www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Subjective
visual
vertical
with
the
bucket
method
in
Brazilian
healthy
individuals
夽
Maristela
Mian
Ferreira
a,∗,
Fabiana
Cunha
b,
Cristina
Freitas
Gananc
¸a
c,d,
Maurício
Malavasi
Gananc
¸a
e,
Heloisa
Helena
Caovilla
faPostgraduatePrograminHumanCommunicationDisorders,CampoFonoaudiológico,EscolaPaulistadeMedicina,Universidade
FederaldeSãoPaulo(EPM-UNIFESP),SãoPaulo,SP,Brazil
bOtorhinolaryngologicalSciences,EscolaPaulistadeMedicina,UniversidadeFederaldeSãoPaulo(EPM-UNIFESP),SãoPaulo,SP,
Brazil
cSciences,EscolaPaulistadeMedicina,UniversidadeFederaldeSãoPaulo(EPM-UNIFESP),SãoPaulo,SP,Brazil
dSchoolofSpeechTherapyandAudiologySpecialization,EscolaPaulistadeMedicina,UniversidadeFederaldeSãoPaulo
(EPM-UNIFESP),SãoPaulo,SP,Brazil
eOtorhinolaryngology,EscolaPaulistadeMedicina,UniversidadeFederaldeSãoPaulo(EPM-UNIFESP),SãoPaulo,SP,Brazil fDisciplineofOtologyandNeurotology,EscolaPaulistadeMedicina,UniversidadeFederaldeSãoPaulo(EPM-UNIFESP),São
Paulo,SP,Brazil
Received24May2015;accepted26August2015 Availableonline2February2016
KEYWORDS
Ear;
Posturalbalance; Otolithicmembrane
Abstract
Introduction:Thecapacityofahealthyindividualtoestimatethetrueverticalinrelationto theEarthwhenafluorescentlineisalignedinacompletelydarkroomiscalledthesubjective visualvertical.
Objective:ToevaluatesubjectivevisualverticalusingthebucketmethodinhealthyBrazilian individuals.
Methods:Binocular subjective visual vertical was measured in 100 healthy volunteers, 50 femalesand50males.Thevolunteersindicatedtheestimatedpositioninwhichafluorescent lineinsideabucketreachedtheverticalposition.Atotaloftenrepetitionswereperformed, fiveclockwiseandfivecounterclockwise.Dataweretabulatedandanalyzedstatistically.
Results:Itwasobservedthatthehighestconcentrationofabsolutevaluesofverticaldeviation waspresentupto3◦,regardlessofgender,andtheverticaldeviationdidnotincreasewithage.
Theanalysisofthemeanoftheabsolutevaluesofdeviationsfromtheverticalof90%ofthe sampleshowedamaximumvalueof2.6◦,andattheanalysisof95%,themaximumvaluewas
3.4◦deviationfromthevertical.
夽 Pleasecitethisarticleas:FerreiraMM,CunhaF,Gananc¸aCF,Gananc¸aMM,CaovillaHH.Subjectivevisualverticalwiththebucketmethod
inBrazilianhealthyindividuals.BrazJOtorhinolaryngol.2016;82:442---6. ∗Correspondingauthor.
E-mail:[email protected](M.M.Ferreira).
http://dx.doi.org/10.1016/j.bjorl.2015.08.027
Conclusion: Thebucketmethodiseasytoperformandinterpretwhenassessingthedeviation ofthesubjectivevisualverticalinrelationtothetrueverticalinhealthyBrazilianindividuals. © 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http://
creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Orelha;
Equilíbriopostural; Membranaotolítica
Verticalvisualsubjetivacomométododobaldeemindivíduosbrasileiroshígidos
Resumo
Introduc¸ão: Acapacidadequeum indivíduohígido tememestimaraverticalverdadeiraem relac¸ãoàTerra,quandoalinhaumalinhafluorescenteemumasalacompletamenteescuraé denominadadeVerticalVisualSubjetiva(VVS).
Objetivo: AvaliaraVVScomométododobaldeemindivíduosbrasileiroshígidos.
