Letters to the Editor
Radiol Bras. 2015 Mar/Abr;48(2):126–130
128
Ernesto Lima Araujo Melo1, Francisco Thiago Martins de Paula1, Rainne André Siqueira1, Sariane Coelho Ribeiro2
1. Universidade Estadual do Ceará (UECE), Fortaleza, CE, Brasil. 2. Hospital Israelita Albert Einstein, São Paulo, SP, Brazil. Mailing Address: Dr. Ernesto Lima Araujo Melo. Universidade Estadual do Ceará, Centro de Ciências da Saúde – Curso de Medicina. Avenida Paranjana, 1700, Campus do Itaperi. Fortaleza, CE, Brasil, 60740-000. E-mail: ernesto. melo@uece.br.
http://dx.doi.org/10.1590/0100-3984.2014.0073
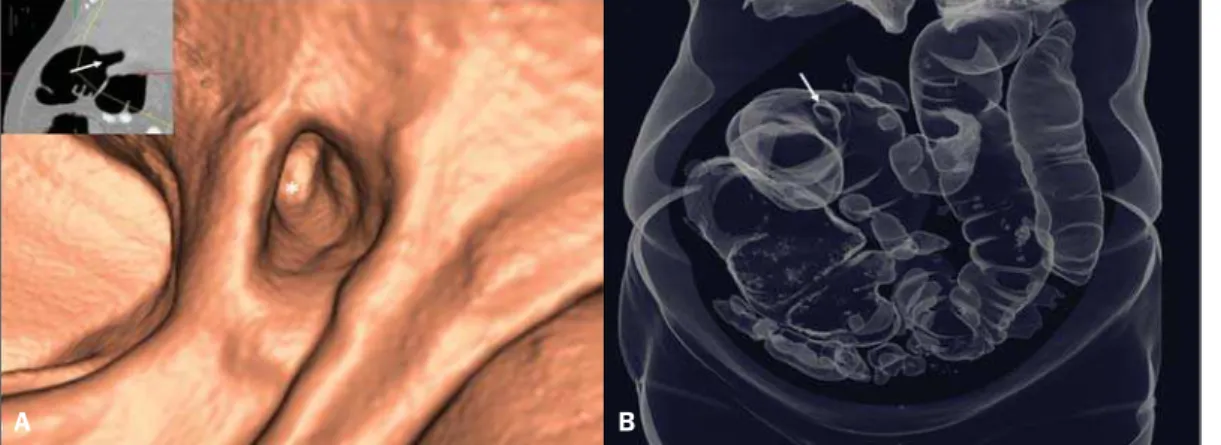
causing abdominal distension upstream due to fecal buildup (Fig-ure 1B). Endoluminal reconstruction of virtual colonoscopy im-ages demonstrated the fistulous orifice in the transverse colon (Figure 2A). Tridimensional reconstruction for gaseous material demonstrated diffuse gaseous distension of the right, transverse and left colons, and also the site of the choledochal-colonic fistula (Figure 2B). Once the diagnosis was established, the patient was successfully submitted to surgery.
Acute obstructive cholecystitis may approach the serosas of the biliary and intestinal tracts due to the gallbladder and/or com-mon biliary duct dilatation. With the repetition of inflammatory episodes and adherence of the serosas, choledochal-colonic fistularization may occur, allowing for the passage of biliary cal-culi into the intestinal lumen(1), besides calculi impaction at some
point in the tract, causing significant pain, severe local irritation, edema or gangrene(2). Amongst cholecystointestinal fistulas,
cholecystoduodenal fistulas represent more than 70%, while cholecystocolonic fistulas represent 8% to 26% of them(3). Rigler
et al. established four criteria (presence of air or contrast medium in the biliary tract; direct or indirect identification of calculus in the bowel; alteration in the position of a previously identified cal-culus; radiological signs of either partial or total occlusion of the intestinal lumen) which corroborate a diagnosis of bowel obstruc-tion caused by a calculus(4). Three findings determined by such
criteria constitute the Rigler’s triad: signs of small bowel dilation, pneumobilia and ectopic calculi.
Despite the rarity of this condition, one should be attentive to the possibility of biliary colon in acute onset of lower intestinal obstruction, in order to allow for a prompt and correct diagnosis and institution of an appropriate treatment.
REFERENCES
1. Wang JK, Foster SM, Wolff BG. Incidental gallstone. Perm J. 2009;13: 50–4.
2. Costi R, Randone B, Violi V, et al. Cholecystocolonic fistula: facts and myths. A review of the 231 published cases. J Hepato Biliary Pancreat Surg. 2009;16:8–18.
