BrazJOtorhinolaryngol.2016;82(1):56---64
www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
The
influence
of
(central)
auditory
processing
disorder
in
speech
sound
disorders
夽
Tatiane
Faria
Barrozo
a,
Luciana
de
Oliveira
Pagan-Neves
b,
Nadia
Vilela
a,
Renata
Mota
Mamede
Carvallo
b,
Haydée
Fiszbein
Wertzner
b,∗aSciencesofRehabilitationProgram,FaculdadedeMedicina,UniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil
bSpeech-LanguagePathologyandAudiologyProgram,DepartmentofPhysicalTherapy,Speech-LanguageandAudiology
andOccupationalTherapy,FaculdadedeMedicina,UniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil
Received24April2014;accepted28January2015 Availableonline20October2015
KEYWORDS
Articulation disorders;
Auditoryperception; Speechperception; Evaluation
Abstract
Introduction:Consideringtheimportanceofauditoryinformationfortheacquisitionand orga-nizationofphonologicalrules,theassessmentof(central)auditoryprocessingcontributesto boththediagnosisandtargetingofspeechtherapyinchildrenwithspeechsounddisorders.
Objective:Tostudyphonologicalmeasuresand(central)auditoryprocessingofchildrenwith speechsounddisorder.
Methods:Clinicalandexperimentalstudy,with21subjectswithspeechsounddisorderaged between 7.0 and 9.11years, dividedinto two groups according to their (central) auditory processingdisorder.Theassessmentcomprisedtestsofphonology,speechinconsistency,and metalinguisticabilities.
Results:Thegroupwith(central)auditoryprocessingdisorderdemonstratedgreaterseverity ofspeechsounddisorder.Thecutoffvalueobtainedfortheprocessdensityindexwastheone thatbestcharacterizedtheoccurrenceofphonologicalprocessesforchildrenabove7yearsof age.
Conclusion:Thecomparisonamongthetestsevaluatedbetweenthetwogroupsshowed dif-ferencesinsomephonologicalandmetalinguisticabilities.Childrenwithanindexvalueabove 0.54demonstratedstrongtendenciestowardspresentinga(central)auditoryprocessing disor-der,andthismeasurewaseffectivetoindicatetheneedforevaluationinchildrenwithspeech sounddisorder.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:BarrozoTF,Pagan-NevesLO,VilelaN,CarvalloRMM,WertznerHF.Theinfluenceof(central)auditoryprocessing
disorderinspeechsounddisorders.BrazJOtorhinolaryngol.2016;82:56---64.
∗Correspondingauthor.
E-mail:[email protected](H.F.Wertzner).
http://dx.doi.org/10.1016/j.bjorl.2015.01.008
PALAVRAS-CHAVE
Transtornosda articulac¸ão; Percepc¸ãoauditiva; Percepc¸ãodafala; Avaliac¸ão
Influênciadotranstornodoprocessamentoauditivo(central)notranstornofonológico
Resumo
Introduc¸ão: Considerando a importância das informac¸ões recebidas auditivamente para a aquisic¸ãoeorganizac¸ãodasregrasfonológicas,aavaliac¸ãodoprocessamentoauditivo(central) trazcontribuic¸õessignificativasparaodiagnósticoedirecionamentodaintervenc¸ão fonoaudi-ologiadascrianc¸ascomtranstornofonológico.
Objetivo: Estudarasmedidasfonológicaseoprocessamentoauditivo(central)decrianc¸ascom transtornofonológico.
Método: Estudoclínicoeexperimentalcom21sujeitoscomtranstornofonológico,entre7,0e 9,11anos,separadosemdoisgrupos:comesemtranstornodoprocessamentoauditivo(central). Foramavaliadasasprovasdefonologia,inconsistênciadefalaehabilidadesmetalinguísticas.
Resultados: Ogrupo com transtorno doprocessamento auditivo (central) apresentou maior gravidadedotranstornofonológico.Ovalordecorteobtidoparaoprocessdensityindexfoi oquemelhorcaracterizouaocorrênciadosprocessosfonológicosparacrianc¸asacimadesete anos.
Conclusão:A comparac¸ão do desempenho das provas avaliadas nos dois grupos mostrou diferenc¸asquantoaalgunsaspectosfonológicosemetalinguísticas.Ascrianc¸ascomvalordo índice acimade0,54demonstraram umaforte tendênciaaapresentar alterac¸ão no proces-samentoauditivo(central),sendoqueestamedidafoiefetivaparaindicaranecessidadede avaliac¸ãodecrianc¸ascomtranstornofonológico.
©2015Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Severalaspectshave beenexploredin thestudiesof chil-dren withspeechsounddisorder (SSD), which isa speech disordercharacterizedbyaninadequateuseof phonologi-calrulesoflanguage(DSM-IVF80.0---315.39).Thedynamic modelsthatattempttoexplainthedevelopmentofspeech production indicate an interactionbetween auditory per-ception, sound production, and sound representation.1,2
Thus, a detailed observation of the performance of chil-dren with SSD regarding centralauditory processingskills cancontributeagreatdealtotheunderstandingofspeech andlanguagemanifestations. The centralquestion of this studywastoinvestigatewhetherchildrenwithSSDwhowere diagnosedlate(between7and9years,11months)alsohave (central)auditoryprocessingdisorders.