Método: AVVSbinocularfoimedidaem100voluntárioshígidos,50dogênerofemininoe50 do masculino. Osvoluntários indicaram aposic¸ãoestimada em queuma linha fluorescente no interiordeum balde alcanc¸ou aposic¸ão vertical.Foramrealizadas 10 repetic¸ões,cinco nosentidohorárioecinconoanti-horário.Osdadosforamtabuladosesubmetidosàanálise estatística.
Resultados: Observou-sequeamaiorconcentrac¸ãodosvaloresabsolutosdosdesviosdavertical estevepresenteaté3◦,independentedogêneroeodesviodaverticalnãoaumentouconforme
aidade.Àanálisedamédiadosvaloresabsolutosdosdesviosdaverticalde90%daamostra, foiencontradoovalormáximode2,6◦eàanálisede95%ovalormáximofoide3,4◦dedesvio
davertical.
Conclusão:Ométododobaldeéfácilderealizaredeinterpretarnaavaliac¸ãododesvioda verticalvisualsubjetivaemrelac¸ãoàverticalverdadeiradeindivíduosbrasileiroshígidos. © 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http://
creativecommons.org/licenses/by/4.0/).
Introduction
The inner ear, also called the labyrinth, can be divided into anterior labyrinth, which contains the hearing organ (cochlea) and posterior labyrinth, comprising the three semicircular canals (lateral, superior, and posterior) and the vestibularsystem, which includes theutricle and the saccule.1Theinnerearvestibularsystemreceptorsconsist oftwotypesof structures:onecupula-endolymphatic sys-temin the threesemicircularcanals, sensitive toangular accelerations,andanamalgamofotolithswithina viscoelas-tic membrane at the level of the utricular and saccular macula,sensitivetolinearaccelerations.1Concomitantwith informationfromthevisualandproprioceptivesystems,the corticalotolithafferentsalsoparticipateinspatial orienta-tion,motionperception,thementalrepresentationof the bodyinspace,1andtheperceptionofverticality.2,3
Theabilitytojudgewhethertheobjectsareinthe ver-ticalpositioniscalledsubjectivevisualvertical(SVV).
Inahealthyindividual,theotolithorgansalonecan con-struct the SVV, evenin casesof deprivation of visual and proprioceptivestimuli;inunilateralvestibulardysfunction, therecoveryofSVVseemstobeassociatedwiththe possi-bilityofeffectivelyusingproprioceptiveandexteroceptive information,particularlythoseoftheplantarsurface.4
Thebucketmethod,theobjectofourresearch,was ini-tiallydesigned5andthencompared6withthesophisticated andstandardizedhemisphericdomemethod,7showingthat
thedistributionofSVVvalueswassimilarforthetwo meth-ods,thusdemonstratingthatthebucketmethodcanbecome partofroutineclinicalexaminations,asitisinexpensiveand easytoperform.
Inthedomemethod,ahemisphericdomecoveredwith coloreddotsandalineartargetisrotatedrandomlyandthe individualisinstructed toalignthetargetthroughavideo gamecontrol,makingitasverticalaspossible;inthebucket method, a bucket is rotated and the individual indicates whenafluorescentstraightlinedisplayedintheinferiorand innerpartofthebucketreachesaverticalposition.6Inthe bucketmethod,therangeofabsolutedeviationsoftheSVV valuesinrelationtothetrueverticalinhealthysubjectswas 0.9±0.7◦(mean±standarddeviation);nosignificanteffect
ofageorgenderwasidentified.6
Anotherstudyindicatedthatthebucketmethodisuseful todescribespatialdeficitsinpatientswithprovenvestibular disorder,butnotasascreeningtest.In50healthysubjects, themean(standarddeviation,minimum/maximum)ofthe absolutevaluesofverticaldeviationwas1.2◦(0.7;0◦/3.2◦)
forfemales;and1.0◦(0.8;0◦/2.7◦)formales.8
InBrazil,SVVwasevaluatedin30healthyBrazilian indi-vidualsby adjusting a virtual line in the verticalposition withacomputermouse,projectedonawhitescreen.The meandeviationofSVVwas−0.372◦±1.21;representingsix
repetitions.9
fluorescentlight,positionedinfrontoftheindividualsandat theleveloftheireyes.Theassessedindividualsworeglasses withlight-filteringlensesthatmadeanyothervisual affer-entinformationimpossible,withtheexceptionofthe fluo-rescentlight,perceivedasagreenline.TenSVVadjustments weremade,oneforeachside,totalingfiveintheclockwise andfiveinthecounterclockwisedirection.Theangular incli-nationsofthevertical positionweremeasured indegrees anddefinedaspositivefor clockwiseandnegativeforthe counterclockwisedeviations,inrelationtothepatient.The resultsofSVVshowedthemeanvaluesoftenadjustments, rangingbetween−2.0◦and+2.4◦(mean=0.18,SD=0.77).10 Severalstudieshaveshowntheimportanceofvestibular assessmentbySVVwithdifferentmethods,andalsowiththe bucketmethod.However,toapplythismethodinBrazil,it isimportanttoknowthebehaviorofhealthyBrazilian indi-viduals,forsubsequentcomparisonwithpatientswhohave vestibulardisorders.Consideringthesemiological valueof theSVVassessmentandthescarcityofnationalstudiesusing thebucketmethod,whichisinexpensiveandeasytoapply, itwasdecidedtoperformthisinvestigation.