3. Del Gaizo A, Raval B. Cholecystocolonic fistula. Applied Radiology. 2006; 35:21–2.
4. Smyth J, Dasari BV, Hannon R. Biliary-colonic fistula. Clin Gastroenterol Hepatol. 2011;9:A26.
Catamenial pneumothorax
Pneumotórax catamenial
Dear Editor,
A previously healthy 29-year-old woman presented at the emergency service complaining of sudden onset dyspnea. At physi-cal examination the vesicular murmur was absent in the entire right hemithorax. Chest radiography demonstrated the presence of pneumothorax at right (Figure 1) and chest computed tomog-raphy (CT) did not demonstrate any other alteration besides the already mentioned pneumothorax. Thoracotomy with underwa-ter seal chest drainage was performed. As the pneumothorax pre-sentation coincided with the patient’s menstrual period, pelvic ultrasonography was performed and identified an image compat-ible with endometrioma in the left ovary. In three months, the patient evolved with a new spontaneous pneumothorax at right, and a pig-tail drainage tube was inserted. Later, thoracocoscopy was performed, and endometriotic foci were identified and resected (Figure 2). The chest wall was repaired with a Marlex mesh. After three months, the patient remains asymptomatic.
Figure 2. A: Endoluminal 3D reconstruction of virtual colono-scopy image demonstrating the fistulous orifice (asterisk) in the large bowel. The reference 2D image of the orifice positioning is highlighted (arrow). B: 3D re-construction demonstrating gaseous bowel distention and the fistulous orifice (arrow).
A B
Letters to the Editor
Radiol Bras. 2015 Mar/Abr;48(2):126–130
129
Imaging evaluation of the chest has been subject of a range of recent publications in the Brazilian radiological literature(1–10).
Thoracic endometriosis is the presence of endometrial tis-sue in the lung parenchyma or in the pleural cavity, and mani-fests clinically by hemoptysis, pneumothorax or hemothorax, oc-curring in conjunction with menstrual periods(11–13). Frequently,
it affects women in childbearing age, with incidence peak between the third and fourth decades of life(14). Thoracic endometrial
im-plants generally occur in the pleural cavity and, less frequently, in the lung parenchyma(14).
Pleural endometriosis is an entity whose course is generally benign, occurring most frequently at right, possibly due to con-genital defects in the right diaphragmatic dome and to continu-ous flow of fluid from the pelvis into the right upper quadrant of the abdomen(15). Typically, thoracic endometrial implants occur
concurrently with periodical symptoms (from one day before to the first two days of menstruation)(16). The clinical presentation
depends on the site of involvement, namely, catamenial pneu-mothorax or hepneu-mothorax in cases of pleural implants; and cata-menial hemoptysis or asymptomatic pulmonary nodules in cases of implants in the pulmonary parenchyma. Histologically, the pres-ence of endometrial tissue is identified in the lungs and/or pleura. Cytology reveals the presence of endometrial cells in the pleural fluid, in pulmonary nodules/masses aspirates, or in bronchial lav-age fluid. Imaging studies include principally chest radiography and CT, which can demonstrate pneumothorax, hydropneu-mothorax or pleural nodular lesions. Magnetic resonance imag-ing has increasimag-ingly gained relevance since, besides differentiat-ing parenchymal from pleural lesions, this method presents a better spatial resolution and, if performed during the menstrual period, it can identify glandular tissue in the affected site (hyperintense foci on T2-weighted images)(17–19).
The treatment has two main pillars: the conservative treat-ment, based on hormone replacement to prevent recurrence of pneumothorax and hemothorax; and the surgical treatment that is indicated in cases of hormone therapy failure, severe treatment side effects, recurrence after treatment interruption, or if the pa-tient wants to become pregnant(20). Therefore, one may conclude
that catamenial pneumothorax should be suspected in the pres-ence of clinical signs coinciding with the menstrual period, and
that imaging studies can confirm the diagnosis. The treatment may be either surgical or medical, and should be appropriately indicated to avoid disease recurrence.
