REVISTA
BRASILEIRA
DE
REUMATOLOGIA
ww w . r e u m a t o l o g i a . c o m . b r
Original
article
Vaccination
in
patients
from
Brasília
cohort
with
early
rheumatoid
arthritis
Luciana
Feitosa
Muniz
∗,
Carolina
Rocha
Silva,
Thaís
Ferreira
Costa,
Licia
Maria
Henrique
da
Mota
HospitalUniversitáriodeBrasília,UniversidadedeBrasília,Brasília,DF,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received15June2012 Accepted7April2014
Availableonline21August2014
Keywords:
Vaccine
Earlyrheumatoidarthritis Brazilianpopulation
a
b
s
t
r
a
c
t
Introduction:Patientswithadiagnosisofrheumatoidarthritis(RA)areatincreasedriskof infections.Vaccinationisarecommendedpreventivemeasure.Therearenostudies evalu-atingthepracticeofvaccinationinpatientswithearlyRA.
Objectives: Toevaluatethefrequencyofvaccinationandtheorientation(bythedoctor)about vaccinesamongpatientswithearlyRAdiagnosis.
Methods:Cross-sectionalstudyincludingpatientsfromtheearlyRABrasiliacohort. Demo-graphicdata,diseaseactivityindex(DiseaseActivityScore28–DAS28),functionaldisability (HealthAssessmentQuestionnaire–HAQ),anddataontreatmentandvaccinationafter diagnosisofRAwereanalyzed.
Results:Sixty-eight patients wereevaluated,94.1% women, mean age 50.7±13.2 years. DAS28was3.65±1.64,andHAQwas0.70.Mostpatients(63%)hadvaccinationcard.Only fivepatients(7.3%)werebriefedbythedoctorabouttheuseofvaccines.Patientswere vac-cinatedforMMR(8.8%),tetanus(44%),yellowfever(44%),hepatitisB(22%),influenza(42%), H1N1(61.76%),pneumonia(1.4%),meningitis(1.4%),andchickenpox(1.4%).Allpatients vac-cinatedwithliveattenuatedviruswereundergoingimmunosuppressivetherapy,andwere vaccinatedinadvertently,withoutmedicalsupervision.Therewasnoassociationbetween theuseofanyvaccineanddiseaseactivity,functionaldisability,yearsofeducation,lifestyle, andcomorbidities.
Conclusion: Patientswereinfrequentlybriefedbythephysicianregardinguseofvaccines, with highfrequencyofinadvertent vaccinationwithlive attenuatedcomponent,while immunizationwithkilledviruswasbelowtherecommendedlevel.
©2014ElsevierEditoraLtda.Allrightsreserved.
DOIoforiginalarticle:http://dx.doi.org/10.1016/j.rbr.2014.04.002.
∗ Correspondingauthor.
E-mail:[email protected](L.F.Muniz). http://dx.doi.org/10.1016/j.rbre.2014.04.002
Vacinac¸ão
em
pacientes
da
Coorte
Brasília
de
artrite
reumatoide
inicial
Palavraschave:
Vacina
Artritereumatoideinicial Populac¸ãobrasileira
r
e
s
u
m
o
Introduc¸ão: Ospacientes comdiagnósticode artrite reumatoide(AR)apresentam risco aumentado deinfecc¸ões.A vacinac¸ãoéumamedidapreventivarecomendada. Nãohá estudosavaliandoapráticadavacinac¸ãonospacientescomARinicial.
Objetivos:Avaliarafrequênciadevacinac¸ãoeaorientac¸ão(feitapelomédico)sobrevacinas entreospacientescomdiagnósticodeARinicial.
Métodos:EstudotransversalincluindopacientesdacoorteBrasíliadeARinicial.Foram anal-isadosdadosdemográficos,índicedeatividadedadoenc¸a(DiseaseActivityScore28–DAS28), incapacidadefuncional(HealthAssessmentQuestionnaire–HAQ),dadossobretratamentoe vacinac¸ãoapósodiagnósticodaAR.
