U
SE OF
CHLORAMPHENICOL AT SOCIAL
SECURITY HEALTH CARE CENTERS IN
BOGOTA, COLOMBIA1
Julio Gonz&z Mohd
I
NTRODUCTIONPrescribing any medication without an appropriate indication ex- poses the patient to needless risk of ad- verse reactions and toxic effects. In the case of antibiotics, the risk is increased for the patient and the community be- cause of the changes that take place in the patient’s normal microbial flora and the selection, emergence, and spread of microbial strains resistant to antibiotics.
For some years it has been rec- ommended that use of chloramphenicol be restricted basically to clinical manage- ment of typhoid fever and a very small number of other clinical situations. This is first because more liberal use tends to encourage emergence of chlorampheni- col-resistant strains (I), and second be- cause chloramphenicol can produce very serious complications-the most serious being bone marrow suppression and en- suing blood dyscrasias (aplastic anemia, hypoplastic anemia, thrombocytoperiia, and granulocytopenia developing weeks or months after oral therapy). The likeli- hood of such disorders developing and proving fatal in people receiving chlor- amphenicol is significant, despite ad- vances in immunology and bone marrow
’ This artide will also be published in Spanish in the Bo- letin de la Oficina Sanitak Pananzekana.
z Physician, Chief of the Quality Conuol Office, Social Security Institute, BogotB, Colombia.
transplants, there being roughly one fa- tality per 25,000 to 40,000 patients re- ceiving chloramphenicol (2-J).
In this regard it should be noted that the likelihood of selecting re- sistant Salmonella typhi strains through misuse or overuse of chloramphenicol is especially worrisome in countries such as Mexico where a number of drug-resistant typhoid fever epidemics have been re- corded; in countries such as Australia, India, and various Middle Eastern na- tions (G) where chloramphenicol-resis- tant S. typhi outbreaks have been en- countered; and in countries where no system for surveillance of delayed adverse reactions to medications (such as aplastic anemia- 7) has been established.
M
ATERIALSANDMETHODS
With this in mind, a survey was made of chloramphenicol use at 35 outpatient health care centers (CABS) of
known as the ISS FAR 15 Program-a daily listing of dispensed drugs classified by drug name and the name of the dis- pensing pharmacy-for the selected study period of 27 February through 9 March 1984. The records reviewed were those of the four ISS Regional Program
Units encompassing the 35 CABS of Cun- dinamarca Department and Bogota.
These records were examined to determine (a) the CABS prescribing sys- temic (oral) chloramphenicol during the study period and (b) the identifying number of each oral chloramphenicol prescription. These prescription numbers were used to obtain copies of associated medical forms, and the forms were used to obtain the following information: each patient’s name and social security membership number (identical to the number of the patient’s clinical history), the name of the attending physician, the medications prescribed in conjunction with chloramphenicol, the dosages pre- scribed and provided, the route of administration, and the treatment regimen.
To help check the accuracy of the automated data processing system, the data obtained on the prescribed medications and dosages were compared with data from another program (the ISS
FAR 12 Program) that records medica- tions dispensed by individual prescrip- tions issued by the CABS. The agreement of these data was found to be almost en- tirely satisfactory.
In addition, the patients’ clinical histories were obtained from the CAB records, and relevant information from these histories was recorded by a nurse and technician from the Cundina- mama-Bogota Quality Control Office,
both of whom participated actively in all phases of the study. In most cases the pa- tient’s social security membership num- ber sufficed for obtaining the clinical his- tory. Occasionally, however, errors in copying or reading the number made it necessary to go back to medical appoint- ment records or to second copies of the medical forms kept in CAB pharmacies; for these purposes it was found essential to have the names of the patient and physician as well as the date of the prescription.
RE
SULTSWhile oral chloramphenicol was found to have been prescribed in all four regional program units (UPZS), the prescription level in the southern unit was approximately 12 times greater than
in the central unit, seven times greater - than in the western unit, and three times s greater than in the northern unit. Fur- s thermore, most of these southern unit % prescriptions were issued by a single phy-
sician in the Girardot CAB, who alone ac- g
counted for 59 % of all the chloramphen- 2 kl icol prescriptions studied (the Girardot
CAB was serving about 1.3 % of all the
Social Security members served by the four units).