Animpairmentinthephonologicalsystemisthemain fea-tureofSSDandmaystemfromspecificdifficultiesrelatedto cognitive-linguisticprocessing(organizationofphonological rules),auditoryprocessing,and/orspeechproduction.The interrelationship among these threeprocessings has been thesubjectofseveralstudies3---5thatsoughttoimprovethe
understanding of the manifestations observed in children withSSD.
Regardless of the SSD classification system used, the literature points to the existence of subtypes,6,7
demon-stratinga varietyofdifficultiesthat mayexhibitdifferent manifestationsandvaryingdegreesofexpression.Such man-ifestationscanbeidentifiedbyvarioustestscomplementary to phonological tests; for instance, speech inconsistency, metalinguistic skills, and those involving auditory orga-nization, assessed in (central) auditory processing (CAP) tests.
The classification of SSD severity is a complex task, because the clinician must consider the phonological changes,speechintelligibility,andageofthechild,among other factors. Some severity index classifications can be found inthe literature, suchasthe Percentage of Conso-nantsCorrect (PCC),8 itsrevised version,thePCC-R,9 and
theProcessDensityIndex(PDI).10
BothPCCandPCC-Rareintendedtoindicatethe percent-ageofcorrectconsonantsinaconventionalspeechsample. ThemaindifferencebetweenthesetoolsisthefactthatPCC considerssubstitutions,omissions,anddistortionsasspeech errors,while PCC-Rconsidersonlyconsonantsubstitutions andomissionsaserrors.
PDI verifies the occurrence of phonological processes, andisdistinctfromPCCandPCC-R,inasmuchasthesetwo latterindexesaccountforthecorrectconsonantsofspeech samples.PDIisinverselyproportionaltoPCCandtoPCC-R, inthatthelowerthevalueofPCC(orofPCC-R),thehigher thevalueofPDI;thatis,thelowerthepercentageofcorrect consonantsemployedinspeech,thehigherthefrequencyof useofphonologicalprocesses.11
PCC-RandPDIhavebeenappliedonBrazilianPortuguese (BP)-speakingchildrenwithSSD inthesame regionofthe countrywherethechildrenofthisstudylive.Studiesshow thatthisisanefficientindexforclassifyingSSDseverity.12---14
Intelligiblespeechdependsonefficientphonological pro-gramming,which reflects the individual’sability toselect thetargetphonemeandorganizethesoundsinthecorrect sequence.15 Difficultyinphonologicalprogrammingcanbe
evaluatedbythespeechinconsistencytest,12,15which
58 BarrozoTFetal.
Animportantfeatureofschool-agechildrenwithSSDis thattheyusually showdifficulties relatedtophonological processing;therefore, analyzing theawareness of smaller unitsthatmakeupspeechisanimportantstepinevaluating thesechildren.Severalmetalinguisticskillsareassessedin school-agechildren,includingrhymeandalliteration. The PhonologicalSensitivity Test(PST)16 checks the
phonologi-calcodingstrategiesofthechild,throughanevaluationof metalinguisticskillsofrhymeandalliteration(equaland dif-ferent).Thistesthastwoversions:auditory(withauditory support)andvisual(withbothauditoryandvisualsupport), which wasdesigned toverify ifchildren with SSD benefit fromvisualsupport.
To furthercomplementthe identification ofdifficulties facedbychildrenwithSSDandconsideringtheinteraction of auditory information received --- in association with the acquisition and organization of phonological rules in this population --- the evaluation of CAP brings significant contributions to the diagnosis of SSD and targeting for phonologicalintervention.Thiscontributionoccursbecause (central)auditoryprocessingdisorder(CAPD),definedasa difficultyinprocessing soundinformation, mayresultina difficultyinlanguagedevelopmentandinlearning.17
Althoughauditorydifficultiesaretheprimarycomplaints of children with CAPD, one study18 observed that other
impairments can be identified, such as those related to language, to reading and writing, and also to learning difficulties.
Importantly,therearefewstudiesthatcorrelateSSDwith CAP.ThismaybejustifiedbythefactthatSSDdiagnosisis mostoftenestablishedinchildrenaged5---7years,andalso becausetheapplication oftheCAP testis performedonly after7yearsofage,duetonecessityforthematurationof thestructuresinvolved.
Studies19,20inchildrenwithotherlanguageimpairments
---for instance, specific languageimpairmentand dyslexia --- showedthe importance of CAP assessment for comple-menting diagnosis, as children with these disorders may exhibitCAPDwithanimpairmentinskillsinvolving discrim-inationofspeechsounds,andthat mayresultin impaired and/orlessstableneuralrepresentationsofthesound, per-hapsinterferingwithperceptionandspeechproduction.
Several tests that assess auditory skills and that are alreadyadapted tothe Brazilian Portuguese language are available.Some of them have moreuse in theevaluation of CAP in children with SSD, by assessing specific speech understandingskills,withouttheirresultssuffering interfer-encefromthephonologicalchangepresentedbythechild. Amongthesetests,thefollowingarenotable:Picture Identi-ficationwithWhiteNoise,whichevaluatesauditoryclosure ability; Dichotic Digit Test, which evaluates figure-ground ability;andFrequency PatternandDurationPattern Tests, whichassessthehearingabilitiesoftemporalorderingand interhemispherictransfer.
Faced with the diversity of correlated causes and of phonologicalmanifestationsfoundinchildrenwithSSD,itis criticaltoobtainmoredetaileddescriptionsonaspectsthat complementthephonologicalevaluationinthesechildren. The aim of this study was to investigate phonological measuresand(central)auditoryprocessingofchildrenwith speechsounddisorder.
