w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Haptoglobin
gene
polymorphisms
and
interleukin-6
and
-8
levels
in
patients
with
sickle
cell
anemia
Bruna
Spinella
Pierrot-Gallo,
Perla
Vicari,
Sandra
Satiko
Matsuda,
Samuel
Ademola
Adegoke,
Grazielle
Mecabo,
Maria
Stella
Figueiredo
∗UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received4May2015 Accepted3July2015 Availableonline31July2015
Keywords:
Haptoglobinpolymorphism Genotype
Interleukins Sicklecellanemia
a
b
s
t
r
a
c
t
Background:Haptoglobingenotypes,andinterleukin-6and-8participateinthe pathophysi-ologyofsicklecellanemia.Theexpressionofcytokinesisregulatedbygeneticmechanisms howevertheeffectofhaptoglobinpolymorphismsonthesecytokinesisnotfullyunderstood. Thisstudyaimedtocomparethefrequencyofhaptoglobingenotypesandtheinterleukin-6 and-8concentrationsinsicklecellanemiapatientsandcontrolstoinvestigatethe associ-ationbetweenhaptoglobingenotypesandcytokinelevels.
Methods:Sixtysicklecellanemiapatientsand74healthyindividualswereanalyzed. Hap-toglobin genotypes were determined bymultiplex polymerase chainreaction, and the interleukin-6and-8levelsbyenzymelinkedimmunosorbentassay.Theassociationbetween haptoglobingenotypesandcytokineswasinvestigatedbystatisticaltests.
Results:Hp2-1wasthemostcommongenotypeinboththecasesandcontrolswhile Hp1-1waslessfrequentamongsicklecellanemiapatients.Interleukin-6and-8levelswere higherinpatientsthancontrols(p-value<0.0001).Therewasnosignificantdifferencein interleukin-6and-8concentrationsbetweenthegenotypes(p-value>0.05).Asimilartrend wasobservedamongthecontrols.
Conclusion: Although,levelsofinterleukin-6and-8werehigherinthesicklecellanemia patients,theyappearednottoberelatedtothehaptoglobingenotypes.Further investiga-tionsarenecessarytoidentifyfactorsresponsibleforincreasedsecretionoftheinterleukin-6 and-8pro-inflammatorycytokinesinpatientswithsicklecellanemia.
©2015Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.Allrightsreserved.
Introduction
Sickle cell anemia (SCA) is the most common hereditary monogenicdiseaseinBrazil,wheretheprevalenceofthetrait
∗ Correspondingauthorat:DisciplinadeHematologiaeHemoterapia,EscolaPaulistadeMedicina(EPM),UniversidadeFederaldeSão
Paulo(UNIFESP),RuaDr.DiogodeFaria,824,3◦andar,VilaClementino,04037-002SãoPaulo,SP,Brazil.
E-mailaddress:[email protected](M.S.Figueiredo).
inthegeneralpopulationis2–8%andtheestimatednumber ofaffectedindividualsisabout7.2million.1Sicklehemoglobin
(Hb S)iscausedbya mutationofasingle nucleotide(HBB glu(E)6Val(A);GAG>GTG;rs334;HBB:c.20A>T;MIM:#603903)2
inthebetaglobingene,whichresultsinglutamicacidbeing
http://dx.doi.org/10.1016/j.bjhh.2015.07.006
substitutedbyvalineatposition6ofthebetaglobin chain. Thischange leadstoHbSpolymerization,especiallyunder lowoxygentension.3
PatientswithSCAsufferfromacuteandchronicvascular occlusionduetopolymerizationofHbSinredcells.Vascular occlusionisamajorpathophysiologiceventinSCA,leading tovarietyofmorbidities suchaspainfulcrisis, acutechest syndrome, stroke, aseptic necrosis of bones, priapism, leg ulcersandproliferativeretinopathy.Patientsalsoexperience chronichemolyticanemia,inflammation,celladhesion,tissue hypoxia,organischemiaandtissueinfarction.4
Hemolyticanemia,amajorcomplicationofSCAislinked toreducednitricoxide(NO)bioavailability.Innormal condi-tions,NObindstosolubleguanylatecyclase,whichconverts guanosinetriphosphatetocyclicguanosinemonophosphate. Itcausesrelaxationofvascularsmoothmuscleandeventual peripheralvasodilatation.Plasmahemoglobinreleasedfrom intravascularhemolysisofsickledredcellsconsumesNOand impairsits homeostaticvascular functions.Apartfrom the scavengingeffectsofcell-freeplasmaHbonNO,reactive oxy-genspecies(ROS)alsoscavengeNOanddepleteitspool.The generationofROSinpatientswithsicklecelldisease (SCD) resultsfromtissueischemiathatoccursduringvaso-occlusion and the accompanyingischemia-reperfusion injury.5 It has
