www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Function
of
obturator
prosthesis
after
maxillectomy
and
prosthetic
obturator
rehabilitation
夽
,
夽夽
,
夽夽夽
Cheng
Chen
a,
Wenhao
Ren
a,
Ling
Gao
b,
Zheng
Cheng
c,
Linmei
Zhang
a,
Shaoming
Li
a,
Pro
Ke-qian
Zhi
d,∗aDepartmentofOralMaxillofacialSurgery,StomatologyHospitalofXi’anJiaotongUniversityCollegeofMedicine,Xi’an,
Shaanxi,China
bKeyLaboratoryofEnvironmentandGenesRelatedtoDiseases,CollegeofMedicine,Xi’anJiaotongUniversity,Xi’an,
Shaanxi,China
cDepartmentofGeneralDentistry,StomatologyHospitalofXi’anJiaotongUniversityCollegeofMedicine,Xi’an,Shaanxi,China dDepartmentofOralMaxillofacialSurgery,StomatologyHospitalofXi’anJiaotongUniversityCollegeofMedicine,
XinchengDistrict,China
Received25September2014;accepted28January2015 Availableonline6November2015
KEYWORDS Mouthneoplasms; Maxillofacial prosthesis;
Recoveryoffunction; Questionnaires
Abstract
Introduction:Maxillarydefectsareusuallyrehabilitatedbyaprostheticobturator.
Objective: Thisstudyaimedtoevaluatethefunctioningofobturatorsprosthesisinpatients withunilateraldefectsaftermaxillectomy.
Methods:Of49patients,28underwenttomaxillectomyasaresultoftumorablativesurgery, andacquiredunilateralmaxillarydefects.Evaluationofthefunctionwasperformedbyapplying theObturatorFunctionalScale(OFS).
Results:Fromatotalof49patients,28weretreatedasfollows:9withaconventionalretained obturator prosthesis (COP), 11 (39%) with an enhancedretentive obturator prosthesiswith stud attachment (POP) and 8 (28%) with an enhanced retentive obturator prosthesis with magnetic attachment (POM). The mean OFS score was 80. Scores on functions ofspeech, swallowing and chewing reached statistical significances (p<0.05) among these three sub-groups.ComparingCOPandMOPgroups,thescoresofOFSinthedomainsof‘‘Speech-ability tospeak inpublic’’and‘‘Swallowing-leakagewithliquids’’were significantlyhigherinAOP group. Comparing COP group, the scores of OFS in ‘‘Swallowing-leakage with solid’’ and ‘‘Chewing/eating’’domainswereincreasedsignificantly(p<0.05)bothinMOPandAOPgroups.
夽
Pleasecitethisarticleas:ChenC,RenW,GaoL,ChengZ,ZhangL,LiS,etal.Functionofobturatorprosthesisaftermaxillectomyand prostheticobturatorrehabilitation.BrazJOtorhinolaryngol.2016;82:177---83.
夽夽Casereport:Cross-sectionalhistoricalcohortstudy.
夽夽夽 Institution:DepartmentofOralMaxillofacialSurgery,StomatologyHospitalofXi’anJiaotongUniversityCollegeofMedicine. ∗Correspondingauthor.
E-mail:[email protected](P.K.-q.Zhi). http://dx.doi.org/10.1016/j.bjorl.2015.10.006
Conclusion:Obturatorprosthesisimprovesoralfunctionofpatientsaftermaxillarydefects;the retentionoftheobturatorprosthesisenhancedbytheadditionofattachmentsshowedmore benefitsinoralfunction.
© 2015 Associac¸ão Brasileira de Otorrinolaringologia e Cirurgia Cérvico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license
(https://creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE Neoplasiasdaboca; Prótesemaxilofacial; Recuperac¸ãoda func¸ão;
Questionários
Func¸ãodapróteseobturadoraapósmaxilectomiaereabilitac¸ãoprotéticaobturadora
Resumo
Introduc¸ão:Emgeral,osdefeitosdamaxilasãoreabilitadosporumapróteseobturadora. Objetivo: Oestudoavaliouofuncionamentodapróteseobturadoraempacientescomdefeitos unilateraisapósmaxilectomia.
