www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Surveillance
of
bacteria
Pseudomonas
aeruginosa
and
MRSA
associated
with
chronic
suppurative
otitis
media
夽
Sibanarayan
Rath
a,
Saumya
Ranjan
Das
b,
Rabindra
Nath
Padhy
a,∗aSiksha‘O’AnusandhanUniversity,InstituteofMedicalSciences&SumHospital,CentralResearchLaboratory,KalingaNagar,
Odisha,India
bSiksha‘O’AnusandhanUniversity,InstituteofMedicalSciences&SumHospital,DepartmentofENT,KalingaNagar,Odisha,India
Received12December2015;accepted11March2016 Availableonline22April2016
KEYWORDS
Chronicsuppurative otitismedia;
Pseudomonas aeruginosa; MRSA; Intracranial complications
Abstract
Introduction:Suppurativeotitismediaisacriticaldiseasecausingperforationofthetympanic membraneassociatedwithchangesofthemucoperiosteumofthemiddleearcleft.
Objective: Toisolatecausativebacteriafromchronicsuppurativeeardischargesandto ascer-taintheirantibioticprofiles,ofpatientsattendingoutpatientsdepartmentin3years.
Methods:Forisolationofbacteria,samplesofeardischargesweregrowninsuitablemediaand bacteriaweresubjectedtoantibioticprofilingbytheKirby---Bauer’smethodwithpresentlyused antibiotics.
Results:Atotalof1043bacteriawereisolated,includingPseudomonasaeruginosaand methi-cillinresistantStaphylococcusaureus,alongwith121fungalisolates.Among371P.aeruginosa
isolates,tobramycin30hadthehighestsusceptibilityrate93.2%,followedbyceftazidime30, 91.5%andamikacin10g/disk64.4%.Of359S.aureusisolates,therewere236coagulase neg-ative S.aureus+methicillin sensitiveS.aureus isolates,while123isolates weremethicillin resistantStaphylococcusaureuswith95.2%isolatessusceptibletocloxacillin15,83.3%isolates toerythromycin15and78.5%isolatestogentamicin30g/disk.Of1164,49patientspresented postauralabscess,12patientshadintracranialcomplications,9patientshadfacialpalsyand3 patientshadlabyrinthitis.Morethan90%P.aeruginosaand90%S.aureusisolatesweresensitive totobramycin30andcloxacillin30g/disk,respectively.
夽 Pleasecitethisarticleas:RathS,DasSR,PadhyRN.Surveillanceofbacteria
PseudomonasaeruginosaandMRSAassociatedwithchronic suppurativeotitismedia(CSOM).BrazJOtorhinolaryngol.2017;83:201---6.
∗Correspondingauthor.
E-mail:[email protected](R.N.Padhy).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.03.008
Conclusion:Multidrug resistant strains of P.aeruginosa were more prevalent than thoseof
S.aureus ineardischarges. Tobramycinandcloxacillinmay beincludedinthe formulatory antibioticregimentoovercomebacterialinfectionsinchronicsuppurativeotitismedia. © 2017 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http://
creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Otitemédiacrônica supurativa;
Pseudomonas aeruginosa; MRSA; Complicac¸ões intracranianas
VigilânciadebactériasPseudomonasaeruginosaeMRSAassociadasàotitemédia crônicasupurativa
Resumo
Introduc¸ão:Otitemédiasupurativaéumadoenc¸aimportantequecausaperfurac¸ãoda mem-branatimpânicaalémdealterac¸õesdomucoperiósteodaorelhamédia.
Objetivo:Isolarasbactériascausadorasapartirdasecrec¸ãoauricularcrônicaeverificarseus perfisdesensibilidadeaosantibióticosempacientesambulatoriaisdurantetrêsanos.
Método: Paraoisolamentodasbactérias,asamostrasdesecrec¸õesauricularesforamcultivadas emmeiosadequadoseasbactériasforamsubmetidasàdetecc¸ãodeperfisdesensibilidadeaos antibióticosusandoométododeKirby-Bauerparaantibióticosusadosnaatualidade.