alsobeen suggestedthat the plasma level ofl-arginine, a
precursorofNO,isdepletedduringseverehemolysis, vaso-occlusivecrisesandacutechestsyndrome.Thisdepletionis partlyduetoincreasedlevelsofplasmaarginaseinthese con-ditions,especiallyduringseverehemolysis.6
Increased expression of adhesion molecules, including interleukin(IL)-6alsostimulatesthe adherenceofredcells andneutrophilstotheendothelium.4,7IL-6,amultifunctional
cytokine,playsastrategicroleinhostdefenseand exhibits bothpro-inflammatoryandanti-inflammatoryproperties.Itis encodedbytheIL-6genewhichislocatedonchromosome7at 7p21-p14,betweenD75135andD75370.8Apartfrom
stimula-tionofBcellproliferationintoplasmacells,itsotherbiological activitiesincludeinductionofthesecretionofacutephase proteinsbylivercells,T-cellactivationanddifferentiationinto cytotoxiccells,andactivationofhematopoiesis.9
Severalstudieshaveshownthatthelevelsofcytokinesin patientswithSCA,eveninsteadystate,areelevated.10–13In
individualswithSCA,pro-inflammatorycytokinessuchas IL-1,IL-6,IL-8andtumornecrosisfactoralpha(TNF-␣)cause chronicendotheliumactivationandadhesionofsickledred cells,and arethus responsibleforthe constantlocaltissue ischemiaand necrosisseen.Inaddition, thereisincreased leukocyteaggregationinresponsetoinflammatorycytokines inSCA.10
Theprimarymechanismofdefenseagainstthedeleterious effectsoffreeHbisprovidedbyhaptoglobin(Hp),anacute phase ␣2-globulin glycoprotein and important physiologic antioxidant,whichbindstoplasmaHbformingasoluble com-plex(Hb-Hpcomplex)toeliminateHbfromtheplasma.This clearanceisimportantbecausethecomplexisnotinertand cancatalyzeoxygenreactivespeciesandconsumeNO.14–16
TheHplocusinthechromosome,16q22,ispolymorphic. Twoclassesofalleleshavebeenidentified:1and2,andthe Hp-2allelepresentsaduplicatedDNAsegmentof1700base pairs (bp) dueto anintragenic duplication ofexons 3and
4.17,18 InSouthAmericaandAfrica,theHp-1allele
predom-inates,unlikeinSoutheastAsiawherethefrequencyofthe Hp-1alleleislowerthantheHp-2allele.19Therearethree
pos-siblegenotypesfortheHpinhumans:Hp1-1,Hp2-1andHp 2-2.
These phenotypesdiffer inthestructureofthe protein, electrophoreticmobility,antioxidantandanti-inflammatory properties,hencetheyexhibitdifferentclinicaleffects.18,20,21
Hp1-1isthemostbiologicallyactiveinbindingfreeHband suppressingconsequentinflammatoryresponses.Hp2-2isthe leastbiologicallyactivewithareducedoverallactivityandHb clearanceeffects,whileHp2-1isintermediate.14Hp
signifi-cantlyreducesthesynthesisofROSinindividualswiththeHp 1-1genotypebecauseofitspotentantioxidantactivity,butin peoplewiththeHp2-2polymorphism,theantioxidantactivity isweakwhichultimatelyfavorsthepersistenceof inflamma-toryresponse.22,23Guettaetal.andUskokovicetal.reported
thatthe Hp1allele whenboundtofreeHb, stimulatesthe secretionofIL-6andIL-10moresignificantlythantheHp2 allele.14,24
In patients with SCA, a disease characterized by both chronic and acute inflammatory and hemolytic states, the modulatoryroleoftheHpgenotypeontheexpressionofthese cytokinesisstilllargelyunderstudied.Thepresentstudywas thereforedesignedtoinvestigatetheassociationbetweenthe differentHppolymorphismsandthesecretionofIL-6andIL-8 inBrazilianSCApatientsincomparisontohealthyindividuals fromthesamelocality.
Methods
Casesandcontrols
Thiscasecontrolstudyincluded60patientswithSCA,aged 13yearsandabove,whowererecruitedfromtheHereditary AnemiaOutpatientClinicoftheHematologyandBlood Trans-fusion Unit, Universidade Federal de São Paulo (UNIFESP), Brazil.Atthe time ofrecruitment,all the patientswere in steadystate,thatis,theyhadhadnoacuteeventforatleast twelveconsecutiveweeks.Thecontrolgroupconsistedof74 apparently healthy,age andgender-matchedHb AA volun-teersfromthesamelocality.
