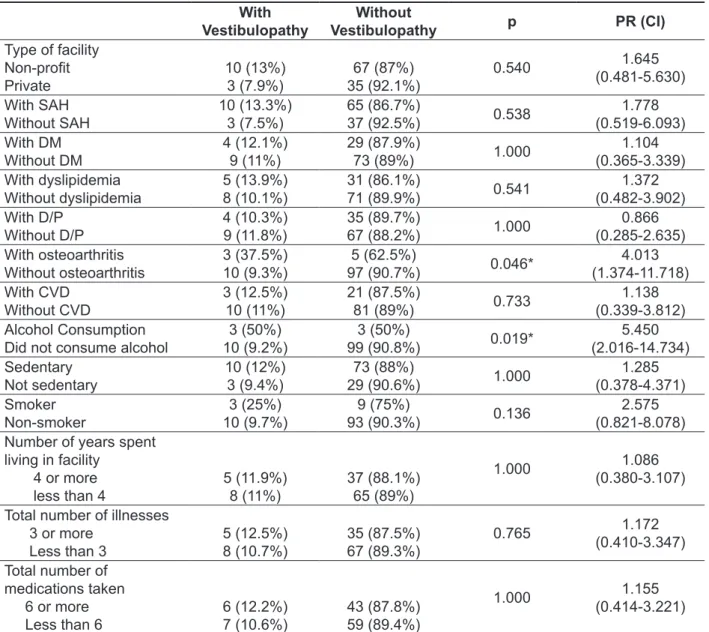
Bivariate analysis identiied an association between osteoarthritis and alcohol consumption
(Table 3).
most did not complain of tinnitus, hearing loss or aural fullness. Most of the elderly persons had good visual acuity (detected by self-reporting and the screening test performed with the Snellen Chart), despite the fact that many of them used glasses. None of the subjects with vestibulopathy
Table 2 – Characteristics of dizziness, symptoms and associated physical conditions in elderly
persons with vestibulopathy in Nursing homes in Natal. Natal, Brazil, 2013.
N %
Type of dizziness
Vertigo
Imbalance
Floating sensation
Floating sensation + Presyncope
Floating Sensation + Vertigo
3 6 2 1 1
23.1 46.2 15.4 7.7 7.7
Duration of dizziness Seconds
Minutes Hours Days
6 5 1 1
46.2 38.5 7.7 7.7
Presence of neurovegetative symptoms
No Yes
10 3
76.9 23.1
Presence of tinnitus
No
Yes unilateral Yes bilateral
7 3 3
53.8 23.1 23.1
Presence of hearing loss
No
Yes unilateral Yes bilateral
9 1 3
69.2 7.7 23.1
Presence of aural fullness
No
Yes unilateral Yes bilateral
10 2 1
76.9 15.4 7.7
Signiicant reduction in visual acuity
No Yes
12 1
92.3 7.7
Use of glasses
No Yes
5 8
38.5 61.5
Use of hearing aid
No 13 100
Use of cane/walker
No Yes
11 2
Test, was 61.53%, a value slightly higher than previously available information. It is likely that this higher prevalence is due to the age range in this sample, as it is known that the prevalence of BPPV increases with age6.
The elderly persons who sufered from vestibu
-lopathy were mostly female and had a median age of 78 years. These results are similar to a Brazilian study which found that 76.6% of elderly people with vestibulopathy were women, with a mean age of 73.62 years30, and another which
identiied that 68.3% were women, with a mean age of 73.40 years31. An American study identiied
a lower proportion of women with vestibular DISCUSSION
The prevalence of vestibulopathy among the general population is between 10 and 30%, rising to 35% among those aged over 40 years27-29. In
the present study, the prevalence of vestibulopathy among the total population of seniors eligible for the study was 10.56%, which is consistent with the indings for diagnosis at the population level.
Among the causes of vestibulopathy, BPPV has been described as the most common cause among elderly persons9. In the present study, the preva
-lence of BPPV, diagnosed using the Dix-Hallpike
Table 3 – Statistical signiicance (p), Prevalence Ratio (PR) and Conidence Interval (CI) of variables
related to vestibulopathy in Nursing homes in Natal. Natal, Brazil, 2013.