Resultados: Nototal,1.043bactérias,incluindoPseudomonasaeruginosaresistentesà meti-cilinaeStaphylococcusaureus,e121fungosisoladosforamidentificados.Entre371isolados deP.aeruginosa,tobramicina30g/discoapresentouamaiortaxadesusceptibilidade(93,2%), seguidaporceftazidima30g/disco(91,5%)eamicacina10g/disco(64,4%).De359isolados deS.aureus,236eramS.aureuscoagulase-negativos+S.aureussensíveisàmeticilina(MSSA), enquanto123eramMRSAcom95,2%desuscetibilidadeàcloxacilina15g/disco,83,3% sen-síveisàeritromicina15g/discoe78,5% àgentamicina30g/disco.Entre1.164 pacientes, 49apresentaramabscessoaural,12apresentaramcomplicac¸õesintracranianas,nove apresen-taramparalisiafacialetrêsapresentaramlabirintite.Maisde90%dasP.aeruginosaisoladas e de 90%de S. aureus eramsensíveis àtobramicina 30g/disco e cloxacilina30g/disco, respectivamente.
Conclusão:CepasmultirresistentesdeP.aeruginosaforammaisprevalentesqueasdeS.aureus
nassecrec¸õesauriculares.Tobramicinaecloxacilinapodemserconsideradasnaformulac¸ãode regimedeantibióticosparatratarasinfecc¸õesbacterianasnaOMCS.
© 2017 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http://
creativecommons.org/licenses/by/4.0/).
Introduction
The generic term,‘otitismedia’ includes widely,casesof ‘acuteotitismedia’(AOM) andcasesof‘otitismediawith effusion’(OME);basicallythesearenon-suppurative. More-over, ‘chronic otitis media’(COM)is the gathering of pus fromsuppurationswheninfectionsarechronic;eventually, chronic suppurative otitis media (CSOM) are with inflam-mationandtheproductionofpus.1Additionally,CSOMmay
remaininactivewiththepotentialtobeactiveoccasionally, leadingtoaperforationofthetympanicmembrane associ-atedwithchangesofthemucoperiosteumofthemiddleear cleft with/without mucoid or mucopurulent otorrhea.1---3
It takes usually 2 or 3 weeks or more duration, for the diseasetoberecognizedasactive.AhealedCOMmayhave permanent abnormalities of the pars tensa; but with an intact pars tensa the occurrence of COM is rare.3 CSOM
could lead to hearing loss, intermittent otalgia causing psychologicaltrauma.InCSOM,themostcausativebacteria are Klebsiella sp., Proteus sp., Pseudomonas aeruginosa andStaphylococcusaureus.4Andotherbacteriacommonly
isolatedfrompatients withAOMareHaemophilus influen-zae,MoraxellacatarrhalisandStreptococcuspneumonia.5
Moreover, P. aeruginosa had been seen as a notorious pathogeninthishospitaltoo.6Mainlyfoundinwoundsand
urinarytract,itfindswaysasbloodstreaminfection(BSI)to innardscausingcomorbidities.7Indeed,theabilityofthese
organisms to form biofilm that may contribute to their frequencyinCSOM.8Asitisknown,therateofinvasionofa
pathogenicbacteriumdirectlydependsonitslevelofdrug resistance,apartfromimmune-conditionsofpatients.9
Particularly, several clonal variants of S. aureus were resistanttothepenicillingroupofantibiotics,afterwhich methicillin/oxacillinwereintroducedfor thecontrol. Sub-sequently, methicillin resistant S. aureus (MRSA),causing surgical site infections and wound emerged.10 The most
ticarcillin-clavulanicacid,piperacillin-tazobactamandthe carbapenem,imipenem.Thus,MRSAisolatesareMDRtoo.11
Moreover,themostdominatingfungalspecieswereof Can-didaandAspergillusalongwithMRSA;andinasurveillance, 50% patients were diagnosed with candidiasis.10 Indeed, Candidaalbicanswasoriginallyaharmlessfungusinhealthy persons,butitscausessuperficialtolife-threatening uncon-trollable systemic infections due to the emergence of antifungalresistance.12
This workdescribes surveillanceofbacterialflorafrom eardischargesofpatientsattendingtheOutpatients Depart-ment(OPD)ofENTdepartmentofthehospital,inthelast 3 years.And the cited twofungi were too isolatedalong withbacteria.Antibiogramsofisolatedbacterialtaxawere determinedtoassessthespectrumofCSOMthatwouldhelp in rescheduling antimicrobial stewardship program of the hospitalorthezoneofcentralOdisha.