The objectiveof thisstudywastoassesstheSVV using thebucketmethodinhealthyBrazilianindividuals.
Methods
This study wasperformed after approval by the Research Ethics Committee of the institution under protocol No. 51439/12.
Thesampleofthiscross-sectionalstudyconsistedof100 healthy adult volunteer individuals from the community, 50females and50males,withnocomplaintsofvestibular disorders and/or hearing loss; individuals with cognitive impairment,severevisualacuityalteration,andhistoryof neurologicaldiseasewereexcluded.
The SVV evaluation wasperformed using a bucket, as wellasinexpensiveandeasilyacquiredmaterials:anopaque plasticbucket,withaborderlargerthan25cm,cardboard, string,fluorescenttape,weights(screwnuts),andadhesive tape.Apieceoffluorescenttape,placedverticallyonthe innersideofthebottomofthebucket,wasperfectlyaligned withthezeromarkofaprotractorpositionedontheexternal andinferiorpartofthebucket,andbothwerealignedwith thetrueverticalinrelationtotheEarth11 (Figs.1and2).
The SVV wasmeasured binocularly. The healthy volun-teerswere asked to look at a fluorescent line inside the bucket,inthesittingposition,withtheirheadsup6(Fig.3). Insomecases,whenitwasimpossibleforthevisualfieldto becompletelyinsidethebucket,thevolunteer’sheadand thebucketwerecoveredwithadarkclothtopreventvisual cues(Fig.4).
To measure the SVV, thebucket wasrandomly rotated by the examiner, to exclude possible tactile cues, in the clockwiseorcounter-clockwisedirections,toafinalposition around15◦,andthenslowlyrotatedtowardthezerodegree
position.The volunteers indicated the estimated position where thefluorescent line hadreached the vertical posi-tion,asking the examiner to stop moving the bucket, by saying‘‘stop’’.Tenrepetitionsoftheprocedurewere per-formed,fiveintheclockwiseandfiveintheanti-clockwise direction;theidentifiedvalueswererecordedinthedegree
Figure1 Viewofthefluorescenttapeonthebottomofthe insideofthebucket.
Figure2 Viewoftheoutsideandbottomofthebucket.
scale on the outside of the bucket. The angular inclina-tionsoftheverticalpositionweremeasuredindegreesand definedaspositivedeviationsintheclockwiseandnegative intheanti-clockwisedirection,inrelationtothevolunteer. Theprocedurewasrepeatedwhentheexaminermovedthe buckettoofast,withoutgivingthepatientenoughtimefor theresponse.
Figure3 Applyingthebucketmethod.
Figure4 Applyingthebucketmethodusingadarkcloth.
(˛=0.05)andSPSSv.19forWindowsandOfficeExcel2007
wereusedinthestatisticalanalysis.
Results
Atotalof100healthyvolunteerswasevaluated,50females and50males,agedbetween18and59years,withno com-plaintsofvestibulardisordersand/orhearingloss.