Resultados: Foramavaliados68 pacientes,sendo94,1% mulheres,comidade média de 50,7±13,2anos.ODAS28foide3,65±1,64,eoHAQde0,70.Amaioriadospacientes(63%) possuíacartãovacinal.Apenascincopacientes(7,3%)foramorientadospelomédicosobre usodasvacinas.Ospacientesforamvacinadosparatrípliceviral(8,8%),tétano(44%),febre amarela(44%),hepatiteB(22%),gripe(42%),influenzaH1N1(61,76%),pneumonia(1,4%), meningite(1,4%)evaricela(1,4%).Todosospacientesvacinadoscomvírusvivoatenuado estavamemusodeimunossupressoresereceberamasvacinasdeformainadvertida,sem orientac¸ãomédica.Nãohouveassociac¸ãoentreousodenenhumavacinaeatividadeda doenc¸a,incapacidadefuncional,anosdeescolaridade,hábitosdevida,comorbidades.
Conclusão: Ospacientesforampoucoorientadospelomédicocomrelac¸ãoaousodas vaci-nas,comelevadafrequênciadevacinac¸ãoinadvertidacomcomponentevivoatenuado, enquantoaimunizac¸ãocomvírusmortosficouaquémdorecomendado.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Infectionsareanimportantcauseofmorbidityand mortal-ityinpatientswithrheumatoidarthritis(RA).1Itisestimated
thatthesepatientshaveatwo-foldriskofdeveloping infec-tionwhencomparedtohealthysubjectsofthesamesexand age.Theincreasedinfectioussusceptibilityisduenotonlyto thetreatmentused,buttothediseaseitselfandtoassociated comorbidities.2 Infections occur morefrequently in joints,
bones,skin,softtissues,andrespiratorytract,2being
respon-sible,atleastinpart,foranincreaseinmortalityinpatients withRA,especiallywhentheyoccurinthegenitourinaryand bronchopulmonarytracts.3–6
Vaccination is the primary preventive measure against infectiousdiseases.7InpatientswithRA,dependingonthe
stateofimmunosuppression,theimmunogenicityofthe vac-cinationmaybereduced,butisstilleffective.8Therearesome
casesofRAreportedfollowingtheuseofthevaccine, espe-ciallyagainsthepatitisB,butthereisnoevidenceofacausal relationshipestablished.Thus,currentlytheadministrationof mostvaccinesrecommendedbythenationalimmunization schedulecanbeperformedsafely withnoeffectondisease activity.7–9
Theuseofvaccinesnotcontaininglivingorganisms,such asthose forinfluenza(intramuscular),pneumonia,tetanus, diphtheria,pertussis,HaemophilusinfluenzaetypeB(Hib), hep-atitisAandBvirus,polio(inactivated–IPV),meningitisand humanpapillomavirus (HPV),isrecommendedinpatients withrheumaticdiseases,includingRA.8,10Amongthose,the
influenzaandpneumococcalvaccinesarethemostsuitable, withahigherlevelofevidenceregardingsafetyandefficacy. Allvaccinesshouldbeadministeredpreferablybeforethestart oftreatmentwithsyntheticor biologicaldisease-modifying antifheumaticdrugs(DMARDs),totrytoachieveanadequate immuneresponse.8,11
Theattenuatedlivevaccinesshouldbeavoided,whenever possible,inpatientswithrheumaticdiseases.8Includedinthis
grouparethefollowingvaccines:MMR(measles,mumps,and rubella),BCG,influenza(nasal),chickenpox,shingles,typhoid, polio (OPV), smallpoxandyellow fever.However,onemust makeanindividualizedassessmentofpatients,considering the degreeof immunosuppressionand the risk factors for acquiringtheseinfections.8,12,13
Despite therecommendationsfortheuseofvaccinesin patients with rheumatic diseases, the frequency of vacci-nation issuboptimal, reaching amaximum of20%-35% in immunosuppressed patients.14 However, few studies have
evaluatedthevaccinationcoverageofRApatients,withmost studiesevaluating onlyinfluenzaorantipneumococcal vac-cines.
The only study evaluating vaccination in patients with earlyRAshowedthattheresponseofpneumoniavaccinewas lowerthanthatseeninthenormalpopulation.Moreover,that studyalsonotedthattheadditionofinfliximabtothetherapy withmethotrexatedidnotaffecttheresponsetothevaccine.15
TheBrazilianSocietyofRheumatologyhasrecentlyissued recommendationsonvaccinationinpatientswithRA.16
Thus,thisstudyaimstoevaluatethefrequencyof vacci-nationamongpatientswithearlyRAdiagnosisandverifythe orientationregardingtheuseofvaccinesgivenbydoctorsto patients.