Método: De 49 pacientes, 28 foram submetidos a maxilectomia como cirurgia de ablac¸ão tumoraletiveramcomosequeladefeitosmaxilaresunilaterais.Aavaliac¸ãodofuncionamento foiefetuadapelaaplicac¸ãodaEscalaFuncionaldoObturador(EFO).
Resultados: Deum total de 49 pacientes, 28 foramtratados da seguinteforma: novecom prótese obturadora retentiva convencional (POC), 11 (39%) com prótese obturadora reten-tivacomfixac¸ãoporpino(POP) eoito(28%) compróteseobturadora retentivacomfixac¸ão magnética (POM). O escore médio na EFO foi de 80. Os escores para func¸ões da fala, deglutic¸ãoemastigac¸ãoalcanc¸aramsignificânciaestatística(p<0,05)entreostrêssubgrupos. Nacomparac¸ãoentreosgruposPOCePOM,osescoresdaEFOnosdomíniosda‘‘Fala-capacidade de discursar em público’’ e ‘‘Deglutic¸ão-vazamento de líquidos’’ foram significativamente maisaltosnogrupoPOP.Nacomparac¸ãocomogrupo POC,osescores daEFOnosdomínios de‘‘Deglutic¸ão-vazamentocomsólido’’e‘‘Mastigac¸ão/ingestão’’estavamsignificativamente aumentados(p<0,05)nosgruposPOMePOP.
Conclusão:A próteseobturadoramelhorouofuncionamento oraldepacientescomdefeitos maxilares;aretenc¸ãodapróteseobturadorareforc¸adapelaadic¸ãodedispositivosdefixac¸ão demonstroumaioresbenefíciosnafunc¸ãooral.
© 2015 Associac¸ão Brasileira de Otorrinolaringologia e Cirurgia Cérvico-Facial. Publi-cado por Elsevier Editora Ltda. Este é um artigo Open Access sob a licença CC BY
(https://creativecommons.org/licenses/by/4.0/deed.pt).
Introduction
The survival rates of patients with head and neck can-cer have improved in past several decades.1---3 Functional rehabilitation and quality of life (QOL) after maxillofa-cial surgery have been emphasized in recent years. It mainlydependsonoutcomesofmaxillofacialreconstruction andrehabilitationinvolvingfunctions,esthetics,psychology acceptanceand resocialization.4 Prostheticobturator was theprimarymethodemployedinrehabilitatinglarger max-illarydefects.5---8Theaimwastoclosethedefect,separate theoralcavityfromnasalcavitiesandpreventhyper-nasal speech,nasal regurgitationof food and liquids, and sup-portthefacialprofile.Basedonlocationandsizeofdefect, healthconditionsof remainingteethand bones,available softtissueundercutsandmuscularcontrol,various obtura-torprostheseswithdifferentretentivedesignswereusedto improveoralfunctions.
Besidesconventionalretainedobturatorprosthesis, oth-erswithvariousretentivetypes9---11 forenhancingstability and retention of prosthesis have been widely used. It wasreportedbysomeresearchersthatobturator prosthe-sis with enhanced retention can improved oral functions
postoperatively. But compared to conventional prosthe-sis, controversy exists whether the reinforced design of obturator had morebenefits.12 Therewere few studies in comparisonandevaluationofvariousobturatorprostheses functionallyaftermaxillarydefects.13
In this study patients with similar unilateral maxillary defects were treated withthree types of obturator pros-theses.ObturatorFunctionalScale(OFS)questionnaireswas appliedtoassessoralfunctionsamongthethreesubgroups.
Methods
foran extravisit.Oneyearafterrehabilitationwith obtu-rator prosthesis thepatients were asked tocomplete the OFS for function evaluation. Forty-nine patients met the criteria.Thestudywasapprovedbythelocalethicalboard of the College of Medicine (n◦ XJTULAC2014-203), Xi’an
Jiaotong University and informed consent was obtained. Based on medical records, the condition of preoperative dentitionwasconsideredgoodwhennomorethan6 maxil-laryteethweremissingbeforesurgeryandwasconsidered poorwhen 6or moremaxillaryteethweremissingbefore surgery.14 Sizes of maxillectomy defects were established fromtheoperativeandradiographicrecordsusingtheBrown classification.15Basedonretentivetypes,Allpatientsinthis studyweredividedinto3subgroups:patientswhoreceived conventionalretainedobturatorprosthesis(COP),patients whoreceivedenhancedretentiveobturatorprosthesiswith studattachment(AOP)andpatientswhoreceivedenhanced retentive obturator prosthesis with magnetic attachment (MOP).