Methods
A total of 1230 pus discharges from clinically diagnosed CSOM cases were collected, during January 2012 to Jan-uary2015 withsterile cottonswabsticks. Pusswabs were cultured on blood and MacConkey agar plates that were incubatedat37◦Covernightforpathogenicbacteria,which were identified according to the standard method used for bacteria and concomitantly for fungi.6,13,14 Antibiotic
susceptibilitytestsofisolatedbacteriaweredone accord-ing to Clinical Laboratory Standard Institute guidelines, as described.15,16 Standard antimicrobial disks (HiMedia,
Mumbai) used for S. aureus were, oxacillin, cotrimoxa-zole, penicillin, cloxacillin, gentamicin, chloramphenicol, ciprofloxacinandvancomycin;similardisksusedforP. aeru-ginosa were gentamicin, chloramphenicol, ciprofloxacin, ceftazidime,piperacillin,carbenecillinandtobramycin.
AntibioticsensitivityanddetectionofMRSA
ThestandardMTCCnumber7443strainandalltheisolated S. aureus strains were subjected to antibiotic sensitivity
tests with antibiotics, by the Kirby-Bauer’s method (disk diffusion)detailedpreviously.11ForthedetectionofMRSA,
chromogenicagar media test wasused; pure clinical iso-lates of S. aureus were streaked onto MRSA-agar media asdescribed.11Muller-HintonAgar(MHA)plateswere
incu-batedat37◦Cfor18handinhibition-zonediameterswere measured. A value of inhibition-zone diameter less than 22mmwasreportedasoxacillinresistantandthatmorethan 21mmwasconsideredasoxacillinsensitive.11
Identificationoffungi
Direct microscopic examination of the cotton swab with sampleswascarried outby mounting sample lots treated with 1---2 drops of 10---20% KOH for 15---30min. Each specimen-lot was inoculated on two sets of Sabouraud’s dextrose agar slopes, one set with chloramphenicol and the other set with cycloheximide (chloramphenicol ---0.05mg/mL, cycloheximide --- 0.5mg/mL). Cultures were incubated at room temperature for 4---6 weeks and were observedregularlyforpossiblegrowth.Fungalisolateswere identifiedon the basis of duration of growth and surface morphologyof colonies,aswell aspigment production on thereverseandmicroscopicexaminationofhyphaeinlacto phenolcottonbluepreparation.6,16
Results
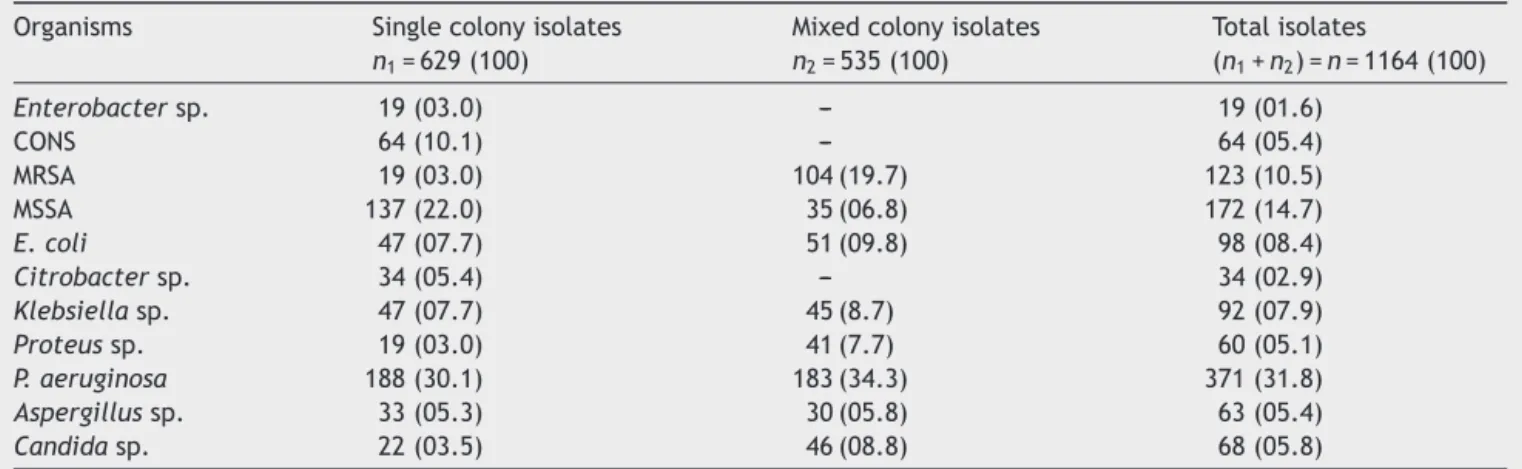
From 1230 collected samples, 1164 bacterial and fungal coloniesgrewas629singleand535mixedcoloniesonagar platesandnomicrobial growthwasseenwith66samples. Therewere1043bacterialand121fungalisolatesintotal. The most common causal bacteria isolated were 220 iso-latesof S. aureus withand 188 isolatesof P. aeruginosa; and 19 isolates of S. aureus were MRSA, and 64 isolates werecoagulasenegativeS.aureus(CONS).Bacteria,P. aeru-ginosawasisolatedin 183 of thetotal 1164 samplesthat yieldedmixedcoloniesofS.aureus,Klebsiellasp.and Pro-teussp.,followedbyEscherichiacoli,giveninTable1.Fungi accountedfor63isolatesofAspergillussp.and68isolates
Table1 GrowthofbacteriaandfungiinculturesofeardischargesamplesofOPDpatientswithCSOMassinglecolonyand mixedcolonies.