With Vestibulopathy
Without
Vestibulopathy p PR (CI)
Type of facility Non-proit
Private
10 (13%)
3 (7.9%) 35 (92.1%)67 (87%) 0.540
1.645 (0.481-5.630)
With SAH
Without SAH 10 (13.3%)3 (7.5%) 65 (86.7%)37 (92.5%) 0.538 (0.519-6.093)1.778
With DM
Without DM 4 (12.1%)9 (11%) 29 (87.9%)73 (89%) 1.000 (0.365-3.339)1.104
With dyslipidemia
Without dyslipidemia 5 (13.9%)8 (10.1%) 31 (86.1%)71 (89.9%) 0.541 (0.482-3.902)1.372
With D/P
Without D/P 4 (10.3%)9 (11.8%) 35 (89.7%)67 (88.2%) 1.000 (0.285-2.635)0.866
With osteoarthritis
Without osteoarthritis 3 (37.5%)10 (9.3%) 97 (90.7%)5 (62.5%) 0.046* (1.374-11.718)4.013
With CVD
Without CVD 3 (12.5%)10 (11%) 21 (87.5%)81 (89%) 0.733 (0.339-3.812)1.138
Alcohol Consumption
Did not consume alcohol 10 (9.2%)3 (50%) 99 (90.8%)3 (50%) 0.019* (2.016-14.734)5.450
Sedentary
Not sedentary 10 (12%)3 (9.4%) 29 (90.6%)73 (88%) 1.000 (0.378-4.371)1.285
Smoker
Non-smoker 10 (9.7%)3 (25%) 93 (90.3%)9 (75%) 0.136 (0.821-8.078)2.575
Number of years spent living in facility
4 or more
less than 4 5 (11.9%)8 (11%) 37 (88.1%)65 (89%)
1.000 1.086
(0.380-3.107)
Total number of illnesses 3 or more
Less than 3 5 (12.5%)8 (10.7%) 35 (87.5%)67 (89.3%) 0.765
1.172 (0.410-3.347)
Total number of medications taken 6 or more
Less than 6 6 (12.2%)7 (10.6%) 43 (87.8%)59 (89.4%)
1.000 1.155
(0.414-3.221)
Legend: SAH: systemic arterial hypertension, DM: diabetes mellitus D/P: dementia or psychosis, CVD: cardiovascular disease. *:
elderly person presents degeneration in various systems related to body balance6, it is common for
elderly patients with vestibular disorders to sufer from diferent types of dizziness, and perhaps even from a combination of types.
The presence of associated neurotological symptoms was also evident among elderly persons with vestibulopathy, as almost half had tinnitus, approximately 30% reported hearing loss, and 23.1% aural fullness. These symptoms are usually present due to lesions involving the cochlear portion of the VIII nerve. Autors31 found slightly higher values
(70.8% tinnitus, 60% hearing loss and 54.2% aural fullness), but this was based on a sample of outpa
-tients, who tend to sufer from a greater number of health complaints than the general population.
Alcohol consumption was found to be associated with vestibulopathy in the present study, as elderly persons who consumed alcohol were 5.45 times more vestibular disorders than those who did not consume alcoholic beverages. There was also an association between osteoarthritis and vestibulopathy, with elderly patients with this disease presenting four times more likely to sufer from vestibulopathy that those who did not. The literature presents studies where alcohol was identiied as a risk factor for dizziness in idosos 33,34, conirming the
above data. This data conirms that proprioception is involved in maintaining body balance and that alterations in its homeostasis may relect disorders in the vestibular system. A chronic alcoholic patient would therefore sufer from proprioception and consequent vestibular damage
CONCLUSIONS
Vestibular disease was found in 10.56% of institutionalized elderly persons in Natal, Brazil, with BPPV identiied as the most common cause. Vestibulopathy was more prevalent among elderly persons who consumed alcohol, and those with osteoarthritis.
disorders (51%)27. In all studies involving the elderly
population, the presence of a higher percentage of women than men is a striking feature. This is due to the greater presence of older women in the general population, as they have a higher life expectancy.
The number of diseases which elderly persons with vestibulopathy sufered from, as well as the number of medications used, were comparable to data in existing literature, which shows the mean number of diseases per person to be between 1.25 and 3.98 (in the present study the median was two diseases per person) and the mean number of medications to be between 3.86 and 4.08 (in the present study a slightly higher number was found, with a median of ive types of medication per elderly person)11,30-32. In this aspect, the institutionalized
elderly person with vestibular disorders has a similar proile to the elderly patient living in the community.