Obturatorfunctionscale
The OFS wasused toassess the self-reported function of obturatorprostheses.EightdomainsinOFSquestionnaires, including satisfaction with facial appearance, ability to speak in public, leakage with liquids and solids, dryness of mouth, insertion of an obturator, chewing or eating, social---family interactions and overall OFS, were scored. Responses toOFSwerecompleted bytelephone or subse-quentvisits.Numericalvaluefrom0to100foreachresponse inthequestionnaireswasused.Ascoreof0indicates maxi-mumsufferingordissatisfactionandascoreof100indicates that thepatient wasasymptomatic or extremely satisfied in therespectivedomain.16 Thequestionnaireshave been validatedandusedbyotherinvestigators.17,18Internal con-sistencyofthequestionswasassessedbyCronbach’salpha test. The English version of OFSquestionnaires were cre-atedbyChigurupatiandtranslatedintoChineseversionfor investigation.TheChineseversionofOFSwasalsovalidated inChinaviareliabilitytestandusedinotherresearch.19
Statisticalanalysis
The data of medical records was listed in Table 1. Age, sex, tumor diameter, pathology diagnosis, chemical ther-apy, radiation therapy,premorbid dentition andmodel of enhanced retention were selected as demographic and treatmentvariables.Datagatheredfrompatientresponses to OFS were scored and analyzed. The impact of select demographicandtreatmentvariablesonOFSwasassessed: 1 --- age (>60 or ≤60years); 2 --- sex (male or female); 3 --- chemotherapy (yes or no); 4 --- postoperative radia-tiontherapy(yesorno); 5---premorbid dentition(goodor poor).Statisticalanalysiswasperformedusing nonparamet-ricKruskal---Wallisranksumsanalysisandposthocanalysis withSPSS18.0.CorrelationanalysisbetweenOFSand demo-graphicvariableswascalculatedbylikelihoodratioinANOVA analysiswithSPSS18.0.Theresultswereconsidered signif-icantatp<0.05.
Table1 Socialandmedicalcharacteristicsofpatients.
Variables n=28
Age(X±SD) 62.05±8.84(47---81)
Sex(M/F) 19/9
Tumordiameter(X±SD,mm) 4.2±1.4mm
Pathologydiagnosis 5/23
Salivaadenoidcysticcarcinoma 11 Squamouscellcarcinoma 7 Mucoepidermoidcarcinoma 5
Myoepithelialadenoma 2
Pleomorphicadenoma 1
Ameloblastoma 2
Chemicaltherapy 10
Radiationtherapy 2
Premorbiddentition(G/P) 18/10 Brownclassification(2a/2b) 15/13 Modelofenhancedretention
Conventionaldesigned 9
Attachmentenhanced 11
Magnetenhanced 8
F,female;M,male;B,benign;M,malignance;G,good;O,poor; X,samplemean;SD,standarddeviation.
Results
Ofthe49patients,4patientshaddied,and6patientswho didnotcontactbytelephoneorpostalmailwereexcluded. Ofthe 39 patients,28 patients wereincluded; 6 patients withacquiredbilateralorsmalldefectswereeliminated;5 patientshadotherproblems(advancedageandpoor phys-icalcondition).The ageofthepatientsrangedfrom47to 81years(mean,62.05years;standarddeviation[SD]8.84 years).Timeelapsedfrommaxillectomyandrehabilitation ofprosthesestoOFSresponseinthisstudyrangedfrom1.8 to6.8 years(mean, 2.5 years;SD,1.3 years). Sixty-eight percentof thepatientsweremen,andthemeanage was 61years.Ofthe28patients,11patientswerediagnosedas salivaryadenoidcysticcarcinoma (SACC); 7patientswere diagnosedwithsquamouscellcarcinoma(SCC); 5patients werediagnosedasmucoepidermoidcarcinoma; 2patients werediagnosedasmyoepithelialadenoma;2patientswere diagnosedasameloblastoma and only1 patientwas diag-nosedas pleomorphic adenoma.Thirty-six percent (10 of 28) received postoperative chemotherapy and 2 patients receivedradiotherapy.Thepreoperativedentitionwasgood in64%(18of28)ofpatients.Basedonmodelsofenhanced retention,ofthe28patients,9patients(32%)receivedCOP, 11patients(39%)receivedAOPand8patients(28%)received MOP.