Organisms Singlecolonyisolates
n1=629(100)
Mixedcolonyisolates
n2=535(100)
Totalisolates
(n1+n2)=n=1164(100)
Enterobactersp. 19(03.0) --- 19(01.6)
CONS 64(10.1) --- 64(05.4)
MRSA 19(03.0) 104(19.7) 123(10.5)
MSSA 137(22.0) 35(06.8) 172(14.7)
E.coli 47(07.7) 51(09.8) 98(08.4)
Citrobactersp. 34(05.4) --- 34(02.9)
Klebsiellasp. 47(07.7) 45(8.7) 92(07.9)
Proteussp. 19(03.0) 41(7.7) 60(05.1)
P.aeruginosa 188(30.1) 183(34.3) 371(31.8)
Aspergillussp. 33(05.3) 30(05.8) 63(05.4)
Candidasp. 22(03.5) 46(08.8) 68(05.8)
Figure1 (A)ConfluentgrowthandisolatedgreencoloniesofP.aeruginosaonnutrientagarplate;and(B)methicillinresistant colorlesscoloniesofS.aureus(MRSA)onbloodagarplate.
Tobramycin PiperacillinCarbe necillin
Cefotaxin Ciprofloxacin
Amikacin
Sparfloxacin Ceftazidime C eftríaxon
Gentamyc in 100
90 80
70 60
50 40
30 20
10 0
Resistant Sensitive
Figure2 AntibiogramofP.aeruginosa.
ofCandidasp.asbothsingleandmixedcoloniesfrom1164 growth-yieldingsamples,giveninTable1.
Antibiograms of the most common bacteria, P. aeru-ginosa and S. aureus (other than MRSA) are depicted
in Fig. 1. Among P. aeruginosa, tobramycin 30g/disk had the highest susceptibility rate as 93.2%, followed by ceftazidime 30g/disk 91.5% and amikacin 10g/disk 64.4%, given in Fig.2. And95.2% S. aureus isolates were
Sensitive Resistant
Cloxacil lin
Ampicillin Cepha
lexin Penicillin
Tetracycli ne
Chloramp henicol
Gentamycin Cotri
mox azole
Erythomycin Ciprofloxacin
100
90
80
70
60
50
40
30
20
10
0
Table2 Numbersofgrowingorganismsfromculturesofeardischargesamplesinpatientswithcomplicatedanduncomplicated CSOM.
Typesoforganisms ComplicatedCSOM UncomplicatedCSOM Total
Assinglecolony 48(0.05) 581(0.49) n1=629(0.54)
Asmixedcolonies 25(0.02) 510(0.43) n2=535(0.45)
Total 73(0.06) 1091(0.94) n=1164(100)
SeenoteofTable1.
Table3 NumbersofpatientswithcomplicationsascomorbiditiescausingCSOMin3years.
Year Facialpalsy Intracranialcomplication Post-auralabscess Labyrinthitis Total
2012 3 3 16 2 24
2013 2 4 18 0 24
2014 4 5 15 1 25
Total 9(12.9) 12(16.6) 49(67.1) 3(3.3) 73(100)
Percentvaluesareinparenthesis.
susceptible to cloxacillin 15g/disk, followed by 83.3% isolates to erythromycin 15g/disk and 78.5% isolates to gentamicin 30g/disk, given in Fig. 3. All MRSA isolates wereMDR;however,none ofthoseisolateswereresistant tovancomycin30g/disk.