Methods
The study was approved by the Research Ethics Commit-teeof theuniversitywhere thestudywasconducted(No. 201/11).Aninformedconsentwassignedbytheparentor guardianofeachchild.
Twenty-onesubjects(bothgenders)diagnosedwithSSD, withagesbetween7.0and9.11years,wereincludedinthis study.Thediagnosiswasestablishedinaspecialized labora-torylinkedtotheuniversitywherethestudywasconducted. AccordingtoCAP evaluationresults,the subjectswere allocatedtothecontrolgroup(CG),with10subjects with-out CAPD, or to the study group (SG), with 11 subjects withCAPD.As inclusioncriteria,thechild neededtohave speecherrorsinthephonologicaltest21 andanage
appro-priate performanceon vocabulary,fluency,andpragmatic evaluations of the ABFW Child Language Test in phonol-ogy, vocabulary, fluency, and pragmatic areas22; needed
tohavecompletedthe(central)auditoryprocessing(CAP) examination23;needed tohave his/herhearing thresholds
within the normal range; and could not have undergone speechtherapy.Inaddition,theSpeechInconsistency Test (SIT)2 and the PST were applied.16 All participants were
BrazilianPortuguese-speakingsubjects.
ThephonologyevaluationoftheABFW21 consistsofthe
picturenamingtask(N)thatincludes34figureswith90 cor-rect consonants, and the imitation of words task (I)with 39wordstotaling107correctconsonants.Thetwo phonol-ogytestsweretranscribedtwicebyphonologyresearchers. Theagreementbetweenthetranscriptswas90%.Fromthe phonologicaltests,PCC,8PCC-R,9andPDI10severityindexes,
the number of different types of phonological processes, as well as the occurrence of each process, were calcu-lated.Thefollowingphonologicalprocesseswereanalyzed: syllablereduction(SR);consonantharmony(CH);stopping (S);velarbacking(VB);palatalbacking(PB);velarfronting (VF);palatalfronting(PF);liquidsimplification(LS);cluster reduction(CR);finalconsonantdeletion(FCD);stopvoicing (SV);fricativevoicing(FV);stopdevoicing(SD);andfricative devoicing(FD).
SIT12consistsof25picturesnamedthreetimesin
differ-ent sequences, interspersed by distracting activities. The threenamingsofeach wordwereanalyzed andclassified, andthesubjectwasconsideredasconsistentwhenhe/she namedthepictureequallyinthreedifferenttimes,andas inconsistentwhenatleastoneofthenamingswasperformed differently.Thespeechinconsistencyindex12representsthe
percentageofinconsistent wordsinthetest andwas ana-lyzedaccordingtothecriteriaestablishedbytheauthors, determiningwhois consistent or inconsistent,considering theestablishedcut-offvaluesaccordingtogenderandage. Subjectswereconsideredinconsistentwhentheyachieved inconsistencyindexratesbelowthecutoffvalues.Forgirls aged5.0---7.6years,thecutoffvalueis≥21.5%;fortheage
group above 7.6 years, it is ≥14.5%. For boys aged
5.0---7.6 years, the cutoff value is ≥31.9%; for the age group
above7.6years,itis≥17.6%.
For the evaluation of metalinguistic skills (rhyme and alliteration, equalanddifferent),thePST16 initsauditory
influence
of
auditory
processing
disorder
in
speech
sound
disorders
59
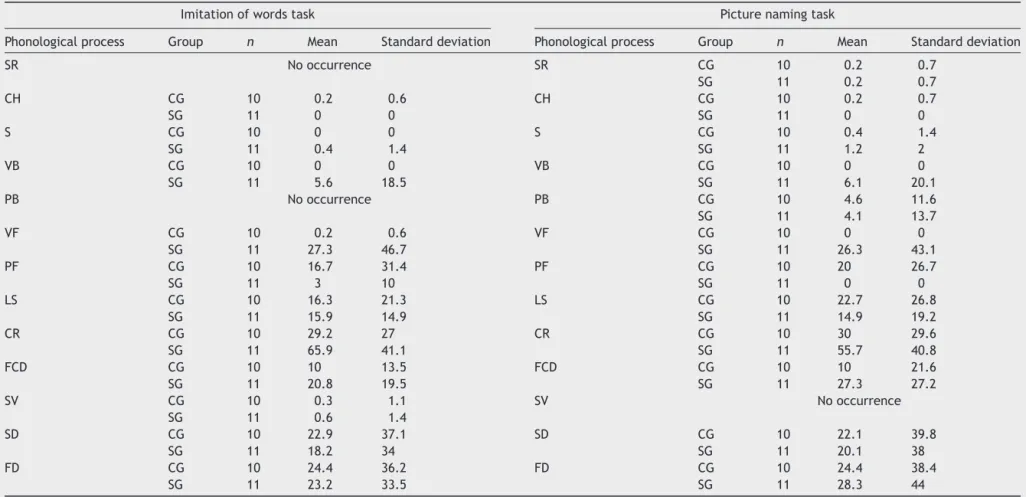
Table1 Descriptivevaluesforpercentageofoccurrenceofphonologicalprocessesinphonologytasksinthecontrolgroup(CG)andstudygroup(SG).