Patients
and
methods
Across-sectionalstudyfromFebruary 2012toJune2012,as partoftheBrasiliaCohortofEarlyRheumatoidArthritis,was carriedout.17–20 DatacollectionwasperformedattheClinic
ofRheumatology,HospitalUniversitáriodeBrasília, Universi-dadedeBrasília(HUB/UnB).Weincludedpatientsolderthan18 yearsdiagnosedwithearlyRA(lessthanoneyearofsymptoms atdiagnosis).
Patientsparticipatedvoluntarilyinthestudy,after clarifi-cationonthecontentoftheresearchandaftersigningafree informedconsentform.ThestudywasapprovedbytheEthics CommitteeoftheFacultyofMedicine,UniversidadedeBrasília (CEP/FM-028/2007).
Allparticipantswereassessedbydirectinterviewinroutine outpatientconsultations.Thevaccinationcard,when avail-able,wascheckedbyevaluatingthosevaccinesusedafterthe diagnosisofRA.Ifthesepatientsdidnotpossessthe vaccina-tioncard,theywereaskedspecificallyabouteachandevery oneof the national immunization schedule recommended vaccinesforadultsandelderlypatients:seasonalinfluenza, 23-valentpneumococcal–Pn23,MMR,tetanus-diphteria(Td), hepatitisB,andyellowfever.21Moreover,theywereevaluated
withrespecttotheuseofothervaccines:measles, meningo-coccal,and humanpapillomavirus(HPV) vaccines.Patients were also asked if they had received some guidance from theaccompanyingphysicianonwhichvaccinestheywould orwouldnotuse.
Informationaboutage,timesincediagnosis,disease activ-ity index (Disease Activity Score 28 – DAS28), functional disability questionnaire (Health Assessment Questionnaire – HAQ), use of synthetic or biologic DMARDs (medication, dose),lifestyle (physical activity,currentor previous smok-ing),education,andcomorbiditieswerealsoobtainedthrough questionnairesandmedicalrecordreviews.Patientswerethen divided into groups, accordingto whether ornot theyhad receivedeachofthevaccineslistedabove.
Descriptivestatistical analysiswas usedtoevaluatethe generalcharacteristicsofthestudypopulation.TheStudent’s
t-testorMann-Whitneytestwasusedtoanalyzecontinuous variables.Categoricalvariableswereanalyzedbychi-squared orFisher’sexacttest,whenappropriate.Thesignificancelevel of5%(p<0.05)wasusedforallstatisticaltests.
Results
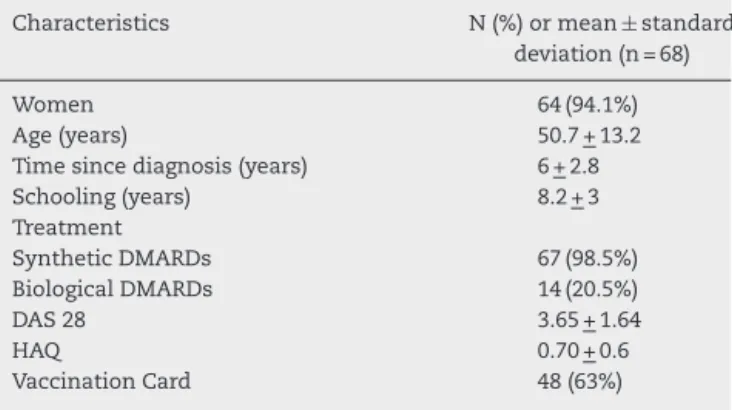
Sixty-eightpatientswithearlyRAwereevaluated.The gen-eral characteristics of the patients are shown in Table 1. Regardingthetreatmentwithimmunosuppressivedrugs,55 (80%)patientsweretakingmethotrexate,18(26%) antimalar-ialdrugs,17(25%)leflunomide,8(11%)sulfasalazine,13(19%) prednisone,6(8.8%)infliximab,1(1.4%)etanercept,2(2.9%) adalimumab,4(5.8%)rituximab,and2(2.9%)abatacept.
Table1–Generalcharacteristicsofpatientsdiagnosed withearlyRAevaluatedforvaccination.
Characteristics N(%)ormean±standard deviation(n=68)
Women 64(94.1%)
Age(years) 50.7+13.2
Timesincediagnosis(years) 6+2.8
Schooling(years) 8.2+3
Treatment
SyntheticDMARDs 67(98.5%)
BiologicalDMARDs 14(20.5%)
DAS28 3.65+1.64
HAQ 0.70+0.6
VaccinationCard 48(63%)
Of the total group, only five patients (7.3%) had been briefed by the doctor about the use of vaccines. Patients whounderwentvaccinationwithoutreceivingspecific med-ical recommendation made it on their own, inadvertently, at the suggestion of the media or of third parties (rela-tives/neighbours/acquaintances).