Of samples of 1164 patients, 73 had complicated and 1091 patients haduncomplicated CSOM, asdetailed:only 48caseshadassinglebacteriumisolatedasasinglecolony, whiletheremaining198caseshadtwoormorebacteria iso-latesasmixedcolonies,giveninTable2.Ofthetotal1230 patients,49hadpostauralabscess,12patientshad intracra-nial complications, 9 patients presented with facialpalsy and3patientpresentedwithlabyrinthitis,giveninTable3. Furthermore, it was seen that the trend of intracranial complications was gradually decreasing while intracranial complicationswere inan increasingtrend,although there was no significant change in overall incidences of CSOM. From 359 S. aureus samples, a total of 123 MRSA strain-sand236strainsof‘CONS+(MSSA)’(methicillinsensitiveS. aureus)strains,asbothsingleandmixedcolonies.The min-imuminhibitoryconcentration(MIC)rangeagainstoxacillin was16---512g/mL,theMICrangewas1---4g/mL,forMRSA and‘CONS+MSSA’.TheseMICvaluesconfirmedthepresence of MRSAstrains, asthe breakpoint for being resistant to oxacillinwas≥4g/mL,giveninTable4.
Discussion
CSOMisadiseaseassociatedwiththestructuralchangein middleear;andpermanentabnormalityofparstensaorpars flaccid,mostly occur assequelae of long standingmiddle ear effusion, inadequately treated AOM, eustachian tube dysfunctionor evenfroma negativemiddle earpressure. Inthe developingcountries,poverty,ignorance,dearthof specialistsandlimitedaccesstomedicalcareamongst oth-ers conspire toworsen the occurrence and complications of CSOM17; poor living conditions, poor access to
medi-cal care, inadequate medicaltreatment, recurrent upper respiratory tract infections and nasal diseases have been recognizedasrisk factorsforCSOM.18 Atticoantral disease
mostcommonly isinvolvedwiththeparsflaccidaand pos-teriorsuperior quadrant of pars tensa. Itis characterized bythe formation of aretractionpocket in which,keratin anddesquamatedepithelial debrisaccumulatetoproduce cholesteatoma;eventuallyitisconsideredtobea danger-ous form of the disease because of the development of severalintracranialandextracranialcomplications.18
More-over,staphylococciareapartofthenormalflora,butthose remain invasive causing a variety of body infections. S. aureus is the most notorious nosocomial pathogen and in communitytoo.11
AlthoughtheclinicalrelevanceofCONSisstill controver-sial,patients at riskof CONS infectionsinclude neonates,
Table 4 Detection of MRSA and ‘CONS+MSSA’ isolates basedonMICvaluesduetooxacillinina12×8micro-titer
plate.
Well Oxacillin (g/mL)
Numberofisolates
MRSA=123 CONS+ MSSA=236
1 0 123 236
2 ≤0.25 ---
---3 0.5 ---
---4 1 --- 83
5 2 --- 75
6 4 --- 78
7 8 ---
---8 16 23
---9 32 26
---10 64 27
---11 128 29
---12 ≥256 28
thosewithintravascular catheters,prostheticdevicesand surgical wounds in immune-compromised individuals. The remarkableabilityofS.aureusandCONStoacquire antibi-otic resistance limits therapeutic options, attended with high rates of morbidity and mortality, including costs of hospitalization.19 Particularly,several clonalvariantsof S. aureusandMRSAwerereportedresistant tothe penicillin group of antibiotics, methicillin/oxacillin. Moreover, in a German study, it was reported that a majority of MRSA strainswerefromwoundinfections(56.9%),with pneumo-niacasesbeingthesecondmostcommon(21.0%),followed byBSI(15.1%).11
Conclusion
MDRstrainsofP.aeruginosaandMRSAweremostprevalent iseardischargesofpatientswithCSOM.Ofthetotal1164, 49patients presented post auralabscess,12 patientshad intracranialcomplications,9patientshadfacialpalsyand3 patientshadlabyrinthitis.Thisstudyrevealedciprofloxacin as less effective in the treatment of active CSOM, and tobramycinandcloxacillincouldpreferablybeusedtotreat CSOM.