Existing literature shows that cardiovascular, metabolic and osteoarticular diseases are most associated with vestibulopathy, and may also be related to the genesis of the condition11,30-32. In
the present study, SAH was the most frequently observed associated disease among the group of elderly patients with vestibular disease, while dyslip
-idemia and diabetes also represented signiicant metabolic changes. However, no statistical associ
-ation was found between these conditions and the emergence of vestibulopathy. A high number of comorbidities and the efect of individual diseases cannot, however, be eliminated as associated factors, as the present study is limited by the small the sample size used.
Similarly, the number of medications taken was not found to be statistically signiicant in the present study, but the absence of statistical signiicance does not rule out the efects of polypharmacy. This just was not identiied statistically.
13. Walker MF, Zee DS. Bedside vestibular examination. Otolaryngol Clin North Am.
2000;33(3):495-506.
14. Kheradmand A, Zee DS. The bedside examination of the vestibulo-ocular relex (VOR): an update. Rev Neurol (Paris). 2012;168(10):710-9. 15. Lo AX, Harada CN. Geriatric dizziness. Evolving diagnostic and therapeutic approaches for the emergency department. Clin Geriatr Med.
2013;29(1):181-204.
16. Gonçalves DU, Ganança FF, Bottino MA, Greters ME, Ganança MM, Mezzalira R et al. Otoneurological evaluation: current good practice. Braz J Otorhinolaryngol. 2014;80(2):95.
17. Drachman DA, Hart CW. An approach to the dizzy patient. Neurology. 1972;22(4):323-34. 18. Johnson J, Lalwani AK. Vestibular Disorders. In: Lalwani AK, editor. Current Diagnosis and Treatment in Otolaryngology: Head and Neck Surgery. New York: Lange Medical Books/McGraw-Hill; 2004. p
761-70.
19. Sociedade Brasileira de Otorrinolarigologia - SBORL. Fórum sobre vertigem. Braz J Otorhinolaryngol. 2003;69(4):1-36.
20. Campana, DR,Ribeiro MQ. Avaliação clínica da orelha.Audição e Equilíbrio. In: SBORL. Tratado de Otorrinolaringologia. São Paulo: Rocca, 2003,v. 1. p. 430-40
21. Petersen JA, Straumann D, Weber KP. Clinical diagnosis of bilateral vestibular loss: three simple bedside tests. Ther Adv Neurol Disord.
2013;6(1):41-5.
22. Angeli SI, Velandia S, Snapp H. Head-shaking nystagmus predicts greater disability in unilateral peripheral vestibulopathy. American Journal of Otolaryngology. 2011;32:522-7.
REFERENCES
1. Ganança MM. Vestibular disorders in the elderly. Braz J Otorhinolaryngol. 2015;81:4-5.
2. Dolci J, Santos MAO. Labyrinth disorders. Rev Bras Med. 2013;70:59-65.
3. Kutz Junior JW. The dizzy patient. Med Clin North Am. 2010;94(5):989-1002.
4. Ferreira LMBM, Ribeiro KMOBF, Pestana ALS, Lima KC. Prevalence of dizziness in older people.
Rev CEFAC. 2014;16(3):739-46.
5. Santana GG, Doná F, Ganança MM, Kasse CA. Vestibulopatia no idoso. Saúde Colet.
2011;8(48):52-6.
6. Marchetti GF, Whitney SL. Older adults and balance dysfunction. Neurol Clin. 2005;23(3):785-805. 7. Alrwaily M, Whitney SL. Vestibular rehabilitation of older adults with dizziness. Otolaryngol Clin North Am. 2011;44(2):473-96.
8. Barin K, Dodson EE.Dizziness in the elderly. Otolaryngol Clin North Am. 2011;44(2):437-54. 9. Iwasaki S, Yamasoba T. Dizziness and Imbalance in the Elderly: Age-related Decline in the Vestibular System. Aging Dis. 2015;6(1):38-47.
10. Dros J, Maarsingh OR, van der Horst HE, Bindels PJ, Ter Riet G, van Weert HC. Tests used to evaluate dizziness in primary care. Can Med Assoc J. 2010;182(13):621-31.