More generally, of the 35 CABS
involved, only 11 (3 1% ) prescribed
chloramphenicol during the 27 Febru-
ary-9 March 1984 study period, and only 20 of the approximately 297 physicians attached to these 11 CABS did so. In all, the physicians prescribing chlorampheni- co1 during the study period were only 6.7 % of these attached to the 35 CABS.
Table 1 shows the number of 3 ‘8 chloramphenicol prescriptions filled, by
UPZ and CAB, the number of CABS in each UPZ, the number of physicians in each CAB issuing chloramphenicol pre-
8
TABLE 1. Oral chloramphenicol prescriptions issued at the 35 social securii health centers (CABS) and filled during the 27 February-9 March 1984 study period. The 11 CABS in the Cundinamarca-Bog& study area that issued these prescriptions am listed by name. The table also shows the number of physicians associated with each center and the number of physicians who issued the chloramphenicol prescriptions.
No. of
Basic health centers No. of No. of physicians Total no. of prescribing chlorarnphenicol physicians prescribing health centers chloramphenicol prescriptions at center chlorarnphenicol in each UPZ Northern unit (UPZ):
Chia 10 3 1
ZipaquirA 5 7 2
Cajiti 3 1 1 11
Norte 3 20 2
1 Southern unit (UPZ):
Girardot 60 17 1
Fuss 2 1
Quiroga ; 12 2 IO
Tunjueliio 1 18 1
1 Central unit (UPZ):
Central 2 107
CS? 9. 3 13
: I 3 Western unit (UPZ):
Paiba 9 97 6 11
Total 101 297 20 35
scriptions, and the number of physicians doing the prescribing.
Table 2 shows the number of medical prescriptions filled during the study period in each UPZ, the number
filled for systemic antibiotics other than chloramphenicol, and the number filled for chloramphenicol. Roughly one in every six outpatients received a systemic antibiotic, a ratio consistent with the results of a separate study (8) by the Cun- dinamarca-Bog06 Quality Control Of- fice on the appropriateness of antibiotic use.
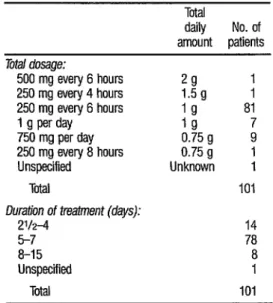
Table 3 summarizes data on daily dosages of chloramphenicol and the duration of treatment. The average duration of prescribed treatment was 5.1 days, while the mode (for 72 patients) was five days. At least 98 of the 101 pa- tients received one gram per day or less.
As indicated in Table 4, nearly all (91 of the 101 patients) were pre- scribed some other drug together with the chloramphenicol. Phenylbutazone, prescribed for 15 patients, has a strong association (second only to chloramphen- icol’s) with cases of aplastic anemia; it has also been associated (together with other drugs of the pyrazolone type such as di- pyrone and griseofulvin) with granulocy- topenia. Other combinations of chlor- amphenicol with antimicrobials should also be noted, the most frequent combi- nation of this kind being with sulfa- trimethoprim.3 Other combinations
TABLE 3. Oral chloramphenicol dosages and treatment durations specified on the 101 prescriptions studied.
Total
daily No. of amount patients Total dosage:
500 mg every 6 hours 29
250 mg every 4 hours 1.5 g ; 250 mg every 6 hours lg 81 1 g per day ICI
750 mg per day 0.75 g ; 250 mg every 8 hours 0.75 g 1 Unspecified Unknown 1
Total 101
Duration of treatment (days):
2V2-4 14
5-7 78
8-15 8
Unspecified 1
Total 101
0
TABLE 4. Drugs prescribed for administration in 2 _ conjunction with the oral chloramphenicol prescribed
during the study period in Cundinamarca-Bog&. E s No. of
Drugs prescribed patient9 E Antispasmodic and antidiarrheal 5
medications 32 2
Metronidazole and/or mebendazole 19 a Phenylbutazone 15
Trimethoprim-sulfamethoxazole 13 2
Antibiotics 7 2
G&of&in 4 %
Oral hypoglycemics 1 2
a It should be noted that wne patients were prescribed two or more drugs 2 in addtion to ati chloramphenicol. 0
8 .