Imitationofwordstask Picturenamingtask
Phonologicalprocess Group n Mean Standarddeviation Phonologicalprocess Group n Mean Standarddeviation
SR Nooccurrence SR CG 10 0.2 0.7
SG 11 0.2 0.7
CH CG 10 0.2 0.6 CH CG 10 0.2 0.7
SG 11 0 0 SG 11 0 0
S CG 10 0 0 S CG 10 0.4 1.4
SG 11 0.4 1.4 SG 11 1.2 2
VB CG 10 0 0 VB CG 10 0 0
SG 11 5.6 18.5 SG 11 6.1 20.1
PB Nooccurrence PB CG 10 4.6 11.6
SG 11 4.1 13.7
VF CG 10 0.2 0.6 VF CG 10 0 0
SG 11 27.3 46.7 SG 11 26.3 43.1
PF CG 10 16.7 31.4 PF CG 10 20 26.7
SG 11 3 10 SG 11 0 0
LS CG 10 16.3 21.3 LS CG 10 22.7 26.8
SG 11 15.9 14.9 SG 11 14.9 19.2
CR CG 10 29.2 27 CR CG 10 30 29.6
SG 11 65.9 41.1 SG 11 55.7 40.8
FCD CG 10 10 13.5 FCD CG 10 10 21.6
SG 11 20.8 19.5 SG 11 27.3 27.2
SV CG 10 0.3 1.1 SV Nooccurrence
SG 11 0.6 1.4
SD CG 10 22.9 37.1 SD CG 10 22.1 39.8
SG 11 18.2 34 SG 11 20.1 38
FD CG 10 24.4 36.2 FD CG 10 24.4 38.4
SG 11 23.2 33.5 SG 11 28.3 44
n,numberofsubjects;SR,syllablereduction;CH,consonantharmony;S,stopping;VB,velarbacking;PB,palatalbacking;VF,velarfronting;PF,palatalfronting;LS,liquidsimplification;
60 BarrozoTFetal.
different)andalliteration(equalanddifferent)skills.Each testconsistsof15items;thefirstthreeitemsareusedto explainthetestandthefollowing12items,forapplication andanalysisofresponses.Inthealliterationparts,the sub-ject is requested to say which of the three words begins equallyor differentlyfromthe targetword; inthe rhyme test,thesubjectisaskedtosaywhichofthethreewords endsequallyordifferentlyfromthetargetword.The max-imumvalueforcorrectanswersforeachtestis12.
ThepresentstudyusedboththeAuditoryVersion(PST-A), whereinthesubjecthasonlyauditorysupportwhen answer-ing,andtheVisualVersion(PST-V),inwhichthesubjecthas auditorysupportassociatedtovisualsupport(pictures).The applicationofthetestwasdividedintofoursessions,to pre-ventinterferenceofthesubject’sfatiguewiththeresults, whichwereanalyzedaccordingtothecriteriaestablishedin theliterature.16
The Picture Identification Tests with White Noise,24
DichoticDigitTest,25FrequencyPatternTest,26andDuration
PatternTest26wereemployedfortheassessmentofCAP.The
criterionforidentifyingAPDinthetestedsubjectswasan observedchange inat least twoof the fouradministered tests.27
The evaluation of CAP was carried out in a special-izedlaboratory fromthesame universitywhere thestudy was conducted. To perform this test, we used a GSI-61 Grason-Stadleraudiometerwithfrequencyrangefrom125 to12,000Hz,andanintensityvariationof10---110dBHLfor puretonein thefrequenciesof125Hzand12,000Hz,and of−10to120dBHLforthefrequenciesof500,750,1000,
2000,3000, 4000,5000, and6000Hz.The calibration was carried out according to ANSI S36-1989; ANSIS3 43; IEC 645-1(1992); IEC645-2 (1993)and ISSO389; UL544,and wasconductedinasoundproofbooth(Siemens)calibrated accordingtoANSIS31-1991standards.
Statisticalmethod
Thefollowingstatisticaltestswereused:Fisher’sexacttest, Student’st-test,andtheMann---Whitneytest.Asto hypothe-sistests,thesignificancelevelwassetat0.05.Theanalysis
Table2 p-Valuesobtainedinthecomparisonof distribu-tionofLS,CR,FCD,SD,andFDprocessesbetweenControl GroupandStudyGroup.
Phonologicalprocess Phonologytask
Imitationofwords Picturenaming
LS 0.88 0.555
CR 0.041a 0.079
FCD 0.231 0.123
SD 0.852 0.938
FD 0.879 0.754
LS,liquidsimplification;CR,clusterreduction;FCD,final conso-nantdeletion;SD,stopdevoicing;FD,fricativedevoicing.
a Significantdifference.
wasperformedusingMinitab(version16)andSPSS(version 18)statisticalprograms.
Results
In the analysis performed by gender in both groups, the results showed that although there was no difference betweenpercentagedistributionforthisvariable(p>0.999, Fisher’sexacttest),itwasnotedthatmostofthesubjects weremale,bothintheCG(7)andtheSG(8).
Regardingthe subjects’ age, the valueswere CG (8.5) andSG(7.10);nosignificantdifferencesbetweenmeansof thegroupswereobserved(p=0.131,Student’st-test).
Astothenumberofdifferenttypesofphonological pro-cesses in phonological tests, the results showed that SG participantsusedameanoffourtypesofphonological pro-cessesineachofthetasks.Conversely,CGparticipantsused ameanofthreetypesofphonologicalprocesses.Although theSGhadameanhighernumberofphonologicalprocesses regardlessofphonologicaltest,thisdifferencewasnot sig-nificantwithrespecttoimitationofwords(p=0.458)orto picturenaming(p=0.538).