ThemeanscoresofeachdomaininOFSarepresentedin
Table2 ScoreofOFSquestionnairesinpatients.
DomainsofOFS Total Subgroups p-Value
(n=28) COP(n=9) AOP(n=11) MOP(n=8)
Satisfactionwithfacialappearance 65.18±22.91 69.44±20.83 68.18±22.16 56.25±25.88 0.13
Speech 85.82±19.00 81.56±24.22 91.00±15.41 83.50±17.64 0.05
Speech-abilitytospeakinpublic 64.43±23.98 55.78±23.75 78.91±22.45b 54.25±17.59b 0.02a
Swallowing-leakagewithliquids 66.82±20.39 59.44±14.99 78.91±22.45b 58.50±15.73 0.01a
Swallowing-leakagewithsolids 59.68±16.87 44.33±17.00 70.00±9.94b 62.75±12.02b 0.01a
Chewing/eating 63.21±24.70 40.67±22.44 79.00±16.65b 66.88±17.91b 0.01a
Saliva-drynessofmouth 75.21±17.19 78.00±16.50 69.91±18.00 79.37±17.07 0.07 Insertionofobturator 83.93±23.78 77.78±26.35 81.82±25.22 93.75±17.67 0.02a
Socialfamilyinteraction 60.89±16.08 59.44±14.99 63.81±18.14 58.50±15.74 0.03a
OverallOFSscore 80.00±14.40 68.89±14.53 89.09±10.44b 80.00±10.69 0.01a
OFS,ObturatorFunctionScale;AOP,attachmentretainedobturatorprosthesis;COP,conventionalobturatorprosthesis;MOP,magnetic obturatorprosthesis.
aStatisticalsignificance,p<0.05(Kruskal---Wallisranksumsanalysis).
b Statisticalsignificance,p<0.05.AposthocanalysisreachedsignificanceamongCOPgroup,AOPgroupandMOPgroup(Duncansums
analysis).
rehabilitation. Comparing COPand MOP groups, scores of OFSinthedomainsof‘‘Speech-abilitytospeakinpublic’’ and ‘‘Swallowing-leakage with liquids’’ were significantly higherin AOPgroup. While comparing COP group, scores ofOFSindomainsof‘‘Swallowing-leakagewithsolid’’and ‘‘Chewing/eating’’ were increased significantly (p<0.05) bothinMOPandAOPgroups.Furthermore,overallOFSscore reachedstatisticalsignificanceinAOPgroup.
The impact of the select demographic and treatment variablesonOFSdomainsarepresentedinTable3.Overall OFScorrelatedsignificantlywithpostoperativeradiotherapy and premorbid dentition (p<0.05). Furthermore, scores on ‘‘interaction’’, ‘‘speech in public’’ and ‘‘satisfaction appearance’’correlatedwithpremorbiddentition.
Discussion
Theobturatorprosthesesweremainlyusedinrehabilitating maxillary defect.8 Theoretically, well-designed obturator prosthesesformaxillarydefectswerenotonlytomaintain durableandgoodretention,stability,andsupport,butalso torelievepainandresultineaseof use.Oneofthemost crucialpartsfor applicationof obturator prosthesis isthe retentionofprosthesis.20Withthedevelopmentofresearch and improved techniques, there were various strategies, designsandmaterialstoachieveenhancedretention,such aspreciseattachmentsupportedbyimplantretentive obtu-ratorprosthesis.21,22 Inthisstudy,weevaluatedretrospect dataof medicalrecordsover past 10years inour depart-ment.The strongest predictor ofOFSwasretentive type; OFScorrelatedstronglywithcondition ofremaining teeth andradiationtherapy.
