rev bras hematol hemoter. 2015;37(4):259–262
w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Case
Report
Limitations
of
performance
status
assessment
in
elderly
with
acute
myeloid
leukemia
Ana
Lúcia
Ippolito
Carbonell
∗,
Maria
de
Lourdes
Chauffaille
UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received23October2014 Accepted25December2014 Availableonline14April2015
Introduction
Elderlypatientspresentclinicalandfunctionalheterogeneity. Thusthechronologicalage(60yearsandolder)alonedoesnot characterizethisgroupofindividualscorrectly.Performance statusscalessuchastheKarnofskyPerformanceScale(KPS)1 or EasternCooperative Oncologic Group Scale(ECOG),2 are usedbyhematologistsindecisionmakingforelderlypatients withcancer. Good performance statusis defined asa KPS equaltoorgreaterthan80%oranECOGlessthan2.These scoresareoneofthecriteriautilizedtochoosethetreatment strategy for elderly patients with acute myeloid leukemia (AML). AMLis morefrequentin the aged. Consideringthe highriskoftoxicityduringAMLtreatmentinelderlypatients, manyresearchershaverecommendedtheapplicationof geri-atricinstruments atbaselineand inthefollowup ofthese individuals. The objective of this paper is to improve the understandingofhowgeriatricapproachesmay benefitthe performancestatusassessmentofelderlypatientswithAML.
∗ Correspondingauthorat:RuaDiogodeFaria,824,04034-000SãoPaulo,SP,Brazil. E-mailaddress:[email protected](A.L.I.Carbonell).
Twocases,asclinicalchallenges,areusedtoexemplifythis clinicalcontext.
Clinical
challenges
Case1–Patient1:75-year-oldmanwithdenovoAML,normal karyotype,KPSof90%andECOGof1
Case2– Patient 2:65-year-old womanwithde novo AML, normalkaryotype,KPSof80%andECOGof1
Question:Howdogeriatricinstrumentsimprovethe char-acterizationofthesepatients?(Table1).
Brief
considerations
about
performance
status
and
functional
status
Performancestatus–assessedbyKPSand/orbyECOG(Table2) – is the traditional method applied by hematologists to
http://dx.doi.org/10.1016/j.bjhh.2015.03.007
260
revbrashematolhemoter.2015;37(4):259–262Table1–Hematologicdataofclinicalchallengepatients.
Patient1 Patient2
Age(years) 75 65
Gender Male Female
Diagnosis DenovoAML DenovoAML Marrowblasts(%) 38 47
Hemoglobin(g/dL) 10.7 8.9 Whitebloodcellcount(×103/L) 3400 2870
Plateletcount(×103/L) 92 50
AML:acutemyeloidleukemia.
evaluatethedisease/treatmentimpactontheelderlypatient’s abilitytocareforthemselvesandtowork.
Theseinstruments are notbasedon asystematic
ques-tionnaire. The scores are obtained based on a general
impression of the clinician about the patient’s symptoms
and the patient’s autonomy to care for themself and to
work.Onedisadvantageofthis methodisthe lackof defi-nitionstospecificallycharacterize thescorelevels ofthese scales.3
Functionalstatusisthelevelofautonomythatan individ-ualhasindailyactivities.TheActivityDailyLivingScale(ADL)4 and InstrumentalActivity OfDaily Living Scale(IADL)5 are complementarytoolswidelyvalidatedtomeasurefunctional status.
ADLwasvalidatedbyKatzinchronicallyillpatientsandis composedofsixquestionsaboutspecificanduniversaltasks.4 IADLwasdelineatedbyLawtonandisascalewithnine ques-tionswiththreepossibleanswers:able,ablewithhelpand
unable.Itreferstotheautonomyinactivitiesthataremore influencedbyculturalcontext(Table2).
In1995,Moretal.6evaluatedthevalidityofKPSbyshowing theautonomyindailylivingactivitiesforeachKPSassessed in685patientswithadvancedcanceronapplyingtheKPSand ADL.Theyshowedthattheautonomyofthesepatientswas lowerastheirKPSscoredecreased.
KPS,ECOG,ADLandIADLrefertothesameconstruct,i.e., tothesameabstracttheoreticalconcept.DifferenttoKPSand ECOG,ADLandIADLemployasequenceofspecificquestions. Thepossibleanswerstoeachquestionaregraduatedintwo (ableorunable)orinthree(able,ablewithhelp,andunable) levels.Theseinstrumentshighlightimprovementsor impair-mentsinfunctionalityduringthefollowupofthepatient.
AsshowninTable2,thecorrelationbetweenthesescores suggests thatpatientswithpoorKPShavelosttheir auton-omyintheIADL5andareatriskofdependenceinbasicADL.4 However,individualswithgoodKPSprobablyhavepreserved autonomyintheADLdimensionbutmayevolvewithsome IADLdependence.