Thedescriptivevaluesforthepercentageofoccurrence of each phonological process in both phonological tasks (Table 1) show that the phonological processes with the
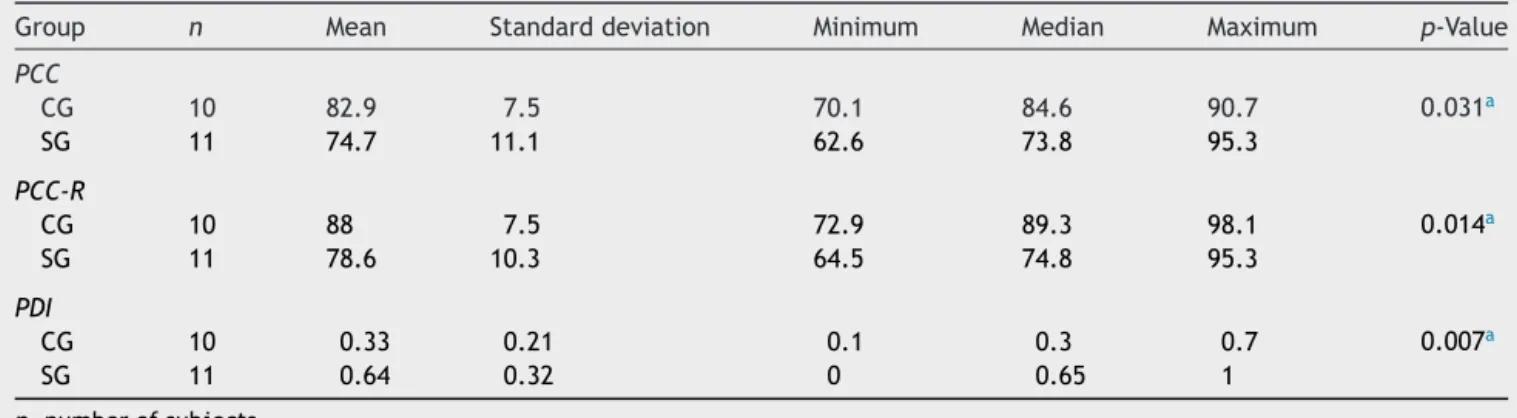
Table3 DescriptivestatisticsforPercentageofConsonantsCorrect(PCC),PercentageofConsonantsCorrect-Revised(PCC-R), andProcessDensityIndex(PDI)inthecontrolgroup(CG)andstudygroup(SG).
Group n Mean Standarddeviation Minimum Median Maximum p-Value
PCC
CG 10 82.9 7.5 70.1 84.6 90.7 0.031a
SG 11 74.7 11.1 62.6 73.8 95.3
PCC-R
CG 10 88 7.5 72.9 89.3 98.1 0.014a
SG 11 78.6 10.3 64.5 74.8 95.3
PDI
CG 10 0.33 0.21 0.1 0.3 0.7 0.007a
SG 11 0.64 0.32 0 0.65 1
n,numberofsubjects. Statistics:Student’st-test.
100
90
80
70
60
CG SG
Group
100
90
80
70
60
0.0 0.2 0.4 0.6 0.8 1.0
CG
CG
SG
SG
Group
Group
PCC
, %
PCC-R, %
PDI
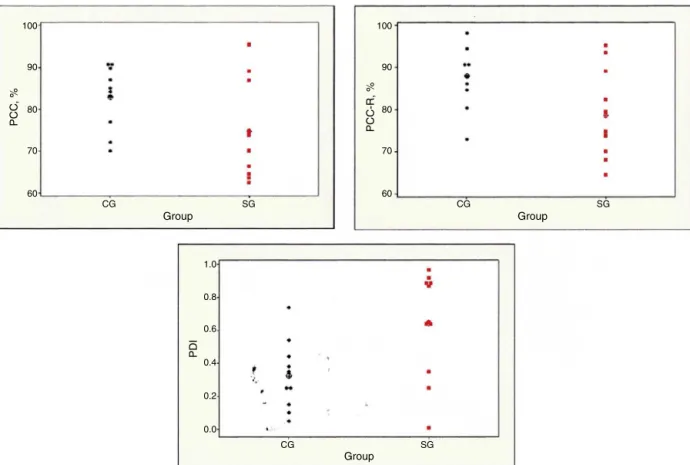
Figure1 Individual andmean valuesof Percentage ofConsonants Correct(PCC), Percentage ofConsonants Correct-Revised (PCC-R),andProcessDensityIndex(PDI)inthecontrolgroup(CG)andstudygroup(SG).
highestmeanpercentageofoccurrencewereLS,CR,FCD, SD,and FD. Depending onthese results, thedistributions oftheseprocesseswerecomparedbetweenthetwogroups (CGandSG;Table2),andadifferencewasfoundonlyforCR inthewordimitationtest,indicatingahigheroccurrenceof thisprocessinSG.
The descriptive valuesof PCC,PCC-R, andPDI in each group(Table3)showedthat,forallseverityindexes,there wasadifferenceinthecomparisonbetweengroups.Itcan beobservedthatthemeanvaluesofthePCCandPCC-Rwere lowerinSG,andthoseofthePDIwerehigherinthisgroup (Fig.1).