Itwasevidentbypreviousstudiesthatlocationandsize ofthemaxillectomydefecttremendouslyinfluenced func-tionsof obturator prostheses.17,23 Rogers etal.24 reported thatpatientswithlargerdefectshadlowerscoresfor activ-ity,recreation,physical function. Okayetal.25 concluded thatstabilityofprosthesiswascompromisedasthedefect sizeincreased,resultinginpoorobturatorfunction.Brown
andShaw15 summarized thatobturator reconstructionwas offeredtopatientswithClass1to2aand2bdefects,buta composite free flapoption waspreferred for larger alve-olar and Class 3 or 4 defects, when appropriate to the patient’s medicalfitness and personal choice. But Chigu-rupati et al.14 reported that the size of defect did not correlate with obturator function on those patients who acquired maxillarydefects(Brown Class2aor 2b).Similar withChigurupati’sreport,ourstudyshowedthatoral func-tionswerecorrelatedwithsizeofdefects.Thismightbedue to improvement of surgeon’s reconstruction plan accord-ingtoprevioustreatmentexperience.Additionallyinorder to reduce bias, installation and fabrication of obturator prosthesesofallpatientswerefinishedonlybysingle expe-rienced prosthodontist and single dental technician. The prosthodontist checked oral conditions of patients, stud-iedresidualboneandteethpreoperatively,andevaluated conditionsofremainingteeth.
Previousinvestigators have confirmedthat the number ofremainingabutmentteethandperiodontalhealthplayed a vital rolein stability and retention of prosthesis.26 The distance of the direct retainertothe fulcrum line of the prosthesiscanalsoaffectthestabilityoftheobturator.Of the28patients,64.3%hadgoodconditionsofresidualteeth andresidualalveolarbone(mesialtodefects).Inaccordance withapreviousreport,17inthisseriesconditionofdentition influencedseverelyfunction ofobturator.There were sig-nificantcorrelationsbetweendentitionanddomainsofOFS. Sowerecommendedthatremainingteethshouldbe evalu-atedandtreatedbeforeoperation.Addingextraretentive appliancealsorequireshealthyteeth.
Table3 Impactoftreatmentanddemographicvariablesonselectedindividuals.
Predictorvariable Patientsn◦ Domains Meanscore(SD) p-value
Sex 16(male) Nonea
13(female) Chemical
therapy
18(no) None
10(yes)
Age 9(<60) None
19(≥60)
Brownclassification 15(2a)13(2b) None Postoperative
radiotherapy
26(no) Overall OFS
82.31±11.77 0.01b
2(yes) 50.00±14.14
Premorbid dentition
18(good) OverallOFS 83.33±14.14 0.02b
10(poor) 74.00±13.50
Interaction 68.83±7.78 0.01b
46.60±17.56 Speechin
public
63.00±30.12 0.01b
67.00±0.00 Satisfaction
appearance
66.67±21.00 0.04b
62.50±27.00
SD,standarddeviation;OFS,ObturatorFunctioningScale.
a NosignificantcorrelationsintheallOFSdomains. b p<0.05,significantcorrelation.
radiationtherapy,sotheinfluencesbyradiationtherapylack support.
OFSwasfinishedwithinthesecondyearafter rehabilita-tiontoanalyzethedifferences.Inthisstudy,comparedwith other groups, the AOP group demonstrated better scores inalldomainsofOFS,particularlyinspeech,chewingand swallowing. Patients withobturator prosthesis which was enhancedbystudattachmentdobetterthanconventional and magnetic retentiveprosthesis in improving oral func-tion,especiallyinspeechandswallowing.Consistentwith
ourreports,thefunctionofobturatorwasenhancedwhen addingattachment reported by other investigators.27 The retentionofconventionalprosthesesmainlydependson set-tingvarious claspsto healthyabutment; and thestability gainedfromremainingteeth andbone. But claspshave a horizontalforceinstantaneouslytoabutmentteethcaused bycyclesofinsertion/removal,andmayleadtochronic peri-odontaldamageinevitably.28Thusthetoothadjacenttothe defectsufferedmanyoverburdenoutsideforces,resulting inrapid periodontaldamages of the tooth. Fordelivering
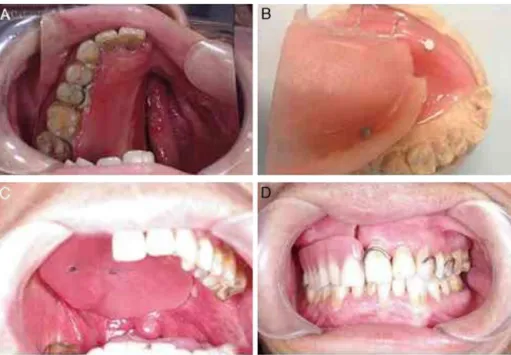
Figure2 (A)Viewofdefectsbeforedefiniterehabilitation;(B)imageoftissuesurfaceofobturatorandmagneticattachment; (C)set-upofobturator;(D)intraoralviewofthedenture.