worth noting because they are known ca- pable of producing adverse interactions * 2 are those of chloramphenicol with ampi- s cillin (prescribed for one patient) and chloramphenicol with aminoglycocides
3
(prescribed for three patients). Chloram- 2 phenicol was also commonly prescribed 3 in combination with the antiparasitic
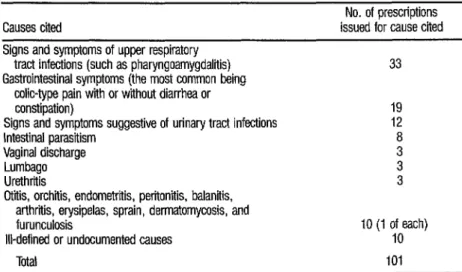
The reasons for prescribing chloramphenicol could not always be as- certained precisely, owing partly to in- complete data and partly to a fairly com- mon lack of correlation between the problem that prompted the consultation and the diagnosis set down in the clinical history. A summary of the reasons given is presented in Table 5. In addition to the data in the table, it should be mentioned that oral chloramphenicol may have been prescribed for halitosis, for a “bad taste” in the mouth, for general malaise, for pain in the midsection, and for loss of memory. It should also be noted that in- testinal parasitism and flu-like states were explicitly cited as reasons for pre- scribing the drug.
There was only one instance in which an attempt was made to test out a possible diagnosis of typhoid fever. (This was done by the Vidal test, which is now considered to have little diagnostic value--l-Q. However, suspicion of this possible diagnosis was not cited in any clinical history. No picture involving fe- ver was documented except in regard to
one patient with a possible urinary tract
infection, nor were any data obtained that would tend to confirm or deny the existence of adenopathy or splenome- galy. Also, oral chloramphenicol was pre- scribed for one patient six and a half months pregnant and for a diabetic pa- tient receiving oral hypoglycemics; but no data justifying these prescriptions were entered in either patient’s clinical history.
Finally, it is important to note that, despite marked deficiencies in the content of the clinical histories, these his- tories showed that at least five of the 101 patients involved had been treated with oral chloramphenicol in the previous year and that some patients had previ- ously received repeated treatments with phenylbutazone.
TABLE 5. Medical causes cited for issuing the 101 oral chloramphenicol prescriptions studied.
Causes cited
Signs and symptoms of upper respiratory tract infections (such as pharyngoamygdaliiis) Gastrointestinal symptoms (the most common being
colic-type pain with or without diarrhea or constipation)
Signs and symptoms suggestive of urinary tract infections Intestinal parasitism
Vaginal discharge Lumbago Urethritis
Gtiiis, orchiiis, endometriiis, peritonitis, balanitis, arthriiis, erysipelas, sprain, dermatomycosis, and furunculosis
Ill-defined or undocumented causes Ttial
No. of prescriptions issued for cause cited
33
19 12 i 3 3
D
ISCUSSIONAlthough the number of phy- sicians found by this study to have inap- propriately prescribed cbloramphenicol was relatively small, the overall pattern of chlorarnphenicol misuse is a matter of
concern. Apart from the drug’s occasion- ally fatal side-effects, its potential for en- couraging selection and spread of resis- tant microbes in the community is
important. In this latter way, misuse of
chlorarnphenicol places at risk not only the patients who receive it but also the entire community, which is powerless to
do anything about emergence of resis-
tant strains. ‘Ibis risk only becomes evi- dent when life-threatening commu-
nicable disease pictures treated with chloramphenicol fail to respond to treat- ment. Such failures have been reported, among other things in regard to a case of infection with gram-negative bacteria in Mexico (1) and in cases elsewhere of meningitis caused by hemophilus strains resistant to both ampicillin and chloram- phenicol (9). Endemic resistance to chloramphenicol (5, 10) has also been
described, particularly in strains of He& sidh, Escheriha coZi, Neisseha gonor- rhoeae, and Proteus rettgeri (11).
Our conclusion that the cblor-
amphenicol use observed in this study was improper is based on the following findings:
1 Only two patients had suffi- ciently documented medical conditions justi- fying the choice of chloramphenicol. These were a case of peritonitis and a case of endo- metritis that could have been caused by an- aerobic gram-negative bacteria. In the other 98 % of the cases for which it was prescribed, chloramphenicol was not really indicated.
2 The standing recommenda- tion to restrict use of chloramphenicol to the clinical management of typhoid fever was not followed. In general, clinical evidence pro-
viding a basis for suspecting typhoid fever- such as the cases of fever emerging during ep- idemics of this disease in Colombia (I, G, 12) and other countries @)-was altogether lacking.