Pregnantwomen,individualswithacuteorchronic infec-tions, chronic renal impairment, rheumatologic disorders, patientson hydroxyureatherapy,chronicblood transfusion therapyandthose whohadhadabloodtransfusionwithin theprecedingthreemonthswereexcludedfromthestudy.All participantsortheirparents/guardians(inthecasesof ado-lescents)gavewritteninformedconsentbeforeparticipation inthestudy.Moreover,permissionforthestudywasobtained fromtheResearchEthicsCommitteeoftheinstitution.
Sociodemographiccharacteristicsofthestudyparticipants wereobtainedusingastructuredquestionnairewhiledataon SCAcomplicationswereretrievedfrommedicalcharts.
Determinationofplasmalevelofcytokines
enzymelinkedimmunosorbentassays (ELISA)according to theinstructionsprovidedbythemanufacturer.TheIL-6ELISA (BDOptEIA, BDBiosciences,SanDiego, USA)hada normal range2.2–12.1pg/mLandlimitofdetectionof2.2pg/mL.For theIL-8ELISA(BDOptEIA,BDBiosciences,SanDiego,USA),the normalrangewas10.2–34.3pg/mLandthelimitofdetection was0.8pg/mL.
DNAextraction
Buffy-coat samples, which were stored at −80◦C at the
MolecularBiologyLaboratoryofUNIFESP,weredefrostedand subjected to red blood cell lysis with saponin. Leukocytes werewashedwithSolution A(100mMKCl,10mMTrisand 2.5mM MgCl2).DNAextractionwas carriedout using
Solu-tionAwithoutsaponin andSolutionB(10mMTris,2.5mM MgCl2,1%Tween-20,1%Triton×100andproteinaseK).After one-hourincubation at 60◦C, DNA was purified with
Phe-nol:chloroform:isoamylalcohol(25:24:1).25
Haptoglobingenotyping
Hpgenotypingwasperformedbyapolymerasechain reac-tion (PCR) techniqueas described byKoch et al.in 2002.17
The method consists of two protocols. In protocol 1, the 1757bpallele1specificsequenceandthe3481bpallele2 spe-cificsequencewereamplified.Inhomozygousindividuals,the intensityofthe1757bpallele-1specificbandishigherthanthe 3481bpallele-2specificband.For22patientswithSCA,itwas notpossibletodefineconclusivelywhetherthe3481bpband waspresent.Thesesamplesweresubmittedtoprotocol2in ordertoamplifythe349bpallele-2specificsequence. Proto-col2involvedtheamplificationofthe349bpallele2specific sequencetoconfirmwhentheresultofthefirstassaywasnot
conclusive.ThePCRproductswereseparatedbyagarosegel electrophoresis.
Statisticalanalysis
DatawasanalyzedusingtheStatisticalPackagefortheSocial Sciences (SPSS) computerprogram version 17.0.Themean plasma valuesofthe interleukins were comparedbetween casesandcontrolbytheindependentsamplet-test,whileIL valuesbetweentheHP1-1,Hp2-1andHp2-2genotypeswere comparedwithanalysisofvariance(ANOVA).Thefrequencies ofHppolymorphismsinthepatientsandthecontrolswere comparedwiththechi-squaretest.Statisticalsignificancewas setforp-values<0.05.
Results
AsshowninTable1,theageandgenderprofilesweresimilar betweenSCApatientsandthecontrolgroup.
Interleukin-6and-8plasmalevels
TheplasmalevelsofIL-6andIL-8weresignificantlyhigherin patientscomparedtothecontrols(p-value<0.0001)asshown inTable1.Therewasaboutafour-foldincreaseinthelevels oftheplasmaIL-6andIL-8inpatientswithSCAcomparedto thehealthycontrols.
Haptoglobinallelesandgenotypes
Thefrequencies ofHp-1 alleles amongthe casesand con-trolswere54(45.0%)and81(54.7%)respectively(Table1).Hp
Table1–Sociodemographic,haptoglobingenotypesandplasmalevelsofinterleukin-6and-8betweenthesicklecell
anemiapatientsandcontrols.
Variables SCAgroup
n=60
Controlgroup n=74
p-value
Gender–n(%)
Male 32(53) 39(53) 1.00a
Female 28(47) 35(47)
Age–years
Median 26.00 29.00 0.29b
Range 15–50 17–60
PlasmaIL(pg/mL)–mean±SD
IL-6 15.9±9.1 4.4±7.4 <0.0001c
IL-8 20.5±15.2 4.9±7.4 <0.0001c
Haptoglobinalleles–n(%)
Hp-1 54(45.0) 81(54.7) 0.113a
Hp-2 66(55.0) 67(43.5)
Haptoglobingenotypes–n(%)
Hp1-1 10(16.7) 25(33.8)
Hp2-1 34(56.7) 31(41.9) 0.07a
Hp2-2 16(26.6) 18(24.3)
SCA:sicklecellanemia;SD:standarddeviation,IL:interleukin. a Chi-square.
b Mann–Whitneytest.