For the PDI index, a receiver operating characteristic (ROC)curvewasdrawn(Fig.2),indicatingthenearestpoint of the upper left corner corresponded to the higher sen-sitivity(0.73) andspecificity(0.90) values.Acutoffvalue of0.54wasassociatedwiththispoint.Theareaunderthe curve(AUC)of0.79confirmedthediscriminatorypowerof the PDI. Thus,subjects withPDI≥0.54 aremost likelyto
belongtoSG,i.e.,topresentanAPchange.
The resultsof SITclassificationsuggested that,inboth groups,thenumberofconsistentchildrenwashigher:sixin theCGandnineintheSG.However,nodifferencebetween the percentages of occurrence ofinconsistent subjectsin bothgroups(p=0.268,Fisher’sexacttest)wasfound.
DistributionsoffrequenciesandpercentagesofPST-Aand PST-VinCGandSG(Table4)showednodifferencebetween percentages of impaired results in the four tests in both
versions,both inthe CG(p=0.504) andtheSG(p=0.772, analysisofvariance);howeverthepercentageofimpaired resultswasgreaterintheSG(p<0.001,Fisher’sexacttest) in all PST-A tasks. In PST-V, the percentages of impaired resultswerehigherintheSG(p<0.001,Fisher’sexacttest), andthisresultwasindependentofthetask(p=0.196, anal-ysisofvariance).
ComparingPST-Avs.PST-V,ap-valueof0.095wasfound; thelackofstatisticalpowercanbeattributedtothesmall samplesizeinbothgroups.
0.0 0.0 0.2 0.4 0.6 0.8 1.0
0.2 0.4 0.6 0.8 1.0
1 - Specificity
Sensitivity
62 BarrozoTFetal.
Table4 FrequencydistributionsandpercentagesofPhonologicalSensitivityTest-Auditory(PST-A)andPhonologicalSensitivity Test-Visual(PST-V)inthecontrolgroup(CG)andstudygroup(SG).
CG SG
Impaired Normal Impaired Normal
n % n % n % n %
PST-A Initialsound
Equal 1 10 9 90 7 63.6 4 36.4
Different 0 0 10 100 7 63.6 4 36.4
Finalsound
Equal 1 10 9 90 9 81.8 2 18.2
Different 1 10 9 90 8 72.7 3 27.3
PST-V Initialsound
Equal 0 0 10 100 6 54.6 5 45.4
Different 0 0 10 100 3 27.3 8 72.7
Finalsound
Equal 2 20 8 80 7 63.6 4 36.4
Different 0 0 10 100 8 72.7 3 27.3
n,numberofsubjects.
Discussion
ThemanifestationsofSSDareheterogeneous,whichmakes their classification difficult.4 Thus, the present study
describedtheperformanceofchildrendiagnosedwithSSD invariousphonological(numberofdifferenttypesof phono-logical processes,SSD severity, andspeech inconsistency) andmetalinguistic(PST-VandPST-A)skills,dependingofthe presence/absenceofimpairmentinCAP.
The description of both groups, CG and SG, indicated nodifferenceregarding thesubjects’ age; a malegender predominancewasnotedinbothgroups.
Among the phonologicalmeasures examined, the num-berofdifferenttypesofphonologicalprocesseshasshown noevidenceofdifferencebetweenCGandSGinboth phono-logicaltasks.Nevertheless,SGpresentedhighermeansfor thisvariable,bothinimitationofwordsaswellasinpicture namingtasks.
Asforphonologicalprocesstypeswithhigherincidence, in general, the same findings already noted in previous studies with Brazilian Portuguese-speaking children were observed:SD,FD,LS,andCR.13Consideringthatthepresent
studycomparedtheperformanceofchildrenwithSSDwith and without CAPD, we found that CR was observed most frequentlyamongthesephonologicalprocesses,bothinthe CGandthe SG. Inaddition,CRwasthe onlyphonological processthatshoweddifferenceonly inimitationof words test between the twogroups, withgreater occurrence in theSG,suggestingthataCAPDcanhinderthephonological organizationofcomplexstructures.
Nonetheless,intheanalysisofthethreeseverityindices (PCC, PCC-R, and PDI), SG subjects presented higher SSD severitycomparedtosubjectswithoutCAPD,i.e.,SG sub-jectshadfewercorrectconsonantsandhigherincidenceof
phonologicalprocesses.Inastudyconductedamong Brazil-ian Portuguese-speaking children with SSD28 and without
CAPD, higher and more homogeneous values were found in thePCC-Rindex,suggesting thatchildren withSSD and CAPD showhigher SSD severity, i.e., greater phonological difficulty.
Evidencearisingfromthecomparisonofseverity meas-ures andphonological processesinchildren withSSDwith andwithoutCAPDiscriticalbecause,ingeneral,verylittle is discussed about CAP inthesechildren. Whereas studies usingdynamicmodelsrelatedtothedevelopmentofspeech areadvancing,theinteractionbetweenauditoryperception andtheproductionandphonologicalorganizationofspeech sounds are becoming more appreciated.1,2 Accordingly, a
verificationoftherelationshipamongphonologicalandCAP measurementsinchildrenover7yearsofagewithSSDshows thatsearchingfor thisrelationshipis notonlyappropriate butalsonecessary.