3 The contraindication against using chloramphenicol in cases of pharyngo- amygdalitis-type infections of the upper res-
piratory tract was disregarded, and the drug was in fact prescribed for use against such in- fections in 32 patients.
4 The recommendation not to use chloramphenicol when potentially less toxic therapeutic agents are equally effective was not followed.
5 The recommendation that chloramphenicol be avoided as much as pos- sible was ignored in some cases.
6 Contrary to the existing rec- ommendations, chloramphenicol was used simultaneously with drugs of the butazone family. These latter drugs cause something on the order of a tenfold increase in the risk of aplastic anemia (14). Phenylbutazone (a member of this group) accounts for some 19% of all drug-induced aplastic anemias PA
7 Again contrary to what is rec- ommended, chloramphenicol was also pre- scribed in combination with drugs (such as phenylbutazone, dipyrone, and griseofulvin) that, depending on the treatment regimen, can depress bone marrow function.
8 Chloramphenicol was pre- scribed for use during pregnancy despite evi- dence that it crosses the placental barrier and that the fetal liver lacks the capacity to me- tabolize it (15).
9 Chloramphenicol was pre- scribed in conjunction with oral hypoglyce- mics, contrary to advice that the latter be temporarily discontinued in order to avoid reducing their clearance by 50 % or more and
thereby risking drug-induced hypoglycemia.
10 The decision to use chlor- amphenicol in conjunction with other anti- microbials does not appear to have had a sound medical basis, but instead seems to have depended on whim or chance. More- over, in prescribing these combinations it ap- pears that little or no consideration was given to the established antagonism (both in vitro and in vivo) between chloramphenicol and gentamicin, as well as between chloramphen- icol and ampicillin (2).
11 There is no technical argu- ment that justifies using chloramphenicol to cope with problems such as flu-like condi- tions or parasitism, upon which it has no
beneficial effect whatever.
All of this indicates, among other things, that a proper medical sense of social responsibility, one that bases the decision to use antibiotics such as chlor- amphenicol on more rigorous and scien- tific grounds, needs to be encouraged (1G). Despite its potentially very serious side-effects, chloramphenicol is an effec- tive antibiotic that is invaluable for deal- ing with certain life-threatening condi- tions. Therefore, its effectiveness needs to be protected by avoiding the sort of excessive use and misuse found at 11 of the 35 Cundinamarca-Bogota health care centers. In this regard, it should be noted that only 6.7% of the 297 physi- cians working at these 11 centers (see Ta- ble 1) were issuing these prescriptions, a finding suggesting that the improper use
2 of chloramphenicol could be eliminated 2 or greatly reduced through effective edu-
- 52
cation, motivation, and supervision. At the same time, attention G
.g should be paid to the chloramphenicol P) regimens being prescribed, because in 3 general the prescribed regimens exam- 2 ined in our study were subtherapeutic. 3 A,
118
That is, the duration of treatment was in- variably much shorter than that indi-
cated for most purposes-such as the 20
days recommended for the clinical man- agement of typhoid fever; and the daily dosage was generally below the recom- mended dosage of 50 mg I kg/ day (2.5 g per day for a 50 kg patient) divided into equal amounts taken once every six hours. As ‘&ble 3 shows, by far the most common dosage prescribed was 1 g daily (20 mgl kg for a 50 kg patient), which at about two-fifths of the usually recom- mended level (2, 3, 15, 17) would seem too low for efficacious treatment. It seems likely that the across-the-board medical decision to prescribe “a little for a short time” arose from a very imperfect understanding of dosage-specific versus dosage-unspecific side-effects, and, above all, of the tendency of subtherapeutic doses to promote bacterial resistance.
A
CKNBWLEDGMEN’I’SWe are grateful to Rosa de Montenegro and Gustav0 Mora of the staff of the Cundinamarca-Bogota Medi- cal Care Quality Control Office for their key collaboration at all stages of the study, and also to Mrs. Nelly de Cardozo, secretary of the office.
S
UMMARYChloramphenicol is currently recommended for use only in treating acute typhoid fever and a very small number of other clinical conditions- partly because it can precipitate rare but potentially fatal side-effects and partly because its overuse encourages microbial resistance.
use at 35 of Colombia’s outpatient health care centers pertaining to the So- cial Security Institute in the city of Bo- gota and the surrounding department of Cundinamarca. The survey found that chloramphenicol was prescribed for 101
patients by 20 physicians at 11 of the 35
centers during the 27 February-9 March 1984 study period. In most (91) cases,
one or more other drugs were prescribed together with the chloramphenicol.