11. Ahearn DJ, Umapathy D. Vestibular impairment in older people frequently contributes to dizziness as part of a geriatric syndrome. Clin Med. 2015;15(1):
25-30.
12. Tusa RJ. Bedside Assessment of the Dizzy
Patient. Neurol Clin. 2005;23(3):655-73.
RESUMO
Objetivo: aferir a prevalência de vestibulopatia e seus fatores associadosem idosos institucionaliza
-dos por meio do exame clínico de cabeceira. Métodos: trata-se de um estudo transversal realizado
nas 12 Instituições de longa permanência para idosos de Natal-Brasil, regulamentadas pela Vigilância Sanitária. Foram eleitos os idosos com bom nível cognitivo e capazes de deambular, totalizando 115 indivíduos. Os idosos foram questionados sobre a presença de tontura no último ano, e quando a resposta era positiva, eram submetidos a questionário e exame físico especíico para diagnóstico de vestibulopatia, segundo o protocolo de Johnson e Lalwani (2004). Para a análise estatística, utilizou
--se o teste do Qui-quadrado ou exato de Fisher para um nível de signiicância de 5% e cálculo da razão de prevalência. Resultados: a prevalência de vestibulopatia foi de 10,56%e foram associados
a osteoartrose e o etilismo. Conclusão: a vestibulopatia apresenta baixa prevalência nos idosos ins
-titucionalizados de Natal-Brasil.
30. Gazzola JM, Ganança FF, Aratani MC, Perracin MR, Ganança MM. Circumstances and consequences of falls in elderly people with vestibular disorder. Braz J Otorhinolaryngol.
2006;72(3):388-93.
31. Gazzola JM, Ganança FF, Aratani MC, Perracini MR, Ganança MM. Clinical evaluation of elderly people with chronic vestibular disorder. Braz J Otorhinolaryngol. 2006;72(4):515-22.
32. Bittar RMS, Simoceli L, Pedalini MEB, Bottino MA. The treatment of diseases related to balance disorders in the elderly and the efectiveness of vestibular rehabilitation. Braz J Otorhinolaryngol.
2007;73(3):295-8.
33. Pluijm SM, Smit JH, Tromp EA, Stel VS, Deeg DJ, Bouter LM et al. A risk proile for identifying community-dwelling elderly with a high risk of recurrent falling: results of a 3-year prospective study. Osteoporos Int. 2006;17(3):417-25.
34. Bellé M, Sartori Sdo A, Rossi AG. Alcoholism: efects on the cochleo-vestibular apparatus. Braz J Otorhinolaryngol. 2007;73(1):110-6.
23. Lopez-Escamez JA, Zapata C, Molina MI, Palma MJ. Dynamics of canal response to head-shaking test in benign paroxysmal positional vertigo. Acta Oto-Laryngologica. 2007;127:1246-54.
24. Silva ALS, Marinho MRC, Gouveia FMV, Silva JG, Ferreira AS, Cal R. Benign Paroxysmal Positional Vertigo: Comparison of two recent international guidelines. Braz J Otorhinolaryngol.
2011;77(2):191-200.
25. Sociedade Brasileira de Otorrinolaringologia - SBORL. Consenso sobre vertigem. Braz J Otorhinolaryngol. 2000;66(6):1-38.
26. Zapparoli M, Klein F, Moreira H. Avaliação da acuidade visual Snellen. Arq Bras Oftalmol. 2009;
72(6): 783-8.
27. Agrawal Y, Carey JP, Della Santina CC, Schubert MC, Minor LB. Disorders of balance and vestibular function in US adults: data from the National Health and Nutrition Examination Survey, 2001–2004. Arch Intern Med. 2009;169:938-44.
28. Teixeira LJ. Vertigem, reabilitação vestibular e demanda social. Rev Neurocienc. 2009;17(2):102. 29. Post RE, Dickerson LM. Dizziness: A diagnostic approach. Am Fam Physician.2010;82(4):361-8.
Received on: February 24, 2015 Accepted on: June 29, 2015
Mailing address:
Lidiane Maria de Brito Macedo Ferreira
Universidade Federal do Rio Grande do Norte,
Centro de Ciências da Saúde, Departamento de
Odontologia
Av. Salgado Filho, 1787, Lagoa Nova
Natal - RN – Brasil CEP: 59056-000