Table2–Hematologicalprofileofthe60sicklecellpatients.
Hematologicalparameters Overall Mean(SD)
Hp1-1 Mean(SD)
Hp1-2 Mean(SD)
Hp2-2 Mean(SD)
Ftest p-valuea
Hemoglobin(g/dL) 8.1(1.0) 7.7(0.9) 8.3(1.0) 8.0(1.2) 1.143 0.326
Hematocrit(%) 23.4(3.1) 21.9(2.2) 23.9(3.2) 23.2(3.0) 1.643 0.202
MCV(fL) 91.6(8.2) 89.8(8.2) 92.9(6.9) 89.8(10.3) 1.081 0.346
Leukocytecount(×1009/L) 11.2(2.8) 11.1(2.1) 11.4(3.0) 10.9(2.6) 0.146 0.865
Plateletcount(×1009/L) 428.4(143.0) 482.5(158.5) 403.8(143.8) 446.9(127.2) 1.368 0.263 Reticulocytecount(×1009/L) 190.4(134.0) 196.9(114.4) 204.5(113.7) 156.9(180.9) 0.643 0.530
HemoglobinF(%) 7.5(6.2) 8.6(6.1) 8.0(6.7) 5.5(4.9) 0.970 0.386
MCV:meancorpuscularvolume.
a ANOVAwasusedtocomparethemeansofthehematologicalparametersbetweenthethreeHpgenotypes.
2-1wasthe mostcommon Hpgenotypein casesand con-trols,accountingfor34(56.7%)and31(41.9%)respectively.The leastcommongenotypeinSCApatientswasHp1-1,16.7%. There was no statisticallysignificant difference in the fre-quencydistributionofHpgenotypesbetweencasesandthe controls[2=5.280,degreeoffreedom(df)=2,p-value=0.07].
Themeanvaluesofallthehematologicalparameterswerenot significantlydifferentbetweenthethreeHpgenotypegroups (Table2).
Associationbetweenhaptoglobingenotypesand interleukin-6
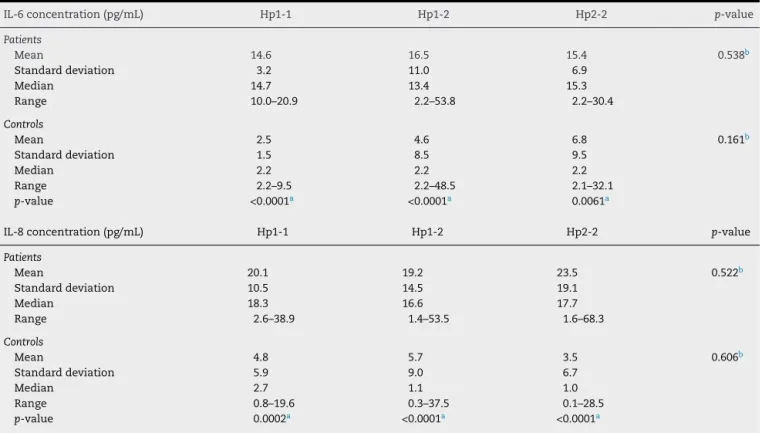
Table3comparesthemeanplasmaconcentrationsofIL-6of thethreeHpgenotypes.Forthecases,therewasnosignificant
differenceinthemeanplasmaconcentrationsofIL-6forthe
Hp1-1,Hp2-1andHp2-2genotypes(14.6;16.5and15.4pg/mL, respectively;F=84.47;p-value=0.54).Forthecontrols,the dif-ferenceinthemeanplasmaconcentrationsofIL-6fortheHp genotypegroupswasalsosimilar(F=53.23;p-value=0.161).
Two-thirdsofpatientswithSCA,comprisingof8withHp 1-1;20withHp2-1and12withHp2-2hadhighlevelsof IL-6i.e.IL-6>12.1pg/mL,whileonlytwo(3.3%)hadlowlevels (values<2.2pg/mL)(Table4).However,amongthecontrols,the majority,62(83.8%)hadlowlevelsofIL-6.
Haptoglobingenotypesandinterleukin-8
Furthermore,themeanplasmavaluesofIL-8ofthethreeHp genotypes weresimilarbothforthecasesandthecontrols
Table3–Associationbetweenhaptoglobingenotypesandplasmaconcentrationsofinterleukin-6and-8levels.