thestressesdirectedattheprimaryabutmentteeth, fixa-tionofsomeoralloftheremainingteethmaybebeneficial. Studattachmentswereeconomical,easy-replaced,andone ofthemostimportantbenefitswasreductionofthe unbal-ancedstressontheabutmentteeth.Inthisstudy,aporcelain fusedmetalcontinuous bridgewas basedonloweringthe burdenoftheabutmenttoothadjacenttodefect(Fig.1). Inconsiderationofthelargeone-sidedefectandtothesex of thepatient, infemale patients studattachment might beabetter choicefor enhancing retentionand improving estheticsandpatient’sconfidence.
Prosthesisretainedbymagneticattachmentwaswidely usedin strengthening retention. In this series, compared with other groups, OFS scores were higher in ‘‘Insertion of obturator’’ and ‘‘Saliva-dryness’’ in MOP group. It is obviouslythatseparateddentureandobturatorwereeasier tosetuporremove(Fig.2).Buttherewasnostatistical sig-nificanceamongthreegroups.Thereasonmightbethatthe obturatorforclosureofthenasaldefectusuallyiscreated largerinvolumeandweight.Althoughitcouldobtain bet-terretentionandclosureatrest,stabilitywascompromised immediatelywhenexercisedfunctionallyafterinsertionof theunderpartofprosthesis.
Thesmallsampleanddurationoffollow-uparethemain limitations in thisstudy, but it bringsnew insight related toprostheticobturationofmaxillarydefectsaftersurgical resectionofmalignanttumorsof oral cavity,more specif-ically the hard palate. The lack of long term follow-up andmultivariateanalysisforotherimportantpredictorsand treatmentvariablesaretheotherlimitationsinthisstudy. Alongitudinal,prospectivestudywithalargesampleshould beconsideredinthefuture.
Conclusion
Obturator prostheses improve oral function of patients after maxilla defects; retention of the obturator
prostheses enhanced by the addition of an attachment showsmorebenefitsinoralfunction.
Funding
This study wassupported in part by the Key Science and TechnologyProgramofShaanxiProvince(n◦
2010ZDKG-50), theProjectofTechnologicalInnovationPlanninginShannxi Province(n◦2012KTCL03-17),theSpecializedResearchFund
fortheDoctoralProgramofHigherEducationofChinaand Natural ScienceFoundation of China (n◦ 81272957 and n◦
81171398).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
Thanks Chigurupatifor supplying scale of OFS.This study wassupported in part bythe Key ScienceandTechnology ProgramofShaanxiProvince(n◦2010ZDKG-50),theProject
of Technological Innovation Planning in Shannxi Province (n◦ 2012KTCL03-17),theSpecializedResearchFundforthe
DoctoralProgramofHigherEducationofChinaandNatural ScienceFoundationofChina(n◦81272957andn◦81171398).
References
1.DruganC,Leary S, MellorT, BainC,Verne J, NessA, et al. HeadandneckcancerinthesouthwestofEngland,Hampshire, andtheIsleofWight:trendsinsurvival1996---2008.BrJOral MaxillofacSurg.2013;51:19---24.
cancer:an analysisfrom Thailand. AsianPac J Cancer Prev. 2012;13:885---90.
3.BrothertonJML,SteinAN,ConwayEL,ReganDG,GrulichA,Law M,etal. Human papillomavirusand headand neck cancers: emergingtrendsandimprovingsurvival.AustNZPublHealth. 2012;36:195---6.
4.HumphrisGM, IrelandRS, Field EA.Thepsychological effect ofinformationaboutoralcancerinprimarycare.JDentRes. 2001;80:1152---62.
5.Dingman C, Hegedus PD, Likes C, McDowell P, McCarthy E, ZwillingC.A coordinated,multidisciplinaryapproach to car-ingforthepatientwithheadandneckcancer.JSupportOncol. 2008;6:125---31.
6.O’FearraighP.Reviewofmethodsusedinthereconstruction andrehabilitationofthemaxillofacialregion.JIranDentAssoc. 2010;56:32---7.