According to the literature,20 close relationships are
observedbetweenspeechimpairmentandCAPD,sinceCAP hinders the formation of phonemic representation in the brain, thus interfering with the learning of the rules of phonology,syntax,andsemantics.ThefactthatSGsubjects withCAPDemployedagreaternumberofdifferenttypesof phonologicalprocessesindicatesgreaterdifficultyin phono-logical representation, perhaps due to the difficulty that thesesubjectsseemtohaveinretrievingthephonological representations through auditory feedback during speech production.1
toCAPD.Thecutoffvalueidentifiedsuggeststhatchildren withSSDaged7yearsandpresentingPDI≥0.54maypresent
CAPD.ThiscutoffvalueprovidesevidencethatPDI,applied tospeechsamplesatthetimeoftheSSDdiagnosisfor chil-dren over 7years of age,is effective toidentifychildren inneedofreferral,onaprioritybasis,forevaluatingCAP. ByevaluatingCAP,additionalinformationcanbeobtained, greatly assisting the planning and execution of the treat-mentofeachchild.
The last phonological measure evaluated in the study --- the speech inconsistency classification --- was analyzed in order todetermine whetherchildren withinconsistent SSD hadCAPD.Ourstudy revealed nodifferencebetween groupsandthat,independentlyofthegroup,thenumberof consistentsubjectswasgreaterthanthenumberof incon-sistentones. This resultindicates that,for this sampleof subjects,phonologicalprogrammingdidnotsuffer interfer-ence of CAPD. Studies12,29 that have already applied the
speechinconsistency classificationindicatethatmost chil-drenwithSSDareconsistent,i.e.,theydonotexperience difficultyinphonologicalprogramming.
Regarding tests evaluating the metalinguistic skills of rhymeandalliteration,thestudyshowedthatthelevelof impaired resultswashigherinthe SGinthefoursubtests andinbothversionsofthePST.Thisfindingsuggestsa rela-tionshipbetweentheskillsinvolvedinCAPwiththoseofPST, i.e.,ifthechildshowsaCAPD,itismorelikelythat diffi-cultieswilloccurinthe metalinguisticskills ofrhymeand alliteration.Thiscanbeexplainedbythegreaterdifficulty ofperceptionandofauditoryorganizationpresentedbySG subjects,whichinterferes withtheabilitytoanswereach itemcorrectly,asinthecaseofthePST,thechildneedsto retainthestimulusinitsworkingmemoryandrecognizeif theinitialor finalsoundis equalor different.This finding suggestsaninterrelationshipoftheprocessingsinvolvedin speech.1,3ConcerningPST,thepresentstudycomparedthe
twoversionsofthetest(visualandauditory),andfoundno differencebetweentheseversionsinthetwogroups.Thus, thevisualsupportprovidedbythepicturespresentedin PST-V didnot help the performanceof children with SSD and CAPD.
This study wasdesigned tobe able toascertain if the phonologicalandmetalinguisticmanifestationsofchildren with SSD differed according to the presence of a CAPD. The studyof suchrelationshipcontribute toa more accu-rate diagnosis of SSD and tomore effective interventions forchildrenwiththisdisorder.Theanalysesperformedfor phonological and metalinguistic measures indicated that childrenwithSSDandCAPDhaveamoreseverecondition, present greater use of the CR phonological process,have moredifficultyinrhymeandalliterationskills,andalsodid notbenefitfromvisualcuesfortheseskills.
An importantfindingof thisstudywasthe cutoffpoint established for the PDI, which effectively differentiated children withSSD and CAPD fromthose withSSD without CAPD.Therefore,PDI,whichisanindexthatmeasuresthe occurrenceof phonological processesin aspeechsample, canbeappliedtotheevaluationofSSDdiagnosis, suggest-ingtheneedtoevaluatetheCAPinchildrenwithSSDaged over7years.
The principallimitationofthisstudywastherelatively small number of participants, since the age required for
assessingCAP isover 7years, andthe diagnosis of SSD is mostoftenmade beforethatage.Thatis thereasonwhy thenumberofchildrenwhomettheinclusioncriterionof agewasreduced.
This study is innovative because it demonstrated that children withSSD witha PDI value>0.54 exhibit a strong tendencytopresentCAPD.
Conclusion
AcomparisonofperformancesofchildrenwithSSDwithand withoutCAPDshowedevidenceofdifferencesamongthem onsomephonologicalandmetalinguisticskills.Childrenwith SSDandCAPDshowedhigheroccurrenceofthephonological processof CR,greater difficultyin rhymeand alliteration testsand,inaddition,werenotbenefited bythe pictures providedatthePST-V.TheyhadlowerPCC-RandhigherPDI values.Inaddition,childrenwithSSDwithaPDIvalueabove 0.54demonstratedastrongtendencytohaveCAPD,andthis measurewaseffectivetoidentifychildrenwithSSDinneed ofaCAPevaluation.
Funding
ThisstudywasfundedbyCAPES---InstitutionalQuota(Social Demand)---UniversidadedeSãoPaulo.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgement
CAPESscholarship.
References
1.GuentherFH.Corticalinteractionsunderlyingtheproductionof speechsounds.JCommunDis.2006;39:350---65.
2.Smith A. Development of neural control of orofacial move-mentsforspeech.In:HardcastleWJ,LaverJ,Gibbon,editors. Thehandbookofphoneticsciences.2nded.NewYork: Wiley-Blackwell;2010.
3.Dodd B, McIntoshB. The inputprocessing, cognitive linguis-ticandoro-motorskillsofchildrenwithspeechdifficulty.Int JSpeechLangPathol.2008;10:169---78.