IL-6concentration(pg/mL) Hp1-1 Hp1-2 Hp2-2 p-value
Patients
Mean 14.6 16.5 15.4 0.538b
Standarddeviation 3.2 11.0 6.9
Median 14.7 13.4 15.3
Range 10.0–20.9 2.2–53.8 2.2–30.4
Controls
Mean 2.5 4.6 6.8 0.161b
Standarddeviation 1.5 8.5 9.5
Median 2.2 2.2 2.2
Range 2.2–9.5 2.2–48.5 2.1–32.1
p-value <0.0001a <0.0001a 0.0061a
IL-8concentration(pg/mL) Hp1-1 Hp1-2 Hp2-2 p-value
Patients
Mean 20.1 19.2 23.5 0.522b
Standarddeviation 10.5 14.5 19.1
Median 18.3 16.6 17.7
Range 2.6–38.9 1.4–53.5 1.6–68.3
Controls
Mean 4.8 5.7 3.5 0.606b
Standarddeviation 5.9 9.0 6.7
Median 2.7 1.1 1.0
Range 0.8–19.6 0.3–37.5 0.1–28.5
p-value 0.0002a <0.0001a <0.0001a
IL:Interleukin.
a Independentsamplet-testwasusedtocomparethemeaninterleukinconcentrationsbetweenthepatientsandthecontrols.
Table4–Relationshipbetweenhaptoglobingenotypesandinterleukin-6and-8levels.
Haptoglobingenotype Hp1-1 Hp2-1 Hp2-2 Total
n(%) n(%) n(%) n(%)
IL-6inSCAgroup(n=60)
Highlevel(>12.1pg/mL) 8(80.0) 20(58.8) 12(75.0) 40(66.7)
Normallevel(2.2–12.1pg/mL) 2(20.0) 13(38.2) 3(18.8) 18(30.0)
Lowlevel(<2.2pg/mL) 0(0) 1(2.9) 1(6.2) 2(3.3)
IL-6inControlgroup(n=74)
Highlevel(>12.1pg/mL) 0(0) 1(3.2) 4(22.2) 5(6.7)
Normallevel(2.2–12.1pg/mL) 2(8.7) 4(12.9) 1(5.6) 7(9.5)
Lowlevel(<2.2pg/mL) 23(91.3) 26(83.9) 13(72.2) 62(83.8)
IL-8inSCAgroup(n=60)
Highlevel(>34.3pg/mL) 1(10.0) 6(17.6) 4(25.0) 11(18.3)
Normallevel(10.2–34.3pg/mL) 7(70.0) 17(50.0) 10(62.5) 34(56.7)
Lowlevel(0.8–10.1pg/mL) 2(20.0) 11(32.4) 2(12.5) 15(25.0)
Extremelylowlevel(<0.8pg/mL) 0(0) 0(0) 0(0) 0(0)
IL-8inControlgroup(n=74)
Highlevel(>34.3pg/mL) 0(0) 0(0) 0(0) 0(0)
Normallevel(10.2–34.3pg/mL) 4(16.0) 5(16.1) 1(5.6) 10(13.5)
Lowlevel(0.8–10.1g/mL) 12(48.0) 14(45.2) 8(44.4) 34(46.0)
Extremelylowlevel(<0.8pg/mL) 9(36.0) 12(38.7) 9(50.0) 30(40.5)
SCA:sicklecellanemia.
(F=97.34; p-value=0.52 and F=56.82; p-value=0.61, respec-tively)(Table3).
AsshowninTable4,themajorityofthecases(56.7%)as wellasthecontrols(46.0%)hadnormallevelsofplasmaIL-8.