AftertheRAdiagnosis,theuseofsomekindofinactivated orrecombinantvaccinewasobservedin57(84%)patients;and theuseofkindofliveattenuatedvaccinewasobservedin32 (47%)patients.Thevaccinationwascarriedoutasfollows:6 (8.8%)forMMR(measles,rubella,andchickenpox),30(44%)for dT,30(44%)foryellowfever,15(22%)forhepatitisB,29(42%) forinfluenza,42(61.7%)forH1N1,4(5.8%)forpneumonia,1 (1.4%)formeningitis,and1(1.4%)forvaricella(1.4%).
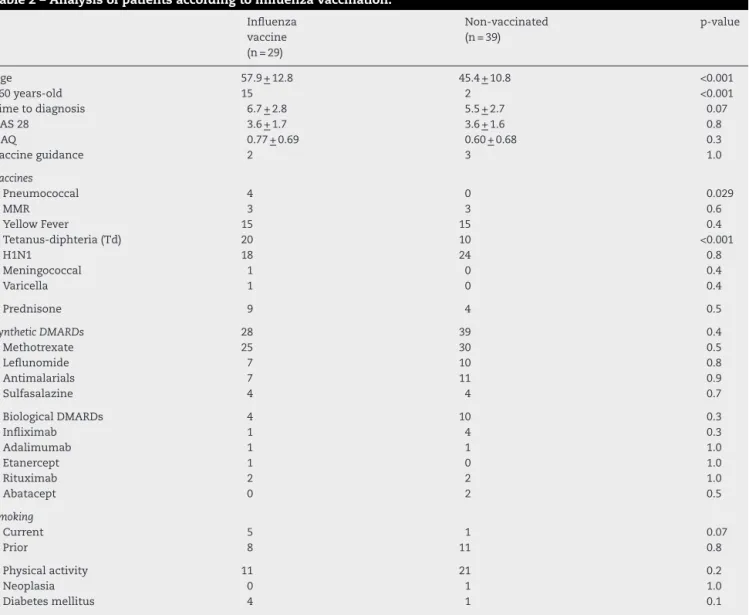
Table 2shows the analysis ofthe characteristics of the groupthatreceivedseasonalinfluenzavaccinecomparedto thegroupofpatientswho didnotreceivethisvaccine.The sameanalysiswasdoneforallvaccinesunderstudy.
No association among the use of any vaccine and dis-easeactivity,functionaldisability,physicalactivity,smoking, andyearsofschoolingwasnoted.Similarly,nodifferencein frequency ofcomorbid conditionsthat could influence the indicationoftheuse ofsomevaccines,suchascancerand diabetesmellitus,wasobserved.Nopatienthadchroniclung diseaseorischemicheartdisease.Theguidanceonwhich vac-cinepatientsshouldorshouldnotusedidnotresultinhigher or lower frequency of using any vaccine. Also in patients vaccinated against H1N1 influenza, therewas no observed differenceinrelationtodrugtherapyoruseofothervaccines. Withregardtoage,patientswhoreceivedhepatitisBand MMR vaccineswere younger (44±12 versus53±13,p=0.03 and 37±9.5 versus 52±13; p=0.01, respectively). The time todiagnosisofRAwaslongerinthegroupthatreceivedTd (6.8±2.7versus5.4±2.7,p=0.03)andinthosewhousedH1N1 influenzavaccine(6,7±2.6versus5±2.9,p=0.01).Thegroup thatreceivedantipneumococcalvaccinepresentedhigherrate ofpatientsabove60years(75%versus22%,p=0.04).
Patientsusingdoubleadult-typevaccinealsomademore frequentuseofMMR(20%versus0%,p<0.005),hepatitisB(47%
versus26%,p<0.001)andyellowfever(63%versus29%,p=0.01) vaccines,comparedtothegroupthathasnotbeenvaccinated withTd.
Table2–Analysisofpatientsaccordingtoinfluenzavaccination.