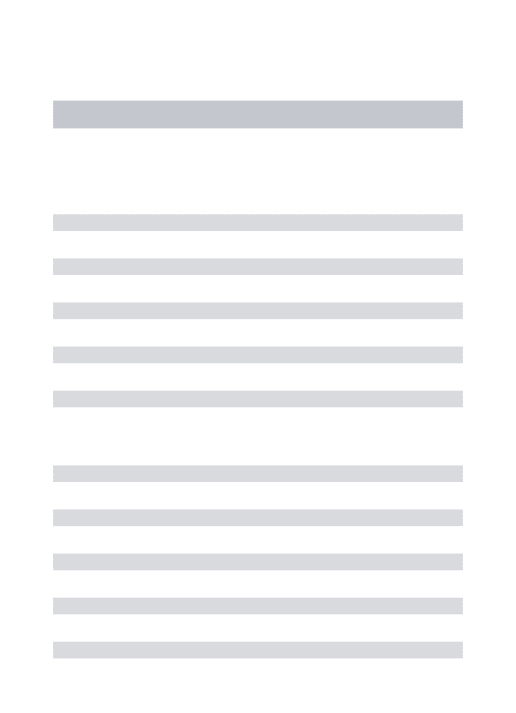
Table1showsthemean,median,standarddeviation,and minimumandmaximumvaluesofthemeanoftheabsolute valuesofdeviationsfromtheverticaloftenrepetitionsin the50femaleandmalevolunteers.
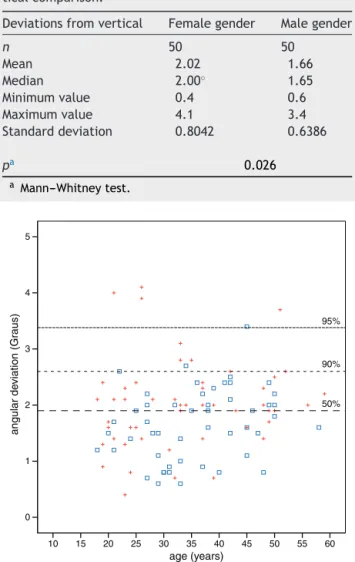
Fig.5representsthemeanoftheabsolutevaluesof devi-ationsfromtheverticalregardingageandgender.Itcanbe observed that the highest concentrationof values can be found upto3◦ of verticaldeviation,regardless ofgender,
Table1 Measurements---summary ofabsolute valuesof deviationsfromthevertical,accordingtogenderand statis-ticalcomparison.
Deviationsfromvertical Femalegender Malegender
n 50 50
Mean 2.02 1.66
Median 2.00◦ 1.65
Minimumvalue 0.4 0.6
Maximumvalue 4.1 3.4
Standarddeviation 0.8042 0.6386
pa 0.026
a Mann---Whitneytest.
angular de
viation (Gr
aus)
age (years) 5
4
3
2
1
0
10 15 20 25 30 35
95%
90%
50%
40 45 50 55 60
Figure5 Two-dimensionalscatterplotandthe50%,90%,and 95%percentilesofthemeanoftheabsolutevaluesofdeviations fromthe vertical (degrees)andtheage (years) accordingto gender(+female/male).
andthattheverticaldeviationdoesnotincreasewithage. Theanalysisofthemeanoftheabsolutevaluesofdeviations fromtheverticalof90%ofthesampleshowedamaximum valueof2.6◦ andthe95%analysisfoundamaximumvalue
of3.4◦ofdeviationfromvertical.