The survey also found that use of chloramphenicol was justified in only two cases-a case of peritonitis and a case of endometritis that could have been caused by anaerobic, gram-negative bac- teria. In all other cases it was unjustified, and in certain cases-those of a pregnant woman, a diabetic continued on hypo- glycemic drugs, and 32 patients with pharyngoamygdalitis-type infections of the upper respiratory tract-it was obvi- ously contraindicated. Chloramphenicol was commonly prescribed in combina- tion with other drugs capable of aggra- vating its adverse side-effects. However, in most cases the chloramphenicol regi- mens prescribed appeared too low to have much therapeutic worth.
All of this suggests that a bet- ter medical understanding of chloram- phenicol and other antibiotics-together with a proper medical sense of social re- sponsibility-needs to be encouraged. However, a relatively small number of physicians (6.7% of the 297 working at the 11 centers) issued all the pre- scriptions for chloramphenicol during the study period, a fact suggesting that the misuse and overuse of chlorampheni-
co1 could be eliminated or greatly re- duced through effective education, mo- tivation , and supervision.
RE
FERENCES1 Guzm?i.n, M. Fiebre tifoidea: AIgunos aspectos novedosos. Colombia M&&a 13(4): 151-154,
1982.
2 Robertson, D., and C. Smith. Mamzdof Chz- icaf Pharmacology. Williams and WiIkins, BaI- timore and London, 1981, pp. 25-29. Goodman, A., L. Goodman, and A. Gilman.
Las &aJeJ farmaco&$2z.r de l’a terapt%tica (sev-
enth ed.). Editorial Panamericana, Buenos Ai- res, 1986, pp. 1124-1129.
American Medical Association. AMA Dwg Evalrcations (fifth ed.). Chicago, 1980, pp. 1282-1284.
Peterson, P. K., and J. Verhoef (eds.). The An- timicrobzld Agents Annaal (vol. 1). EIsevier Science Publishers Bureau, Amsterdam, 1986,
pp. 91-96.
Smith, S. H., P. E. PaIumbo, and P. J. Edelson. Saknonella strains resistant to multi- ple antibiotics: therapeutic implications. Pe- diatr Infect Dir 3:45 5.
Silver, B., and K. Suckerman. Aplastic ane- mia. Mea’ Ch North Am 64:601-622, 1980. Gonzaez, J. Racionahdad de la formulation de Lincosaminas. Acta Mt%ica Colombiana 9:139-145, 1984.
Simsathien, S., C. Duangmari, and I? Echeverrla. Haemophihs infZuenzae type B re- sistant to ampiciIIii and chloramphenicol in an orphanage in Thailand. Lancet 2:1214- 1217, 1980.
10 Ward, J. I., T. F. Tsai, G. A. Felice, and D. W. Fraser. Prevalence of ampicillin and chloram- phenicol-resistant strains of HaemophLh in- j?uenzae causing meningitis and bacteremia. J Infect Dir 138:421-424, 1978.
11 Grieco, M. Resistencia a 10s antibikicos. C&zi- cas M&&as de NotieamZrica. Interamericana, Mexico City, 1982, pp. 25-38.
13 Goffman, T, C. Ruiz, and G. Counts. Water- borne tvnhoid fever in Dade Countv. Florida: Clinicai&d therapeutic evaluation of 105 bac- teremic patients. Am J Med 59:481-487, 1975.
14 The International Agranulocytosis and Aplas- tic Anemia Study. Risks of agranulocytosis and aplastic anemia. JAMA 256(3):1750-1757, 1986.
15
16
17
Ambrose, P. J. Clinical pharmacokinetics of chloramohenicol. ChicaL Pharmacohinetics 9:222, 1584.
Participants in Conference on Molecular Biol- ogy, Pathogenicity and Ecology of Plasmids; Santo Domin o, Dominican Republic. Decla- ration on wor d misuse of antibrotics. Biomi- P &a 1(4):226-228, 1981.
Kauffman, R. E., J. N. Mice& L. Strebel, J. A. Bucklev. A. K. Done. and A. S. Daiani. Phar- macok&etics of chldramphenicol and chlor- amphenicol succinate in infants and children. J Pediatr 98:315-320, 1981.