Influenza vaccine (n=29)
Non-vaccinated (n=39)
p-value
Age 57.9+12.8 45.4+10.8 <0.001
>60years-old 15 2 <0.001
Timetodiagnosis 6.7+2.8 5.5+2.7 0.07
DAS28 3.6+1.7 3.6+1.6 0.8
HAQ 0.77+0.69 0.60+0.68 0.3
Vaccineguidance 2 3 1.0
Vaccines
Pneumococcal 4 0 0.029
MMR 3 3 0.6
YellowFever 15 15 0.4
Tetanus-diphteria(Td) 20 10 <0.001
H1N1 18 24 0.8
Meningococcal 1 0 0.4
Varicella 1 0 0.4
Prednisone 9 4 0.5
SyntheticDMARDs 28 39 0.4
Methotrexate 25 30 0.5
Leflunomide 7 10 0.8
Antimalarials 7 11 0.9
Sulfasalazine 4 4 0.7
BiologicalDMARDs 4 10 0.3
Infliximab 1 4 0.3
Adalimumab 1 1 1.0
Etanercept 1 0 1.0
Rituximab 2 2 1.0
Abatacept 0 2 0.5
Smoking
Current 5 1 0.07
Prior 8 11 0.8
Physicalactivity 11 21 0.2
Neoplasia 0 1 1.0
Diabetesmellitus 4 1 0.1
(0%versus32%,p=0.015).Patientsvaccinatedagainsthepatitis BalsousedmorefrequentlyMMR(33%versus19%,p=0.01).
Allpatientsvaccinatedwithliveattenuatedviruses(MMR, varicellaandyellowfever)wereonimmunosuppressive ther-apy. In all these cases, the vaccination occurred without guidancegivenbyRheumatologyDepartmentphysicians.
Discussion
DespitetheincreasedinfectioussusceptibilityofRApatients and the importance of vaccination, the practice of pas-siveimmunizationhasbeenperformedimproperlyinthese patients.10,14 OurstudyshowedthatBrasiliacohortpatients
received little guidance (7.3%) from the physician as to whetherornottousevaccinesingeneral,orspecificallyin relationtocontraindicationsoflivevirusvaccines.Thus,most ofvaccinatedpatientsinourearlyRAservicereceivedthe vac-cineontheirown,regardlessofmedicaladvice.Thisfinding isveryimportant,becausetheBrasiliacohortisfollowed-up atanoutpatient rheumatology tertiary careservice, where therecommendationsforvaccinationinimmunosuppressed patientsshouldbeobserved.
Thelackofrecommendationbyprofessionalsfroma ter-tiary care service makesus wonderabout the situation in relation to the recommendation tobe vaccinated in other primary and secondary care centers in our country, and emphasizestheimportanceofgreaterdisclosureand atten-tionforthatmatter.
Workdoneinothercountriesshowedhigherfrequencyof medicalguidanceastovaccination,withproportionsranging from 45% to 95%.22–25 We observed no influence of
guid-anceontheuseofanyvaccine.However,Doeetal.showed improvementintherateofinfluenzavaccinationafter guid-anceoptimizationfromhealthprofessionals,anincreaseof 56%to72%infouryearsofobservation.22,23
Besides medical guidance, other factors influence vac-cination coverage, for instance, vaccination offered at the hospital,allergytovaccinecomponents,andpreviousadverse reactions.22–27 The length of rheumatologists’ professional
practice may also interfere with the frequency of passive immunization. Desai et al. showed a higher proportion of patients vaccinated against pneumonia in the group of rheumatologists with ≤ 10 years of practice.28 However,
influenceoftimeofprofessionalpractice.29Intheearly
arthri-tis outpatient service wherethis study was conducted, all rheumatologistshave≤10yearsofpractice.
Wefoundthattheuseofsomevaccines,suchasinfluenza, tetanus,andhepatitisB,was animportantfactor forusing othervaccines.Thismayhavehappenedthankstothebest advicegiventothesepatientsabouttheimportanceof vacci-nationingeneral.Furthermore,intheplaceofapplicationofa particularvaccine(asoccursinprimaryhealthservices)other vaccinesmayhavebeenprovided,inaccordancewithageand riskofacquiringotherinfections.