LoosingautonomyinADLandhavingpoorscoresinKPS (≤80%)orECOG(>1)areofprognosticvalue.3,7
However,despitetheprognosticvalueofperformance sta-tus,elderlypatientswithgoodKPScouldbeathighriskto succumb duringtheinductionphaseofAMLtreatmentfor reasons notrelated tothe disease.This eventhasjustified someresearcherstoapplyinggeriatricapproachesinelderly patientswithAML.Thegoldstandardmethodforevaluating olderpatientsisComprehensiveGeriatricAssessment(CGA). CGAisamultidisciplinaryandtime-consumingapproach that includes functional, cognitive, psychological status, comorbidity, nutritional, polypharmacy and social support
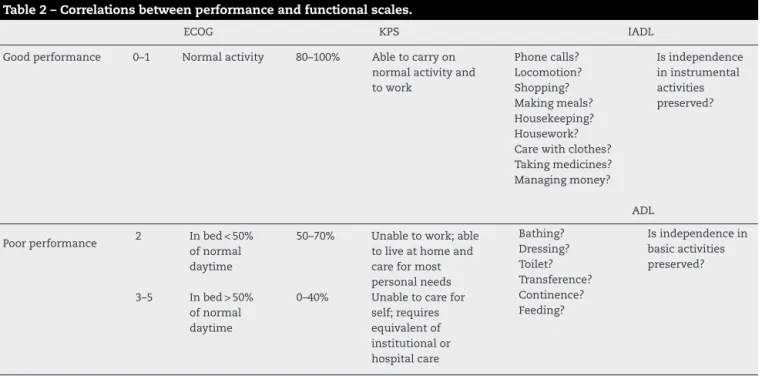
Table2–Correlationsbetweenperformanceandfunctionalscales.
ECOG KPS IADL
Goodperformance 0–1 Normalactivity 80–100% Abletocarryon normalactivityand towork Phonecalls? Locomotion? Shopping? Makingmeals? Housekeeping? Housework? Carewithclothes? Takingmedicines? Managingmoney? Isindependence ininstrumental activities preserved? ADL
Poorperformance 2 Inbed<50% ofnormal daytime
50–70% Unabletowork;able toliveathomeand careformost personalneeds Bathing? Dressing? Toilet? Transference? Continence? Feeding?
Isindependencein basicactivities preserved?
3–5 Inbed>50% ofnormal daytime
0–40% Unabletocarefor self;requires equivalentof institutionalor hospitalcare
KPS:Karnofskyperformancescale;ECOG:EasternCooperativeOncologyGroupscale;IADL:instrumentalactivitiesofdailyliving;ADL:basic activitiesofdailyliving;Goodperformance:KPS≥80%andECOG<2;Independence:nodependenceinADLandIADL;Dependence:needhelp
revbrashematolhemoter.2015;37(4):259–262
261
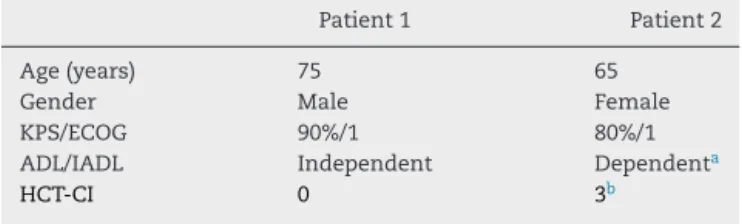
Table3–Functionalassessmentandcomorbidityscores ofclinicalchallengepatients.
Patient1 Patient2
Age(years) 75 65
Gender Male Female
KPS/ECOG 90%/1 80%/1 ADL/IADL Independent Dependenta
HCT-CI 0 3b
KPS: Karnofsky performance scale; ECOG: eastern cooperative oncologic group scale; ADL: activities of daily living scale; IADL:instrumental activities ofdaily livingscale;Independent: no dependence in daily activities; HCT-CI: hematopoietic cell transplantation-comorbidityindex.
a Patient2neededhelptotakemedications/locomotionandshe
hadurinaryincontinence.
b Patient2hadinsulin-dependentdiabetesmellitusandserum
cre-atinineequalto2.6mg/dL.
assessments.Overthelast20 years,CGAhasbeen applied intheoncogeriatricfieldandhasaggregatedimportantdata forthetherapeuticmanagementofthisgroupofindividuals. ItisnotablethattheADLandIADLaretoolswidelyusedfor thefunctionalstatusassessmentincludedinCGA.8
In2006,Weddingetal.9demonstratedthebenefitofadding theIADLtotheKPSinthefunctionalassessmentofelderly patientswithAML.Sincethen,severalotherresearchershave studied the impact of geriatric parameters in the survival andthe qualityoflifeofolderpatientswithhematological malignancies.10
Agingisassociatedwithahighincidenceofcomorbidities thathaveasignificantimpactonsurvivalandon complica-tionsoftreatment.11 Comorbiditiesaremorbidentitiesthat havealreadybeendiagnosedatthetimeofthediagnosisof theindexdisease,hereAML,orthatarediagnosedduringthe patientfollowup.