Discussion
SVVassessmentisasimpletechniquetostudyotolith func-tion,asthe inclinationofthe fluorescentline beyondthe valuesconsidered tobe normal is the most sensitive sign of vestibularsystem dysfunction; the buckettest is inex-pensiveandeasytoperform;theanalysisof theresultsis simple,thetestisfastandreliable,anditcanbeapplied anywhere,warrantingitsbroaduse.6
ofdeviations fromthevertical infemale andmale volun-teers,similartopreviousreportsintheliterature.8
Theoriginalstudyusingthebucketmethoddidnot iden-tify an effect of gender and age on the deviation from the vertical.6 However, according to the two-dimensional scatterplotgraph,thesamplecanbeconsidered homoge-nousregardinggenderandage,andwhen90%ofthesample wasanalyzed,thevalueswerefoundupto2.6◦,or
approxi-mately3◦,asthebucketmethodidentifiesangulardeviation
valuesinwholenumbers.Thevalueof2.6◦issimilartothe
valueof 2.3◦ found in theoriginal study usingthebucket
method.6 Another study,12 assessing the performance of healthy elderly individuals, adopted a deviation of 3◦ as
thenormallimit,similartothatofthepresentstudy,also making an approximation of the standard values used as reference.6
The SVV was evaluatedin healthy Brazilian individuals through other methods that identified values similar to that found in this study; the mean deviation from SVV was−0.372±1.21◦ withthemethodthatusedacomputer
mousetoadjustavirtualline inthevertical position pro-jected on a white screen,9 and it ranged between
−2.0◦
and+2.4◦ inanotherstudythatusedaportablestickwith
fluorescentlight.10
As previously noted,6,13 the authors also believe that an easy-to-perform and easy-to-interpret SVV evaluation shouldbeincludedinroutineclinicalvestibulartests,asit canprovideinformationontheotolithorganfunctionand also can monitor changes and responses to treatment in patientswithcentralorperipheralvestibulardisorders.
TheaimofthisstudywastoevaluateSVVusingthebucket methodinhealthyBrazilianindividualswithnoauditoryand vestibularcomplaints. It is hoped that these findings uti-lizing this method may be useful in clinical practice and infuture studies,in orderto help characterize vestibular systemdysfunctioninpatientswithbodybalancedisorders.
Conclusion
Thebucketmethodiseasytoperformandinterpretwhen evaluatingthedeviationoftheSVVinrelationtotrue ver-ticalinhealthyBrazilianindividuals.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.MaiaFCZ.Elementospráticosemotoneurologia.2nded.Riode Janeiro:Revinter;2011.
2.AnastasopoulosD,BronsteinAM.Acaseofthalamicsyndrome: somatosensoryinfluencesonvisualorientation.JNeurol Neu-rosurgPsychiatry.1999;67:390---4.
3.SchwarzU. Neuroophthalmology: a brief Vademecum.Eur J Radiol.2004;49:31---63.
4.Faralli M, Longari F, Ricci G, Ibba MC, Frenguelli A. Influ-ence of extero and proprioceptive afferents of the plantar surfaceindeterminingsubjectivevisualverticalinpatientswith unilateral vestibular dysfunction. Acta Otorhinolaryngol Ital. 2009;29:245---50.
5.FrisénL.Practicalestimationofoculartorsionandsubjective vertical.Neuro-ophthalmology.2000;23:195.
6.Zwergal A, Rettinger N, Frenzel C, Dieterich M, Brandt T, Strupp M.A bucket of static vestibular function.Neurology. 2009;72:1689---92.
7.Dieterich M, Brandt T. Ocular torsion and tilt of subjec-tivevisualverticalaresensitivebrainstemsigns.AnnNeurol. 1993;33:292---9.
8.Cohen HS, Sangi-HaghpeykarH. Subjective visual vertical in vestibular disorders measured with the bucket test. Acta Otolaryngol.2012;132:850---4.
9.Pavan TZ, Funabashi M, Carneiro JA, Pontelli TE, Tedeschi W,Colafêmina JF,etal.Softwareforsubjective visual verti-calassessment:anobservationalcross-sectionalstudy.BrazJ Otorhinolaryngol.2012;78:51---8.
10.Kanashiro AMK, Pereira CB, Maia FM, Scaff M, Barbosa ER. Avaliac¸ãodaverticalvisualsubjetivaemindivíduosbrasileiros normais.ArqNeuropsiquiatr.2007;65:472---5.
11.Cook J. SVV Bucket construction (last edited 2010-05-05 09:14:00byJamesCook),UniversityofPittsburgh.
12.Davalos-Bichara M, Agrawal Y. Normative results of healthy olderadultsonstandardclinicalvestibulartests.OtolNeurotol. 2014;35:297---300.