Regardingvaccinationagainstinfluenza,weshowedthat vaccinationcoverage (42%)was suboptimal,similar tothat reportedinotherstudiesforRA.14,22,23InBrazil,thesepatients
arethetargetoftheNationalCampaignforElderly Vaccina-tion,whichoccursannually.Thegoalofthecampaignisto vaccinate80%ofthetargetpopulationagainstinfluenza,and, in2011,ithasachieved84%vaccinationcoverage.30The
vac-cinationforpneumoniawasstilllessfrequent(5.8%),andall patientswerealsovaccinatedforinfluenza.Thesevaluesare lowerthanthosereportedintheliterature,rangingfrom20.2% to43%.25,28 Age over 60years wasa factor thatinfluenced
vaccinationagainst influenza and pneumonia,as alsowas observedinothercountries,24,28,31whichispossiblyexplained
bytheextensivemediacoverageoftheNationalCampaignfor ElderlyVaccination.
Thevaccine againstH1N1influenza was themostused byourpatients(61.7%),thankstoanationalcampaigndue tothepandemicin2009,whichincludedimmunosuppressed patients.Thisdemonstratesthatwhenpatientsarebetter tar-geted,thevaccinationcoverage canbemoreeffective.In a BrazilianstudyofRApatients,thevaccinewaswelltolerated andsafe,despitealowerseroconversion.32
Infectionsinpatients withRAhavegained greater con-cernwiththeemergenceoftheso-calledbiologicalagents, including inhibitors of tumor necrosis factor-alpha (anti-TNF␣), rituximab, tocilizumab, and abatacept. These drugs arecommonlyusedincombinationwithtraditionalDMARDs, further increasing the immunosuppressive effect of these drugs.10Theuseofrituximabmaycompromisetheresponse
ofsomeimmunizations,suchaspneumococcalandflu vac-cines,duetoitsmechanismofaction;thus,theadministration of these vaccines is recommended before beginning that medication.8,33
Feutchtenbegeretal. noted a higherrate ofvaccination againstinfluenzaandStreptococcuspneumoniaeinpatientswho wereonanti-TNForrituximab.25However,nodifferencewas
observedinrelationtomedicaladviceornotvaccinationin patientswhowere usingbiologicals. Inpatientsvaccinated againsthepatitisB,leflunomidewaslessused–anapparently fortuitousfinding.Wedidnotobserveanincreasedpresence ofliverdiseaseinthesepatients.
Patients vaccinated for viral hepatitisB and MMR were younger.ThisisbecausethetargetpopulationforMMR vac-cinearewomen20-49yearsandmen20-39years.Likewise,the nationalimmunizationschedulerecommendshepatitisB vac-cinationforadultsbelongingtoriskgroupssuchaspregnant women,healthprofessionals,workersofdifferentareas,and riskysexualgroups.Thispopulationisalsooftenquotedas beingyounger.21
Thelow frequencyofuse ofvaricellaand antimeningo-coccalvaccinesisjustifiedbythenon-routineofferofthese vaccinesbythepublichealthsysteminBrazil.Therewasno registryofuseofHPVvaccine,whichisalsocurrentlyoffered byprivatemedicalservices.
Vaccinationwithliveattenuatedcomponents(MMR, vari-cellaandyellowfever)wasveryfrequentandinadvertently made.Theuseofliveattenuatedvaccinesshouldbeavoided when possible, but these products may be generally used inmoderatelyimmunosuppressed patients,witheach case beingindividuallyevaluated.8
With respect to anti-yellow fever vaccine, Mota et al. observedinanotherstudyconductedinourdepartment 52 patients with RAwho had received this vaccine. Ofthese, 12.8% had only mild adverse effects. There were no seri-ous reactions or deaths.12 Considering thatyellow fever is
endemicinagreatpartofBrazil,thevaccinationagainstthis diseaseisindicatedfortheresidentpopulationinan exten-sivepartofthenationalterritory(inadditiontotravellersto theseregions).However,thecurrentrecommendationisthat patientsundergoingimmunosuppressivetherapyshouldnot bevaccinatedagainstthisdisease.13
Thestudyshowedthatahighpercentageofpatientsinour earlyRAcohort,livinginanendemicareaforyellowfever,are vaccinatedregardlessofmedicaladvice.
It is essential for rheumatologists from endemic areas beingabletoinstructthepatientsaboutareas with recom-mendationofthevaccine,epidemicsandoutbreaks,aswell asevaluating theindividual riskofinfection anddegreeof immunosuppressionforeachpatient.