Extermannet al.11 studiedthe toolsused for comorbid-ityscoringinelderlypatientswithcancer.Theyshowedthat comorbidity scores increase with advancing age and that thesescoresarecorrelatedwithmortalitybutnotassociated tofunctionalstatus.11 Inconclusion,comorbidityand func-tionalityareindependentvariablesandshouldbemeasured separatelyinolderpatientswithcancer.
Recently,hematologistsdevelopeddiseasespecific instru-mentsthatmeasurethe impactofcomorbiditiesonelderly individualswithAML,myelodysplasticsyndromesandthose submittedto hematopoieticstem cell transplantation. Sor-roretal.developedtheHematopoieticCell Transplantation ComorbidityIndex (HCT-CI)12 which hasalready been vali-datedinpatientswithAML.
Whathappenedtothepatient’sassessmentwiththe aggre-gationofsomegeriatricscales? Table3showstheresultof functionalandcomorbidityassessmentofthetworeported cases.
Clinical
challenges
follow-up
Patient1wassubmittedtothestandardtreatmentwithfull dosesoftheAMLinductionprotocol andoneconsolidation
phase.Afterconsolidation,heevolvedwithsepsisand pro-longedneutropenicperiod.Sixmonthsafterthediagnosisof AML,hewasaliveandwithoutevidenceofdisease.
Patient2wassubmittedtoexclusivepalliativecare, accord-ingtoherandherfamily’swishesandconsideringtheimpact ofhercomorbidity scoreand herdependence accordingto ADL/IADL.ShediedofAMLfourmonthsafterdiagnosis.
Consideringthesetwopatients,bothwithgoodKPS,Patient 1 wasten years older than Patient 2. Despite this,he had greaterautonomyandalowercomorbidityscorethat delin-eated aclinical context more favorableto AML treatment. Moreover,theaggregationofgeriatrictoolsaddedinformation aboutPatient2thatidentifiedherfunctionaland comorbidity-relatedrisks.Theseinstrumentsprovidedspecificinformation forthemanagementofherfinalphaseoflife.
Inconclusion,ADLand IADLimprovedthesensitivityof the functional assessment of these elderly patients. They added importantinformationaboutPatient 2thatchanged herperformancescorefrom‘good’to‘goodbutdependent’. Furthermore,theHCT-CIscorepredictedtheimpactof comor-bidities onhersurvival.TheapplicationsofADL,IADLand HCT-CIimprovetheassessmentofelderlypatientswith hema-tologicalmalignances.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.KarnofskyDAA,CraverWH,BurchenalLFJH.Theuseofthe nitrogenmustardsinthepalliativetreatmentofcarcinoma– withparticularreferencetoBronchogeniccarcinoma.Cancer. 1948;1(4):634–56.
2.OkenMM,CreechRH,TormeyDC,HortonJ,DavisTE, McFaddenET,etal.Toxicityandresponsecriteriaofthe EasternCooperativeOncologyGroup.AmJClinOncol. 1982;5(6):649–55.
3.GarmanKS,CohenHJ.Functionalstatusandtheelderly cancerpatient.CritRevOncolHematol.2002;43(3):191–208. 4.KatzS,FordAB,MoskowitzRW,JacksonBA,JaffeMW.Studies
ofillnessintheagedtheindexofADL:astandardized measureofbiologicalandpsychosocialfunction.JAMA. 1963;185(12):914–9.
5.LawtonMP,BrodyEM.Assessmentofolderpeople: self-maintainingandinstrumentalactivitiesofdailyliving. Gerontologist.1969;9(3):179–86.
6.MorV,LaliberteL,MorrisJN,WiemannM.TheKarnofsky PerformanceStatusScale.Anexaminationofitsreliability andvalidityinaresearchsetting.Cancer.1984;53(9):2002–7. 7.YatesJW,ChalmerB,McKegneyFP.Evaluationofpatients
withadvancedcancerusingtheKarnofskyperformance status.Cancer.1980;45(8):2220–4.
8.ExtermannM,HurriaA.Comprehensivegeriatricassessment forolderpatientswithcancer.JClinOncol.
2007;25(14):1824–31.
262
revbrashematolhemoter.2015;37(4):259–26210.HamakerME,PrinsMC,StauderR.Therelevanceofageriatric assessmentforelderlypatientswithahaematological malignancy–asystematicreview.LeukRes.2014;38(3):275–83. 11.ExtermannM,OvercashJ,LymanGH,ParrJ,BalducciL.
Comorbidityandfunctionalstatusareindependentinolder cancerpatients.JClinOncol.1998;16(4):1582–7.