4.Shriberg LD,FourakisM, HallSD, KarlssonHB, LohmeierHL, McSweenyJL,etal.Extensionstothespeechdisorders classifi-cationsystem(SDCS).ClinLinguistPhon.2010;24:795---824.
5.RvachewS,Brosseau-LapréF.Aninput-focusedinterventionfor childrenwithdevelopmentalphonologicaldisorders.Perspect LangLearnEduc.2012;19:31---5.
6.Shriberg LD, Lewis BD, Tomblin JB, Mcseeny JL, Karlsson BK, Scheer AR. Toward diagnostic and phenotype markers for geneticallytransmittedspeechdelay.JSpeechHearRes. 2005;48:834---52.
7.BetzSK,Stoel-GammonC.Measuringarticulatoryerror consis-tencyinchildrenwithdevelopmentalapraxiaofspeech. Clin LingPhon.2005;19:53---6.
64 BarrozoTFetal.
9.ShribergLD,AustinD,LewisBA,McSweenyJL.Thepercentage ofconsonantscorrectmetric:extensionsandreliabilitydata. JSpeechLangHearRes.1997;40:708---22.
10.EdwardsML.Clinicalforum:phonologicalassessmentand treat-mentinsupportofphonologicalprocesses.LangSpeechHear ServSch.1992;23:233---40.
11.WertznerHF, Amaro L,GaleaDES.Phonological performance measuredbySpeechSeverityIndexesrelatedtocorrelated fac-tors.SãoPauloMedJ.2007;125:309---14.
12.Castro MM, Wertzner HF. Speech inconsistency index in BrazilianPortuguese-speaking children.FoliaPhoniatrLogop. 2011;63:237---41.
13.Wertzner HF, Pagan LO, Galea DES, Papp ACCS. Caracterís-ticas fonológicas decrianc¸as com transtornofonológico com e sem histórico de otite média. Rev Soc Bras Fonoaudiol. 2007;12:41---7.
14.Wertzner HF,Claudino GL,Galea DES,PatahLK, Castro MM. Medidasfonológicasemcrianc¸ascomtranstornofonológico.Rev SocBrasFonoaudiol.2012;17:189---95.
15.DoddB.Evidence-Basedpracticeandspeech-language pathol-ogy: strengths,weaknesses, opportunities and threats.Folia PhoniatrLogop.2007;59:118---29.
16.HerreroSF[dissertac¸ão]Desempenhodecrianc¸ascom distúr-bio fonológico:testedesensibilidadefonológica ede leitura eescrita.SãoPaulo:FaculdadedeFilosofia,LetraseCiências Humanas,UniversidadedeSãoPaulo;2007.
17.JergerJ,MusiekFE.Reportofconsensusconferenceonthe diag-nosisofauditoryprocessingdisordersinschool-agedchildren. JAmAcadAudiol.2000;11:467---74.
18.Bellis TJ. Historical foundationsand thenature of(central) auditory processing disorder. In: Chermak GD, Musiek FE, editors. Handbook of (central) auditoryprocessing disorder: auditoryneuroscienceandclinicaldiagnosis.1sted.SanDiego: PluralPublishing;2007.p.119---36.
19.FlitchRH,TallalP.Neuralmechanismsoflanguage-based learn-ingimpairments:insightsfromhumanpopulationsandanimal models.BehavCognNeurosciVer.2003;2:155---75.
20.McArthurGM,BishopDV.Speechandnon-speechprocessingin people withspecific language impairment: a behavioral and electrophysiologicalstudy.BrainLang.2005;94:260---73.
21.WertznerHF.Fonologia.In:AndradeCRF,Befi-LopesDM, Fer-nandesFDM,WertznerHF,editors.ABFW:Testedelinguagem infantilnasáreasde Fonologia,VocabulárioFluência e Prag-mática.2nded.Carapicuiba:Pró-Fono;2004,98pp.
22.Andrade CRF, Befi-Lopes DM, Fernandes FDM, Wertzner HF. ABFW: Teste de linguagem infantil nas áreas de Fonologia, VocabulárioFluênciaePragmática.2nd ed.Carapicuiba: Pró-Fono;2004.p.5---32.
23.PereiraLD,SchochatE.Processamentoauditivocentral:manual deavaliac¸ão.1sted.SãoPaulo:Lovise;1997,231pp.
24.Almeida CIR, Caetano MHU. Logoaudiometria utilizando sentenc¸as sintéticas. Rev Bras Otorrinolaringol. 1988;54: 68---72.
25.SantosMFC, Pereira LD. Escuta com dígitos. In: Pereira LD, SchochatE,editors.Processamentoauditivo central:manual deavaliac¸ão.1sted.SãoPaulo:Lovise;1997.p.147---9.
26.Auditec.Evaluationmanualofpitchpattersequenceand dura-tionpatternsequence.Missouri,USA:Auditec;1997,26pp.
27.Sharma M, Purdy SC, Kelly AS. Comorbidity of auditory processing,languageandreadingdisorders.JSpeechLangHear Res.2009;52:706---22.
28.VilelaN, WertznerHF, Sanches GSG, Neves-Lobo IF,Carvallo RMM. Processamento temporal de crianc¸as com transtorno fonológicosubmetidasaotreinoauditivo:estudopiloto.JSoc BrasFonoaudiol.2012;24:42---8.