Althoughthisisthefirststudyevaluatingthevaccination statusofpatientswithearlyRA,ithassomelimitations.The study didnotevaluatethe vaccinationcard ofall patients, becausethecardhadbeenlostbyafewindividuals.Inthese cases, the recordof thevaccines may nothave been done reliably, due tothe patients’ memory bias. Thereasons by whichsomepatientsmissedoutimmunizationwerealsonot evaluated–suchasallergiesandpreviousvaccinereactions, evenwhentheywerebriefedbythedoctor.Theknowledgeof thesereasons wouldhelp ustooptimizethe patients’ vac-cination coverage. Another limitation was that we didnot assessseroconversion,seroprotectionandadversereactions fromvaccines.
After this study,our service is trying to offer guidance ontheappropriateuseofvaccines,androutinelyassessthe immunizationstatusofpatientswithearlyRA.Thishasbeen doneinformofachecklist,especiallypriortotreatmentwith DMDs.Ideally, thisassessmentshouldbemadenotonlyby rheumatologists in secondary/tertiary care healthservices, butalsoattheprimarylevelofhealthcare,bynon-specialist doctorsandnurses.
rheumatologist,buttothepatient’sspontaneousdemandfor thevaccine.
Thus,bothdoctorsandpatientsshouldbebetterinformed astothenecessityofvaccination,giventhatinfectionsarean importantcauseofmorbidityandmortalityinpatientswith RA.Inthisscenario,thedisseminationandimplementation oftherecommendations containedintheBrazilianSociety ofRheumatologyConsensus2012onVaccinationinPatients withRheumatoid Arthritismay be ofgreatimportance for improvingtheclinicalpracticeofrheumatologists.16
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgement
Ourspecialthankstotheresidentcolleagueswhohelpedus indatacollection:MelianeCardosoandGabrielaJardim.
r
e
f
e
r
e
n
c
e
s
1. MichaudK,WolfeF.Comorbitiesinrheumatoidarthritis.Best PractResClinRheumatol.2007;21:885–906.
2. DoranMF,CrowsonCS,PondGR,O’FallonWM,GabrielSE. Frequencyofinfectioninpatientswithrheumatoidarthritis comparedwithcontrols:apopulation-basedstudy.Artrhritis Rheum.2002;46:2287–93.
3. MutruO,LaaksoM,IsomakiH,KootaK.Tenyearmortality andcausesofdeathinpatientswithrheumatoidarthritis. BMJ.1985;290:1797–9.
4. PriorP,SymmonsDP,ScottDL,BrownR,HawkinsCF.Causeof deathinrheumatoidarthritis.BrJRheumatol.1984;23:92–9. 5. Myllykangas-LuosujarviR,AhoK,KautiainenH,IsomakiH. Shorteningoflifespanandcausesofexcessmortalityina population-basedseriesofsubjectswithrheumatoid arthritis.ClinExpRheumatol.1995;13:149–53.
6. ReillyPA,CoshJA,MaddisonPJ,RaskerJJ,SilmanAJ.Mortality andsurvivalinrheumatoidarthritis:a25-yearprospective studyof100patients.AnnRheumDis.1990;49:363–9. 7. ContiF,RezaiSoheila,ValesiniG.Vaccinationand
autoimmunerheumaticdiseases.AutoimmunityReviews. 2008;8:124–8.
8. VanAssenS,Agmon-LevinN,ElkayamO,CerveraR,Doran MF,DougadosM,etal.EULARrecommendationsfor
vaccinationinadultpatientswithautoimmuneinflammatory rheumaticdiseases.AnnRheumDis.2012;70:414–22.
9. FeuchtenbergerM,VollRE,KneitzC.Vaccinationsin Rheumatology.ZRheumatol.2010;69:803–12.
10.GluckT,Ladner-MullerU.VaccinationinPatientswith ChronicRheumaticorAutoimmuneDiseases.ClinInfectDis. 2008;46:1459–65.
11.AssenSV,BijlM.Immunizationofpatientwithautoimmune inflammatoryrheumaticdiseases(theEULAR
recommendations).Lupus.2012;21:162–7.
12.MotaLM,OliveiraAC,LimaRA,Santos-NetoLL,TauilPL. Vaccinationagainstyellowfeveramongpatientson immunosuppressorswithdiagnosesofrheumaticdiseases. RevSocBrasMedTrop.2009;42:23–7.
13.OliveiraACV,MotaLMH,Santos-NetoLL,TauilPL.Whata Rheumatologistneedstoknowaboutyellowfevervaccine. BrazJRheumatol.2013;53:206–10.
14.GluckT.Vaccinateyourimmunocompromisedpatients! Rheumatology.2006;45:9–10.