REFERENCES
1. Zanetti G, Nobre LF, Mançano AD, et al. Paracoccidioidomicose pul-monar. Radiol Bras. 2014;47(1):xi–xiii.
2. Fernandes MC, Zanetti G, Hochhegger B, et al. Pneumonia por Rho-dococcus equi em paciente com SIDA. Radiol Bras. 2014;47(3):xi–xiii. 3. Amorim VB, Rodrigues RS, Barreto MM, et al. Achados na tomografia computadorizada em pacientes com infecção pulmonar pelo vírus in-fluenza A (H1N1). Radiol Bras. 2013;46:299–306.
4. Eifer DA, Arsego FV, Torres FS. Atresia unilateral das veias pulmona-res: avaliação por tomografia computadorizada. Radiol Bras. 2013;46: 376–8.
5. Souza VF, Chaves RT, Balieiro VS, et al. Avaliação qualitativa e quan-titativa da densidade pulmonar em paciente com polimiosite e fibrose pulmonar. Radiol Bras. 2013;46(3):ix–x.
6. Marcos L, Bichinho GL, Panizzi EA, et al. Classificação da doença pul-monar obstrutiva crônica pela radiografia do tórax. Radiol Bras. 2013; 46:327–32.
7. Amoedo MK, Souza LVS, Souza AS, et al. Enfisema intersticial pulmo-nar: relato de caso e revisão da literatura. Radiol Bras. 2013;46:317–9. 8. Zanetti G, Nobre LF, Mançano AD, et al. Sinal do halo invertido com paredes nodulares causado por tuberculose pulmonar, confirmada por cultura do escarro. Radiol Bras. 2013;46(6):ix–x.
9. Koenigkam-Santos M, Paula WD, Gompelmann D, et al. Endobron-chial valves in severe emphysematous patients: CT evaluation of lung fissures completeness, treatment radiological response and quantitative emphysema analysis. Radiol Bras. 2013;46:15–22.
10. Silva JLP. O trinômio vírus-droga-hospedeiro na caracterização tomo-gráfica da infecção pulmonar por influenza A (H1N1) – uma visão clí-nico-radiológico-patológica. Radiol Bras. 2013;46(5):vii–ix. 11. Alifano M, Vénissac N, Mouroux J. Recurrent pneumothorax associated
with thoracic endometriosis. Surg Endosc. 2000;14:680.
12. Attaran S, Bille A, Karenovics W, et al. Videothoracoscopic repair of diaphragm and pleurectomy/abrasion in patients with catamenial pneu-mothorax: a 9-year experience. Chest. 2013;143:1066–9.
13. Bagan P, Berna P, Assouad J, et al. Value of cancer antigen 125 for diagnosis of pleural endometriosis in females with recurrent pneumotho-rax. Eur Respir J. 2008;31:140–2.
14. Costa F, Matos F. Endometriose torácica. Rev Port Pneumol. 2008;XIV: 427–35.
15. Cassina PC, Hauser M, Kacl G, et al. Catamenial hemoptysis. Diagno-sis with MRI. Chest. 1997;111:1447–50.
16. Yu Z, Fleischman JK, Rahman HM, et al. Catamenial hemoptysis and pulmonary endometriosis: a case report. Mount Sinai J Med. 2002;69: 261–3.
17. Marchiori E, Zanetti G, Rafful P, et al. Pleural endometriosis and re-current pneumothorax: the role of magnetic resonance imaging. Ann Thorac Surg. 2012;93:696–7.
18. Coutinho A Jr, Bittencourt LK, Pires CE, et al. MR imaging in deep pelvic endometriosis: a pictorial essay. Radiographics. 2011;31:549– 67.
19. Marchiori E, Zanetti G, Rodrigues RS, et al. Pleural endometriosis: findings on magnetic resonance imaging. J Bras Pneumol. 2012;38: 797–802.
20. Alifano M, Roth T, Broët SC, et al. Catamenial pneumothorax: a pro-spective study. Chest. 2003;124:1004–8.
Brainner Campos Barbosa1, Edson Marchiori2, Gláucia Maria Ribeiro Zanetti2, Jorge Luiz Barillo3
1. Hospital Santa Teresa, Petrópolis, RJ, Brazil. 2. Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brazil. 3. Universidade Federal Fluminense (UFF), Niterói, RJ, Brazil. Mailing Address: Dr. Brainner Campos Barbosa. Rua das Laranjeiras, 371, ap. 303, Edifício Marco Luiz, Laranjei-ras. Rio de Janeiro, RJ, Brazil, 22240-004. E-mail: brainnerc@gmail.com.
http://dx.doi.org/10.1590/0100-3984.2014.0067 Figure 2. Videothoracoscopy revealing the presence of endometriotic foci