Discussion
SCAisamonogenicdiseasewithanexceptionalphenotypic variabilitythatisregulatedbyseveralknownandunknown geneticfactors.Understandingthevascularandinflammatory componentsofthediseasecanhelpinprovidinginformation onthepossiblegenomicsitesthatinfluencethephenotype. StudiesontheHppolymorphisms,animportantmarkerof vasculardiseaseandpro-inflammatorycytokinesmay there-foreprovideusefulinformation.Tothebestknowledgeofthe authors,thisisthefirststudythatexaminedtherelationship betweenHppolymorphismsandinterleukinsamongBrazilian SCApatients.TheabilitytopredictthephenotypeofSCA dur-ingthefirstmonthsoflifeorevenintheprenatalperiodwill allowamorepreciseprognosisandindividualizedtreatment. Intravascular hemolysis produces a state of endothe-lial dysfunction, vascular proliferation, inflammation and oxidativestress.Recentstudieshavedemonstratedthe impor-tant roles offreeplasma Hb inreducing NO. Intravascular hemolysisandthereductionofNOcausesincreased expres-sionofendothelin-1,andactivationofendothelialadhesion moleculesandplatelets.Thus,notonlydotheycause vaso-constriction,butNOisinvolvedinendothelialactivationand proliferationthateventuallycontributestothepathogenesis ofSCA.4,26Itisknownthatsickledredcellsbindtothevascular
endotheliumcellsbyintegrinalpha-4beta-1.Thismembrane proteinthenactsasareceptorforeitherfibronectinor VCAM-1.Intheendothelium,VCAM-1isstimulatedbyinflammatory cytokines,suchasIL-6andIL-8whicharereleasedbythe acti-vatedleucocytes.27,28 Hemeand hemin,which arereleased
intothecirculationduringtheactivephaseofsickle-cell dis-ease, also contributeto inflammatorystates in individuals withSCAbyincreasingtheexpressionofendothelial adhe-sionmoleculesandadherenceofleukocytesandreticulocytes toendothelialcells.29
Inthepresentstudy,higherlevelsofbothIL-6andIL-8were detectedinSCAindividuals comparedtothecontrolgroup (p-value<0.001). Ourdata agreewithprevious studies that identified elevatedlevelsofinflammatorycytokinesinSCA patients.10,30,31
Considering that the transcription ofcytokines is regu-lated byagreatnumberofgeneticmechanisms,thisstudy intendedtoverifywhethertheHppolymorphismsinfluence cytokinesecretion.Hphasemergedasoneofthemost impor-tantSCDphenotypicmodulators,asitisaproteinwithhigh capabilitytobindtofreeHbintheplasma,formingtheHp–Hb complex and thereby preventing heme-catalyzed oxidative damage.32AlthoughthethreeHpphenotypeshavethesame
abilitytobindtofreeHb,thespeedofhemerelease canbe relatedtodifferencesintheirmolecularsize.Hp2-2,which isamorecomplexpolypeptide,removesironmoreslowlyto theextravascularspacetherebyallowingfreeHbtobeinthe circulationforalongerperiod,causingmoreoxidativestress. Ontheotherhand,Hp1-1protectstheendotheliumagainst oxidative damage,as itis themostbiologicallyactive.33 In
this analysis, the Hp 2-1phenotype was morecommon in both patients and controls(56.7% and 41.9%, respectively). Moreover,the profileofthe Hpgenotypewas notdifferent betweenthegroups(p-value=0.70).Thispatternagreeswith moststudiesonthedistributionofhaplotypepolymorphisms
inSCD.32,34
intracellular parasites and inhibiting the Th2 cytokines neededforhumoralresponse.35Moreover,theHp-1-1-Hb
com-plexsignificantlystimulatesthesecretionofmoreIL-6than theHp-2-2-Hbcomplex.14
TherehavebeeninconsistenciesinthedistributionofHp genotypes in the SCA population. In 2011, Santos et al.32
reportedthattheHp2-2phenotypeinBrazilianSCApatients waslessfrequentthantheHp1-1phenotypeand hypothe-sizedthatHp2-2mightbeassociatedwithworseprognosis becauseoflowerantioxidantcapacityandhigher inflamma-toryresponse. In the current study, the Hp 1-1 phenotype waslesscommon(16.7%),whichagreeswiththefindingsof Adekile&HaiderinKuwaitipatientswithSCDinwhichonly 4.9%hadHp1-1comparedto52.4%inthosewiththeHp2-2
genotype.34Onthecontrary,inthesamestudytheyreported
Hp2-2asbeinglessfrequentamongNigerianpatientswith SCD.Itwasconcludedthat,inSCDindividuals,theHp geno-typesappeartodifferbetweenethnicgroupsandgeographical areas,andarenotnecessarilylinkedto-globingene haplo-typesindifferentpopulations.
MoststudiesontheinfluenceofHppolymorphismsonthe clinicalphenotypesofSCDhavefailedtoestablishanystrong linkbetweenthetwo.Forinstance,nosignificantassociation wasfoundbetweentheHp-2alleleandincreasedriskofsevere vaso-occlusivecrisesamongKuwaitiHbSS patients.34 This
may implythat other factors mediatethe influenceof Hp. Ofsuch,thescavengerreceptorCD163andhemeoxygenase playactiverolesintheclearanceoftheHb–Hpcomplexfrom theplasma,therebypreventingoxidativedamagecausedby heme.15ThelevelandactivityofCD163,ratherthanHp
poly-morphisms maytherefore berelated toSCD complications andseverity.