15.VisvanathanS,KeenanGF,BakerDG,LevinsonAI,WagnerCL. Responsetopneumococcalvaccineinpatientswithearly rheumatoidarthritisreceivinginfliximabplusmethotrexate ormethotrexatealone.JRheumatol.2007;34:952–7.
16.BrenolCV,MotaLMH,CruzBA,PereiraIA,FronzaLSR,Bertolo MB,etal.Consenso2012daSociedadeBrasileirade
Reumatologiasobrevacinac¸ãoempacientescomartrite reumatóide.RevBrasReumatol.2013;53:13–23.
17.MotaLMH,SantosNetoLL,PereiraIA,BurlingameR,Ménard HA,LaurindoIM.Autoantibodiesinearlyrheumatoid arthritis:Brasíliacohort:resultsofathree-yearserial analysis.RevBrasReumatol.2011;51:564–71.
18.MotaLMH,dosSantosNetoLL,BurlingameR,MénardHA, LaurindoIM.Laboratorycharacteristicsofacohortofpatients withearlyrheumatoidarthritis.RevBrasReumatol.
2010;50:375–88.
19.MotaLMH,LaurindoIM,dosSantosNetoLL.Prospective evaluationofthequalityoflifeinacohortofpatientswith earlyrheumatoidarthritis.RevBrasReumatol.
2010;50:249–61.
20.MotaLMH,LaurindoIM,dosSantosNetoLL.Demographic andclinicalcharacteristicsofacohortofpatientswithearly rheumatoidarthritis.RevBrasReumatol.2010;50:
235–48.
21.MinistériodaSaúde.SecretariadeVigilânciaemSaúde.In: DepartamentodeVigilânciaEpidemiológica.Manualdos centrosdereferênciaparaimunobiológicosespeciais.3.ed Brasília:MinistériodaSaúde;2006.
22.BridgesMJ,CoadyD,KellyCA,HamiltonJ,HeycockCR.Factors influencinguptakeofinfluenzavaccinationinpatientswith rheumatoidarthritis.AnnRheumDis.2003;62:685.
23.DoeS,PathareS,KellyCA,HeycockCR,BindingJ,HamiltonJ. Uptakeofinfluenzavaccinationinpatientson
immunosuppressantagentsforrheumatologicaldiseases:a follow-upauditoftheinfluenceofsecondarycare.
Rheumatology.2007;46:716–7.
24.SowdenE,MitchellWS.AnAuditofinfluenzaand
pneumococcalvaccinationinrheumatologyoutpatients.BMC MusculoskeletalDisorders.2007;8:58–62.
25.FeuchtenbergerM,KleinertS,SchwabS,RollP,ScharbatkeEC, OstemeierE.Vaccinationsurveyinpatientswithrheumatoid arthritis:acrosssectionalstudy.RheumatolInt.
2012;32:1533–9.
26.PradeepJ,WattsR,ClunieG.Auditontheuptakeofinfluenza andpneumococcalvaccinationinpatientswithrheumatoid arthritis.AnnRheumDis.2007;66:837–8.
27.FominI,CaspiD,LevyD,VarsanON,ShalevY,ParanD,etal. Vaccinationagainstinfluenzainrheumatoidarthritis:the effectofdiseasemodifyingdrugs,includingTNFalpha blockers.AnnRheumDis.2006;65:191–4.
28.DesaiSP,TurchinA,Szent-GyorgyiLE,WeinblattM,CoblynJ, SolomonDH,etal.Routinelymeasuringandreporting pneumococcalvaccinationamongimmunosupressed rheumatologyoutpatients:thefirststepinimprovingquality. Rheumatology.2011;50:366–72.
29.SilvaCA,TerreriMT,AikawaNE,CarvalhoJF,PileggiGC, FerrianiVP.Práticadevacinac¸ãoemcrianc¸ascomdoenc¸as reumáticas.RevBrasReumatol.2010;50:3513–61.
30.MinistériodaSaúde.SecretariadeVigilânciaemSaúde, ProgramaNacionaldeImunizac¸ões.InformeTécnico: CampanhaNacionaldeVacinac¸ãocontraaInfluenza. Brasília.2012.
32.RibeiroAC,GuedesLK,MoraesJC,SaadCG,AikawaNE,Calich AL,etal.ReducedseroprotectionafterpandemicH1N1 influenzaadjuvant-freevaccinationinpatientswith rheumatoidarthritis:implicationsforclinicalpractice.Ann RheumDis.2001;70:2144–7.