Funding
Thisworkwassupported bythemajorresearchprojectn◦ BT/PR8214/PBD/17/863/2013onbacterialinfections,from Department of Biotechnology (DBT), Govt. of India, New Delhi, awarded to RN Padhy. This work is a part of PhD thesisofSNRath,aJRFintheDBTproject,in Biotechnol-ogyof S‘O’A University,Bhubaneswar. We are grateful to Prof.RankanidhiSamal,forcriticalappreciationand thank-fultoProf.GangadharaSahoo,Dean,IMSandSumHospital, Bhubaneswar,forextendedfacilities.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Berman S. Otitis mediain children. NEngl JMed. 1995;23: 1560---5.
2.Browning GG, Merchant SN, Kelly G, Swan IR, Canter R, McKerrow SW. Chronic otitismedia. Scott-Brown’s otorhino-laryngologyheadandneck,vol.19.EdwardArnoldLtd.;2008. p.3406---10.
3.AfolabiOA,FadareJO,OmokanyeHK,OlatokeF,OdiTO,Saka MJ, et al. Socioeconomic challenges of chronic suppurative otitismedia management in state tertiary health facility in Nigeria.EgyptJEarNoseThroatAlliedSci.2014;15:17---22. 4.CouzosS,LeaT,MullarR.Effectivenessofototopicalantibiotics
for CSOM in Aboriginal children, a community based multi-centerdoubleblindrandomizedcontrolledtrial.MedJAust. 2003;4:185---90.
5.Bluestone CD,KleinJO. In:Bluestone CD,Klein JO,editors. Otitis media in infants and children. Microbiology. 3rd ed. Philadelphia,PA:WBSaunders;2001.p.79---101.
6.SahuMC,PadhyRN.Bayesianevaluationoftwoconventional diagnosticmethodsforpathogenic fungalinfections.JAcute Med.2014;4:109---19.
7.AskarianM,HossseiniR,KheirandishP.Incidenceandoutcome ofnosocomialinfectionsinfemaleburnpatientsinShiraz,Iran. AmJInfectControl.2004;32:23---6.
8.AhmedB,HydriAS,EjazA,FarooqS,ZaidiSK,AfridiAA. Micro-biologyofear dischargeinQuetta.JCollPhysicianSurgPak. 2005;15:583---4.
9.Giamarellos-Bourboulis EJ, Papadimitriou E, Galanakis N, AntonopoulouA,TsaganosT,KanellakopoulouK.Multidrug resis-tance to antimicrobials as a predominant factor influencing patientsurvival.IntJAntimicrobAgent.2006;27:476---81. 10.WisplinghoffH, BischoffT, TallentSM,Seifert H,Wenzel RP,
EdmondMB.Nosocomialbloodstream infectionsinUS hospi-tals:analysisof24,179cases from a prospectivenationwide surveillancestudy.ClinInfectDis.2004;39:309---17.
11.DubeyD,Rath S,SahuMC, PatnaikL,DebataNK,Padhy RN. Surveillanceofinfectionstatusofdrugresistant Staphylococ-cusaureusinanIndianteachinghospital.AsianPacJTropDis. 2013;3:133---42.
12.RichardsonM,LasseFlorlC.Changingepidemiologyofsystemic fungalinfections.ClinMicrobiolInfect.2008;14:5---24. 13.RathSN,PadhyRN.Surveillanceofacutecommunityacquired
urinarytractbacterialinfections.JAcuteDis.2015;3:186---95. 14.PrajnaL,Vijayakumar A.Atlas offungalcornealulcers
clini-calfeaturesandlaboratoryidentificationmethods.NewDelhi: JaypeeBrothMedPublishers;2008.
15.ClinicalandLaboratoryStandardsInstitute.Performance stan-dardsforantimicrobialsusceptibilitytesting.PA:Wayne;2011. 16.Rath SN,Panda M,Sahu MC,Padhy RN. Bayesiananalysisof twodiagnosticmethodsfor paediatricringworminfectionsin ateachinghospital.JMycolMéd.2015;25:191---9.
17.VikramBK,KhajaN,UdayashankarSG.Clinico-epidemiological studyofcomplicatedanduncomplicated chronicsuppurative otitismedia.JLaryngolOtol.2008;122:226---42.
18.ChowdhuryMA,AlauddinA.Comparativestudybetween tubo-tympanic and atticoantral type of chronic suppurativeotitis media.BangladeshMedResCouncBull.2002;1:36---44. 19.Zong Z, Peng C, Lu X. Diversity of SCCmec elements in