AmongtheSCApatientsinthepresentstudy,the geno-typesdidnotappeartoberelatedtotheserumlevelsofIL-6 and IL-8; there was norelationship between the Hp geno-typesandcytokinelevels.Thisisincontrasttothefindings ofGuettaetal.whoreportedthattheHp-1allelewas asso-ciatedwiththesecretionofsignificantlymoreIL-6andIL-10 thantheHp-2allele.14Theyalsodemonstratedthattherelease
ofthesecytokineswasdependentonthebindingofthe Hb-HpcomplextotheCD163receptorandtheactivityofcasein kinase II. However, the lackof association ofHp polymor-phisms withthe expressionofpro-inflammatorycytokines maybeduetothesmallnumberofpatientsinthepresent study.
ConsideringtheimportantrolesofcytokinesinSCA patho-physiology, further investigations are necessary to identify factorsthatareresponsibleforincreasedsecretionofplasma IL-6andIL-8.Althoughtheresultsofthisstudydonotallow us to conclude that Hp genotypes on their own influence expressionofIL-6and8inSCApatients,thispolymorphism when investigatedwithother genetic factors,may unravel thepathogenesisofelevatedpro-inflammatorycytokinesin SCA.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
ThisstudywasfundedbyFundac¸ãodeAmparoàPesquisado EstadodeSãoPaulo–FAPESP(grantnumber04/04498-4)and Coordenac¸ãodeAperfeic¸oamentodePessoaldeNívelSuperior –CAPES(grantnumber054/2010).
Scholarships were provided by CAPES, CNPq (Conselho Nacional deDesenvolvimento CientíficoeTecnológico) and COLSAN(Associac¸ãoBeneficentedeColetadeSangue).
r
e
f
e
r
e
n
c
e
s
1.Canc¸adoRD,JesusJA.Adoenc¸afalciformenoBrasil.RevBras HematolHemoter.2007;29:204–6.
2.Sicklecellanemia.OnlineMendelianInheritanceinMan (OMIM).Availablefrom:http://omim.org/entry/603903[cited 02.06.15].
3.SteinbergMH,SebastianiP.Geneticmodifiersofsicklecell disease.AmJHematol.2012;87(8):795–803.
4.KatoGJ,GladwinMT,SteinbergMH.Deconstructingsicklecell disease:reappraisaloftheroleofhemolysisinthe
developmentofclinicalsubphenotypes.BloodRev. 2007;21(1):37–47.
5.MackAK,KatoGJ.Sicklecelldiseaseandnitricoxide:a paradigmshift?IntJBiochemCellBiol.2006;38(8):1237–43.
6.MorrisCR,VichinskyEP,vanWarmerdamJ,MachadoL, Kepka-LenhartD,MorrisSMJr,etal.Hydroxyureaand argininetherapy:impactonnitricoxideproductioninsickle celldisease.JPediatrHematolOncol.2003;25(8):629–34.
7.BrittainJE,PariseLV.Cytokinesandplasmafactorsinsickle celldisease.CurrOpinHematol.2007;14(5):438–43.
8.Interleukin6;IL6.OnlineMendelianInheritanceinMan (OMIM).Availablefrom:http://omim.org/entry/147620[cited 02.06.15].
9.PopkoK,GorskaE,DemkowU.Influenceofinterleukin-6and G174CpolymorphisminIL-6geneonobesityandenergy balance.EurJMedRes.2010;15Suppl.2:123–7.
10.HibbertJM,HsuLL,BhathenaSJ,IruneI,SarfoB,CrearyMS, etal.Proinflammatorycytokinesandthehypermetabolismof childrenwithsicklecelldisease.ExpBiolMed(Maywood). 2005;230(1):68–74.
11.AkohoueSA,ShankarS,MilneGL,MorrowJ,ChenKY,Ajayi WU,etal.Energyexpenditure,inflammation,andoxidative stressinsteady-stateadolescentswithsicklecellanemia. PediatrRes.2007;61(2):233–8.
12.PatelN,GonsalvesCS,MalikP,KalraVK.Placentagrowth factoraugmentsendothelin-1andendothelin-Breceptor expressionviahypoxia-induciblefactor-1alpha.Blood. 2008;112(3):856–65.
13.LanaroC,Franco-PenteadoCF,AlbuquequeDM,SaadST, ConranN,CostaFF.Alteredlevelsofcytokinesand inflammatorymediatorsinplasmaandleukocytesofsickle cellanemiapatientsandeffectsofhydroxyureatherapy.J LeukocBiol.2009;85(2):235–42.
14.GuettaJ,StraussM,LevyNS,FahoumL,LevyAP.Haptoglobin genotypemodulatesthebalanceofTh1/Th2cytokines producedbymacrophagesexposedtofreehemoglobin. Atherosclerosis.2007;191(1):48–53.
15.ThomsenJH,EtzerodtA,SvendsenP,MoestrupSK.The haptoglobin-CD163-hemeoxygenase-1pathwayfor hemoglobinscavenging.OxidMedCellLongev. 2013;2013:523652.
16.CoxSE,MakaniJ,SokaD,L’EsperenceVS,KijaE,
andriskofabnormaltranscranialDoppleramongpatients withsicklecellanemiainTanzania.BrJHaematol. 2014;165(5):699–706.
17.KochW,LatzW,EichingerM,RoguinA,LevyAP,SchomigA, etal.GenotypingofthecommonhaptoglobinHp1/2 polymorphismbasedonPCR.ClinChem.2002;48(9): 1377–82.
18.AslehR,LevyAP.Invivoandinvitrostudiesestablishing haptoglobinasamajorsusceptibilitygenefordiabetic vasculardisease.VascHealthRiskManag.2005;1(1):19–28.
19.LangloisMR,DelangheJR.Biologicalandclinicalsignificance ofhaptoglobinpolymorphisminhumans.ClinChem. 1996;42(10):1589–600.
20.BarbosaLC,Miranda-VilelaAL,HiragiCdeO,RibeiroIF, DaldeganMB,GrisoliaCK,etal.Haptoglobinand
myeloperoxidase(−G463A)genepolymorphismsinBrazilian sicklecellpatientswithandwithoutsecondaryironoverload. BloodCellsMolDis.2014;52(2–3):95–107.
21.CarterK,WorwoodM.Haptoglobin:areviewofthemajor allelefrequenciesworldwideandtheirassociationwith diseases.IntJLabHematol.2007;29(2):92–110.
22.LazaldeB,Huerta-GuerreroHM,Simental-MendiaLE, Rodriguez-MoranM,Guerrero-RomeroF.Haptoglobin2-2 genotypeisassociatedwithTNF-alphaandIL-6levelsin subjectswithobesity.DisMarkers.2014;2014:912756.
23.QuayeK.Haptoglobin,inflammationanddisease.TransRSoc TropMedHyg.2008;102(8):735–42.
24.UskokovicA,ArambasicJ,BogojevicD,Ivanovic-MaticS, MihailovicM,DinicS,etal.Differencesbetweenmolecular mechanismsinvolvedintheregulationofhaptoglobingene expressionduringtheacutephaseresponseanddietary restriction.FoliaBiol(Praha).2009;55(3):107–15.
25.LeeTH,SakaharaNS,FiebigEW,HirschkornDF,JohnsonDK, BuschMP.Quantitationofwhitecellsubpopulationsby polymerasechainreactionusingfrozenwhole-blood
samples.ViralActivationTransfusionStudy.Transfusion. 1998;38(3):262–70.
26.AtagaKI,MooreCG,JonesS,OlajideO,StrayhornD,
HinderliterA,etal.Pulmonaryhypertensioninpatientswith sicklecelldisease:alongitudinalstudy.BrJHaematol. 2006;134(1):109–15.
27.SteinbergMH,RodgersGP.Pathophysiologyofsicklecell disease:roleofcellularandgeneticmodifiers.Semin Hematol.2001;38(4):299–306.
28.PathareA,KindiSA,DaarS,DennisonD.Cytokinesinsickle celldisease.Hematology.2003;8(5):329–37.
29.GhoshS,AdisaOA,ChappaP,TanF,JacksonKA,ArcherDR, etal.Extracellularhemincrisistriggersacutechestsyndrome insicklemice.JClinInvest.2013;123(11):4809–20.
30.PathareA,AlKindiS,AlnaqdyAA,DaarS,Knox-MacaulayH, DennisonD.CytokineprofileofsicklecelldiseaseinOman. AmJHematol.2004;77(4):323–8.
31.Etienne-JulanM,BelloyMS,DecastelM,DougaparsadS, RavionS,Hardy-DessourcesMD.Childhoodsicklecellcrises: clinicalseverity,inflammatorymarkersandtheroleof interleukin-8.Haematologica.2004;89(7):863–4.
32.SantosMN,BezerraMA,DominguesBL,ZaccariottoTR, OliveiraDM,CostaFF,etal.Haptoglobingenotypesin sickle-celldisease.GenetTestMolBiomarkers. 2011;15(10):709–13.
33.Melamed-FrankM,LacheO,EnavBI,SzafranekT,LevyNS, RicklisRM,etal.Structure-functionanalysisofthe antioxidantpropertiesofhaptoglobin.Blood. 2001;98(13):3693–8.
34.AdekileAD,HaiderMZ.Haptoglobingenepolymorphismsin sicklecelldiseasepatientswithdifferentbetaS-globingene haplotypes.MedPrincPract.2010;19(6):447–50.