7.DesjardinsRP,Laney WR.Prostheticrehabilitation after can-cer resection in the head and neck. Surg Clin North Am. 1977;57:809---22.
8.ArianiN,VisserA,vanOortRP,KusdhanyL,RahardjoTB,Krom BP,etal.Currentstateofcraniofacialprostheticrehabilitation. IntJProsthodont.2013;26:57---67.
9.GrossmannY, MadjarD. Resinbonded attachments for max-illaryobturatorretention: aclinicalreport.JProsthetDent. 2004;92:229---32.
10.EtienneO,TaddeiCM.Useofbar-clipattachmentstoenhance theretentionofamaxillofacialprostheticobturator:aclinical report.JOralRehabil.2004;31:618---21.
11.MuratS, Gurbuz A, IsayevA, DokmezB, Cetin U. Enhanced retentionofamaxillofacialprostheticobturatorusingprecision attachments:twocasereports.EurJDent.2012;6:212. 12.SalinasTJ.Prostheticrehabilitationofdefectsoftheheadand
neck.SeminPediatrSurg.2010;24:299---308.
13.KeyfF.Obturatorprosthesesforhemimaxillectomypatients.J OralRehabil.2001;28:821---9.
14.ChigurupatiR, Aloor N, Salas R, Schmidt BL. Quality of life aftermaxillectomyand prostheticobturatorrehabilitation. J OralMaxillofacSurg.2013;71:1471---8.
15.BrownJS,ShawRJ.Reconstructionofthemaxillaandmidface: introducinganewclassification.LancetOncol.2010;11:1001---8. 16.Young CW, Pogrel MA, Schmidt BL. Quality of life in patientsundergoingsegmentalmandibularresectionandstaged
reconstructionwithnonvascularizedbonegrafts.JOral Maxillo-facSurg.2007;65:706---12.
17.RiazN,WarriachRA.Qualityoflifeinpatientswithobturator prostheses.JAyubMedCollAbbottabad.2010;22:121---5. 18.IrishJ,SandhuN,SimpsonC,WoodR,GilbertR,GullaneP,etal.
Qualityoflifeinpatientswithmaxillectomyprostheses.Head Neck.2009;31:813---21.
19.JiaoT, ZhuC,Dong X,GuX. Rehabilitationofmaxillectomy defectswithobturatorprosthesesfabricatedusing computer-aided design and rapid prototyping: a pilot study. Int J Prosthodont.2014;27:480---6.
20.AramanyMA.Basicprinciplesofobturatordesignforpartially edentulouspatients.PartII:Designprinciples.JProsthetDent. 2001;86:562---8.
21.Candel-Marti E, Carrillo-Garcia C, Penarrocha-Oltra D, Penarrocha-Diago M. Rehabilitation of atrophic posterior maxilla with zygomatic implants: review. J Oral Implantol. 2012;38:653---7.
22.Aparecida de Mattias Sartori I, Uhlendorf Y, Padovan LE, Junior PD, Melo AC, Tiossi R. Attachment-retained gingi-val prosthesis for implant-supported fixed dental prosthesis in the maxilla: a clinical report. J Prosthodont. 2014;May, http://dx.doi.org/10.1111/jopr.12159[Epubaheadofprint]. 23.MorenoMA,SkorackiRJ,HannaEY,HanasonoMM.Microvascular
freeflapreconstructionversuspalatalobturationfor maxillec-tomydefects.HeadNeck.2010;32:860---8.
24.RogersSN,LoweD,McNallyD,BrownJS,VaughanED. Health-related quality of life after maxillectomy: a comparison betweenprostheticobturationandfreeflap.JOralMaxillofac Surg.2003;61:174---81.
25.Okay DJ, Genden E, Buchbinder D, Urken M. Prosthodon-tic guidelines for surgical reconstruction of the maxilla: a classification system of defects. J Prosthet Dent. 2001;86: 352---63.
26.Mindl-MohrE.Designofa resectionprosthesiswitha hollow defectobturator.Zahntechnik(Berl).1983;24:443---50. 27.Murat S,Gurbuz A, IsayevA, Dokmez B, Cetin U. Enhanced
retentionofamaxillofacialprostheticobturatorusingprecision attachments:twocasereports.EurJDent.2012;6:212---7. 28.Sharma AB, Beumer J. Reconstruction of maxillary defects: