Ef
fi
cacy of removal of cariogenic bacteria and
carious dentin by ablation using different
modes of Er:YAG lasers
A. Baraba
1, L. Kqiku
2, D. Gabri
ć
3,
Ž
. Verzak
4, K. Hanscho
2and I. Mileti
ć
1 1Department of Endodontics and Restorative Dentistry, School of Dental Medicine, University of Zagreb, Zagreb, Croatia
2
University Clinic of Dental Medicine and Oral Health, Division of Prosthodontics, Restorative Dentistry, Periodontology and Implantology, Medical University Graz, Graz, Austria
3
Department of Oral Surgery, School of Dental Medicine, University of Zagreb, University Hospital Center Zagreb, Zagreb, Croatia
4
Department of Pediatric and Preventive Dentistry, School of Dental Medicine, University of Zagreb, University Hospital Center Zagreb, Zagreb, Croatia
Abstract
The primary objective of thisin vitrostudy was to evaluate the efficiency of removal of cariogenic bacteria and carious dentin by ablation using two lasers:fluorescence-feedback controlled (FFC) Er:YAG laser and different pulses of Er:YAG laser based on variable square pulse technology (VSPt). The secondary objective was to measure the temperature during laser ablation of carious tissue. Seventy-two extracted human molars were used in this study. Sixty teeth with carious dentin were randomly divided into four experimental groups according to the treatment for caries removal: group 1: 400ms (FFC group); group 2: super
short pulse (SSP group, 50ms pulse); group 3: medium short pulse (MSP group, 100ms pulse); group 4: short pulse (SP group,
300ms pulse) and one positive control group with no treatment. Twelve teeth without carious lesion were used as a negative control group. After caries removal, swabs were taken with cotton pellets and real-time PCR analysis was performed. During caries ablation, a thermal infrared camera was used to measure the temperature changes. In all experimental groups, speci-mens were free of bacterial contamination after the treatment. In the SSP, MSP and SP groups, temperatures measured during caries ablation were significantly higher compared to temperatures in the FFC group (Po0.001). In thisin vitrostudy, laser
treatment for removal of carious dentin and cariogenic bacteria was an efficient treatment modality without causing excessive temperatures that might adversely affect pulp vitality.
Key words: Dental caries; Er:YAG laser; Ablation; Real-time PCR; Thermography
Introduction
The aim of caries excavation is to remove dentin contaminated by bacteria without removal of sound tooth structure, and maintain the vitality of the pulp (1). Caries lesions have two distinct substrates with different chemical composition and morphological structures: caries-infected and caries-affected dentin (2,3). The inner‘infected dentin’ is a superficial and soft necrotic zone rich in bacteria, incapa-ble of remineralization, with degenerated collagen fibrils that have lost their cross-links (4–6). If viable bacteria
present in the infected dentin remain after caries removal, they may potentially release antigens into the pulp and cause a chronic inflammation reaction (7). Interestingly, well-sealed margins of the cavity seem to be more crucial for the long-term success of the restoration and pulp vitality than the presence of bacteria in the cavity since clinical follow-ups of bonded restorations placed over soft
carious dentin showed that further progression of carious lesion can be arrested (8). However, caries-infected dentin showed extremely low cohesive strength as a result of low mineral content and changes in organic matrix (9), and consequently lower microtensile bond strength compared to sound and caries-affected dentin (10,11). Although thicker hybrid layers are obtained in caries-infected dentin, many dentin tubules remain completely free from tag formation (12–14). Due to this poor
inter-action during adhesive procedures, it is generally accepted that this layer needs to be removed prior to the place-ment of the restoration. Nevertheless, caries-affected dentin also produces lower bond strengths compared to normal dentin (15–18) due to lower mechanical
ties and changes in chemical and morphological proper-ties, and therefore this layer, which is free of bacteria or
Correspondence: D. Gabrić:<[email protected]> Received July 10, 2017 | Accepted November 7, 2017
contains clinically insignificant number of bacteria, may be retained (4).
Different methods are described for caries removal, including rotary burs, hand instrument action, air abrasion, ultrasonic techniques, enzymes treatment, chemomechani-cal techniques and laser treatment (19). A laser commonly used for ablation of hard dental tissue is the Er:YAG laser. The erbium wavelengths coincide with the absorp-tion peak of water and hydroxyapatite causing removal of hard dental tissue by microexplosions (20). Carious tissue contains even more water compared to healthy hard dental tissues and therefore the high absorption of the Er:YAG laser provides a selective and conservative caries removal without extending the preparation into the sound tooth structure. Introduction of the Er:YAG laser with variable square pulse technology (VSPt) enabled the use of very short, square-shaped pulses of adjustable duration. The pulse profile is controlled and ensures that the power within the pulse is approximately constant with all pulse energy being used up for ablation (21). However, according to the histological evaluation in a study by Medioni et al. (22), Er:YAG laser removed both infected and affected dentin. Another possibility to improve selec-tive caries removal is the application of fluorescence feedback-controlled (FFC) Er:YAG laser, a combination of a diagnostic device and Er:YAG laser. With this system, the removal of dental hard tissues is controlled by the fluorescence signal from the tooth surface, induced by the red-infrared indium gallium arsenide diode laser (23). The excitation wavelength induces afluorescence signal that has been assigned to protoporphyrin, a bacterial breakdown product (24). A sensor for the detection of fluorescence radiation of the dentinal tissue indicates whether any infected carious dentin is still present in the cavity, depending on the threshold level set when operating with FFC Er:YAG laser. The advantages of laser also include bactericidal properties from the high temperature (photothermal effect) during laser irradia-tion. The photothermal effect may be responsible for kill-ing residual bacteria in cavities durkill-ing caries ablation. However, the heat produced during laser ablation can cause thermal damage to irradiated substrates or the pulp in case of a temperature increase of more than 5.5°C, as shown in the in vivo study on monkeys by Zach and Cohen (25). Therefore, it is of outmost importance that these alternative techniques for caries removal are harm-less for tooth pulp, in terms of thermal damage.
According to the literature available to the authors, there is no study comparing removal of cariogenic bacteria and carious dentin by measuring the temperature changes during caries ablation with different pulses of VSPt-based Er:YAG compared to FFC Er:YAG laser. Therefore, the primary objective of this in vitro study was to evaluate efficiency of removal of cariogenic bacteria and carious dentin by ablation with FFC Er:YAG laser and with dif-ferent pulses of Er:YAG laser based on VSPt. The secondary
objective was to measure the temperature during laser ablation of carious tissue.
Material and Methods
Study design
Seventy-two extracted human molar teeth were included in the study: 60 teeth with cavitated caries lesions extend-ing into dentin, and 12 teeth without caries lesion. All molars were extracted for periodontal reasons at the Department of Oral Surgery, School of Dental Medicine, University of Zagreb. This experimental study was approved by the regional Ethical Review Board, University of Zagreb (106/09). Written informed consent was obtained from all participants to use their extracted teeth for scientific purposes. Inclusion criteria were teeth presenting cavi-tated caries lesions on the occlusal surface by visual exami-nation and caries depth between the enamel-dentin junction and middle two-thirds of dentin examined on radiograph. Exclusion criteria were the presence of restorations or cavitations on other tooth surfaces. The tooth specimens were thoroughly cleaned of all residual debris using brushes and curettes and stored in saline for 2 weeks; saline was changed daily. All 60 teeth with carious lesions were randomly divided into four experimental groups (n=12) and one positive control group (n=12), while teeth without caries lesions were used as a negative control group (n=12). In thefirst experimental group, FFC Er:YAG laser (Key III, KaVo, Germany) was used. For the remaining three experimental groups, a second generation Fidelis Plus II Er:YAG laser (Fotona, Slovenia) with super short pulse (SSP, 50 ms), medium short pulse (MSP, 100 ms), and short pulse (SP, 300ms), were used. For both lasers used all parameters were chosen according to the manu-facturer’s instructions. During caries ablation, temperature changes were measured with an infrared thermal camera while real-time PCR analysis was used to determine the presence of cariogenic bacteria.
Ablation procedures
All specimens werefixed with clamps during the caries removal treatment.
Groups 2(SSP group),3(MSP group)and 4(SP group). Cavities were prepared with a second generation Fidelis Plus II Er:YAG laser (Fotona) with super short pulse (SSP, 50ms), medium short pulse (MSP, 100ms), and short pulse (SP, 300 ms; Figure 1). The Er:YAG laser energy was delivered by a non-contact RO2-C handpiece with a spot size of 0.9 mm in diameter, under continuous water spray (3 mL/min) at a focus distance of 7 mm from the target. The pulse energy was 350 mJ for enamel and 250 mJ for dentin, with a pulse frequency of 10 Hz. The energy density for enamel was 54.7 and 39.1 J(cm2)-1pulse for dentin-1. The caries removal was performed under visual control by testing the hardness of the remaining tissue with a dental probe. The caries ablation procedure was considered complete after the dental probe induced a sharp sound and did not penetrate the dentin.
Infrared thermography
During caries ablation at room temperature, tempera-ture changes were measured with an infrared thermal camera. In the FFC group, a Thermosensorik GmbH camera was used (Thermosensorik GmbH, Geramny), and in SSP, MSP, and SP groups the ThermaCAM p45 (Flir Systems Inc., USA) was used for temperature measurement. Thermo-vision cameras were fixed and placed directly above the specimens at a distance of 20 cm.
Real time PCR analysis
After caries ablation, samples were taken with a sterile cotton pellet from each experimental group and both positive and negative control groups. Cotton pellets were
placed into Eppendorf tubes (Eppendorf, Germany), in 1 mL of phosphate buffer solution (PBS), and the contents of each tube were shaken to detach the samples of dentin from the cotton pellet. Real-time PCR analysis was used to investigate the presence of the positive and gram-negative cariogenic bacteria in cavities after caries ablation (Table 1).
For the bacterial DNA isolation, as the first step in bacterial identification, the QIAamp DNA Stool Mini Kit (Qiagen GmbH, Germany) was used according to the manufacturer’s instruction. Real-time PCR analysis was performed by using Primerdesignt Ltd. (Great Britain) genesis standards kits for Lactobacillus acidophilus, Streptococcus sanguinis, Porphyromonas gingivalis, S. mutans, Actinomyces israelli, Prevotella melanino-genica,Fusobacterium nucleatum,Peptostreptococcus micros,P. endodontalis, andP. gingivalis. The reaction mixture contained 20 mL: 10 mL of Precisiont Master-mixa (Primerdesignt Ltd.), 1mL of mixture of a primer Table 1. Gram-positive and gram-negative cariogenic bacteria investigated in this study.
Gram-positive bacteria Gram-negative bacteria
Streptococcus mutans Prevotella melaninogenica Streptococcus sanguis Fusobacterium nucleatum Lactobacillus acidophilus Porphyromonas endodontalis
Actinomyces israelli Porphyromonas gingivalis Peptostreptococcus micros
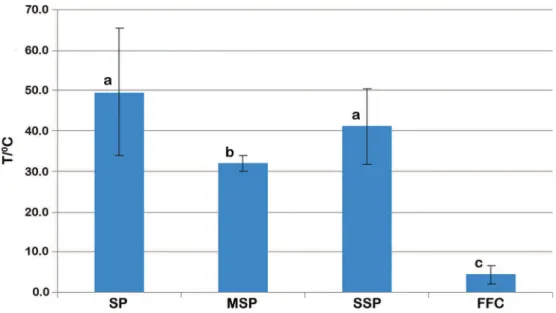
Figure 1.Average temperature (°C) and standard deviations for FFC, SP, MSP, and SSP groups. The temperatures were significantly higher in the SSP, MSP, and SP groups compared to temperatures in the FFC group (Po0.001). Temperature in the MSP group was
significantly lower compared to SP (Po0.001), and SSP (P=0.002) groups. FFC:fluorescence feedback controlled; SP: short pulse;
and a probe (Primerdesignt Ltd.), 4 mL of water and 5 mL of diluted DNA according to standard procedures. The PCR cycling conditions were performed as described in the amplification protocol of the PrimerDesign kit and cycling was performed in a LC480 (Roche Diagnostics, Austria). During PCR amplification, forward and reverse primers were hybridized to each bacterial DNA. Afl uoro-genic probe was included in the same reaction mix-ture, which consisted of a DNA probe labelled with a 50-dye and a 30-quencher. During PCR amplification, the probe was cleaved and the reporter dye and quencher were separated. The resulting increase influorescence was detected on a range of real-time PCR platform (LC480 (Roche Diagnostics). Positive control inside the specific kit was performed simultaneously during each PCR reaction, and RNAse/DNAse free water was used as negative control. The resulting data were averaged between the duplicates and then the proportions of each species were calculated against the universal assay primer/probe set (UniB) values of all species within each sample.
Statistical analysis
Data was statistically analyzed with one-way ANOVA and Scheffe’spost hoctest with the level of significance set to 5%. The analysis was performed using Statistica 7.0 (StatSoft, USA).
Results
Cariogenic bacteria were found in all specimens of the positive control group (Table 2) and not in specimens of the negative control group. In all laser experimental groups, specimens were free of the bacterial contamina-tion after ablacontamina-tion procedure.
Average temperatures for each group and the range of average temperatures for every specimen in experi-mental groups during caries ablation are shown in Figure 1. The temperatures were significantly higher in the SSP (41.2±9.3°C), MSP (32.0±1.9°C), and SP (49.5±15.7°C)
groups compared to the temperatures in the FFC group (4.5±2.4°C; Po0.001). The temperature during caries ablation in the MSP group was significantly lower com-pared to SP (Po0.001) and SSP (P=0.003) groups. There was no significant difference in temperatures between SP and SSP groups (P=0.129).
Discussion
The main purpose of this experimental study was to evaluate efficiency of removing cariogenic bacteria during ablation of carious tissue with two different lasers: FFC Er: YAG laser and VSPt based Er:YAG. In addition, the aim was also to measure the temperature changes during laser ablation of carious tissue. Qualitative and quantita-tive assessment of cariogenic bacteria of each sample was performed using RT PCR technique. Results showed that cavities in all experimental groups were free of bacterial contamination after laser-assisted caries abla-tion. Similar results were found only for FFC Er:YAG laser in studies that examined the amount of cariogenic bacteria after removal of carious tissue. These studies used dif-ferent methods of evaluation of residual bacteria such as cultivation of dentin samples on culture medium for S. mutans and L. species (26) or histological staining for gram-positive and gram-negative bacteria (27). The mechanism of removing bacteria from the tooth cavity using laser technology is mechanical and photothermal. High temperatures cause changes in the cell wall and membrane of bacteria, along with denaturation of proteins
Table 2.Quantity of examined cariogenic bacteria DNA in negative control samples.
SM SS LA AI PM FN PeM PE PG
31.12 30.12 28.12 21.00 27.20 24.10 28.60 18.00 38.10 32.15 30.05 31.20 29.10 31.00 31.50 34.20 30.20 45.20 25.05 32.18 25.40 22.73 21.89 27.43 33.26 27.34 25.15 38.67 33.20 17.60 26.70 2.18 28.16 30.20 28.67 30.35 27.95 27.80 27.80 23.70 27.50 24.20 27.70 17.80 29.13 28.69 28.69 23.69 23.00 21.60 29.50 26.09 21.70 27.71 30.69 28.50 26.50 20.50 22.50 38.20 25.50 22.86 21.50 30.19 31.20 33.20 21.68 30.00 25.18 34.50 32.14 23.40 38.04 34.04 34.04 32.07 34.80 37.08 25.15 33.08 38.14 27.08 29.18 29.18 27.20 21.10 27.61 37.08 30.20 22.19 30.16 30.16 30.16 31.18 18.15 32.17 28.65 30.15 34.16 30.78 29.75 28.60 38.10 17.60 28.90 22.76 18.64 22.60 Data are reported as Ct values. Ct-cycle threshold: the lower the Ct value, the more DNA detected by a primer pair is present. SM:
and damage to nucleic acid, resulting in the death of bacteria (28). Furthermore, the photothermal effect is also induced after absorption of the laser beam by water, which causes microexplosions and breakup of the bacteria (29). Yamaguchi et al. (30) found that lipopolysaccharides in the cell membrane of gram-negative bacteria have a peak value of absorption of 2.92 mm, which is close to the wavelength of the Er:YAG laser. This specific laser removes 83.1% of lipopolysaccharides with a pulse energy of 100 mJ and frequency of 1 Hz. In this study, the pulse energy was 250 mJ, and the frequency 10 Hz, meaning that the bactericidal impact on the investigated gram-negative bacteria could be even more pronounced. It was also found that amines and amine groups that are present in bacteria also absorb the wavelength of the Er:YAG laser and this has a detrimental effect on bacteria due to the photochemical effect (31). Contrary to that, Valerio et al. (32) in their clinical study showed that affected dentin in the pulpal wall had similar amounts of S. mutans and Lactobacillus sp. comparing caries removal by Er:YAG laser and bur. In their study, microbiological analysis was performed by counting tested bacteria (32). However, inoculating cariogenic bacteria on culture medium in the laboratory might yield false positive results, because other bacteria, besides the tested ones, can grow on the same culture medium (33). The RT-PCR method, which was used in this study, is a more accurate method to detect clinically relevant cariogenic bacteria because it has a higher sensitivity and specificity in the detection of bacterial nucleic acids (34).
Temperature measurements showed the lowest values for the FFC Er:YAG group, probably due to a feedback control of the laser, which appeared to operate like a cut-off switch when infected dentin was eliminated (35) and stopped the laser from emitting energy intermittently. In this investigation, the threshold level was set at 7 according to the results of Krause et al. (26). They indi-cated that a fluorescence threshold level of 7 or 8 units
can guide an Er:YAG laser to a complete removal of car-ious dentin (26). Interestingly, for Er:YAG based on VSPt the lowest value of average temperature was measured for the MSP group, while there was no significant dif-ference between the SSP and SP groups. Diaci et al. (21) showed that shorter pulses with high energy enable a higher ablation rate of tissue than the diffusion of heat into the surrounding tissue. That causes less temperature rise compared to longer pulses like the SP used in this study. However, shorter pulses, like SSP, also decrease the time for cooling of hard dental tissue, which may explain the results of this study and the higher temperatures found for the shortest pulse. It should be emphasized that the infrared thermal camera measures the tem-perature in the center of the laser irradiation where the laser energy is maximal and produces large amount of heat, hence the temperature rise. These temperatures would be found in adjacent layers of dentin or in the pulp chamber.
Within the limitations of this study it was concluded that the Er:YAG lasers used in this study with different modes were efficient in removing cariogenic bacterial from infected dentinin vitro. In all treatment groups, cariogenic bacteria were completely removed. However, the lowest temperature rise was associated with the use of the FFC Er:YAG laser.
Based on thisin vitrostudy, laser treatment for removal of carious dentin and cariogenic bacteria seems to be an efficient treatment modality without causing excessive temperatures, which might adversely affect pulp vitality.
Aknowledgements
The authors wish to thank Fotona and Kavo for providing the laser equipment and Janez Žabkar for his support during temperature measurements. The authors wish to thank Professor Marijana Javornik Cubric for proof reading.
References
1. Stoll R, Urban-Klein B, Giacomin P, Loukas A, Jablonski-Momeni A. In vivoassessment of caries excavation with afluorescence camera compared to direct bacteriological sampling and quantitative analysis using flow cytometry.
Laser Med Sci 2015; 30: 843–849, doi:
10.1007/s10103-013-1459-2.
2. Banerjee A. Minimal intervention dentistry: part 7. Minimally invasive operative caries management: rationale and tech-niques.Br J Dent2013; 214: 107–111, doi: 10.1038/sj.bdj. 2013.106.
3. Almeida Neves A, Coutinho E, Cardoso MV, Lambrechts P, Van Meerbeek B. Current concepts and techniques for caries excavation and adhesion to residual dentin.J Adhes Dent2011; 13: 7–22, doi: 10.3290/j.jad.a18443.
4. Holmgren CJ, Roux D, Domejean S. Minimal intervention dentistry: part 5. Atraumatic restorative treatment (ART)- a
minimum intervention and minimally invasive approach for the management of dental caries.Br Dent J2013; 214: 11–18, doi: 10.1038/sj.bdj.2012.1175.
5. Macedo GV, Yamauchi M, Bedran-Russo AK. Effects of chemical cross- linkers on caries-affected dentin bonding.
J Dent Res 2009; 88: 1096–1100, doi: 10.1177/0022034
509351001.
6. Banerjee A, Kellow S, Mannocci F, Cook RJ, Watson TF. Anin vitroevaluation of microtensile bond strengths of two adhesive bonding agents to residual dentine after caries removal using three excavation techniques. J Dent 2010; 38: 480–489, doi: 10.1016/j.jdent.2010.03.002.
7. Hahn CL, Best AM, Tew JG. Cytokine induction by
Streptococcus mutans and pulpal pathogenesis. Infect Immun2000; 68: 6785–6789, doi:
8. Mertz-Fairhurst EJ, Curtis JW, Ergle JW, Ruggeberg FA, Adair SM. Ultraconservative and cariostatic sealed restora-tions: results at year 10.J Am Dent Assoc1998; 129: 55–66,
doi: 10.14219/jada.archive.1998.0022.
9. Nakajima M, Sano H, Burrow MF, Tagami J, Yoshiyama M, Ebisu S et al. Tensile bond strength and SEM evaluation of caries-affected dentin using dentin adhesives.J Dent Res
1995; 74: 1679–1688, doi: 10.1177/00220345950740100901. 10. Yoshiyama M, Doi J, Nishitani Y, Itota T, Tay FR, Carvalho RM et al. Bonding ability of adhesive resins to caries-affected and caries-infected dentin.J Appl Oral Sci2004; 12: 171–176, doi: 10.1590/S1678-77572004000300002.
11. Costa AR, Garcia-Goday F, Carrer-Sobrinho L, Naves LZ, Raposo LH, Carvalho FG et al. Influence of different dentin supstrate (caries-affected, caries-infected, sound) on long-termmTBS. Braz Dent J 2017; 28: 16–23, doi: 10.1590/
0103-6440201700879.
12. Hsu KW, Marshall SJ, Pinzon LM, Watanabe L, Saiz E, Marshall GW. SEM evaluation of resin-carious dentin inter-faces formed by two dentin adhesive systems.Dent Mater
2008; 24: 880–887, doi: 10.1016/j.dental.2007.11.001.
13. Yoshiyama M, Tay FR, Doi J, Nishitani Y, Yamada T, Itou K et al. Bonding of self-etch and total-etch adhesives to carious dentin.J Dent Res2002; 81: 556–560, doi: 10.1177/
154405910208100811.
14. Yoshiyama M, Tay FR, Torii Y, Nishitani Y, Doi J, Itou K et al. Resin adhesion to carious dentin.Am J Dent2003; 16: 47–52.
15. Wei S, Sadr A, Shimada Y, Tagami J. Effect of caries-affected dentin hardness on the shear bond strength of current adhesives.J Adhes Dent2008; 10: 431–440.
16. Scholtanus JD, Purwanta K, Dogan N, Kleverlaan CJ, Feilzer AJ. Microtensile bond strength of three simplified adhesive systems to caries-affected dentin.J Adhes Dent
2010; 12: 273–278.
17. Taniguchi G, Nakajima M, Hosaka K, Iwamoto N, Ikeda M, Foxton RM et al. Improving the effect of NaOCl pretreatment on bonding to caries-affected dentin using self-etch adhesives.
J Dent2009; 37: 769–775, doi: 10.1016/j.jdent.2009.06.005.
18. Kunawarote S, Nakajima M, Foxton RM, Tagami J. Effect of pretreatment with mildly acidic hypochlorous acid on adhe-sion to caries-affected dentin using a self-etch adhesive.
Eur J Oral Sci2011; 119: 86–92, doi: 10.1111/j.1600-0722.
2010.00788.x.
19. Yip HK, Samaranayake LP. Caries removal techniques and instrumentation: a review.Clin Oral Invest1998; 2: 148–154, doi: 10.1007/s007840050062.
20. Gurgan S, Kiremitci A, Cakir FY, Yazici E, Gorucu J, Gutknecht N. Shear bond strength of composite bonded to erbium:yttrium-aluminum-garnet laser-prepared dentin.Lasers Med Sci2009; 24: 117–122, doi: 10.1007/s10103-007-0532-0.
21. Diaci J. Laser profilometry for the characterization of craters produced in hard dental tissues by Er:YAG and Er,Cr:YSGG Lasers.J Laser Health Acad2008; 2: 1–9.
22. Medioni E, Rocca JP, Fornaini C, Merigo E. Histological evaluation of the three techniques for caries removal.J Oral Sci2016; 58: 583–589, doi: 10.2334/josnusd.16-0225.
23. Eberhard J, Eisenbeiss AK, Braun A, Herdderich J, Jepsen S. Evaluation of selective caries removal by afluorescence feedback-controlled Er:YAG laserin vitro.Caries Res2005; 39: 496–504, doi: 10.1159/000088186.
24. König K, Flemming G, Hibst R. Laser-induced autofl uores-cence spectroscopy of dental caries.Cell Mol Biol1998; 44: 1293–1300.
25. Zach L, Cohen G. Pulp response to externally applied heat.Oral Surg Oral Med Oral Pathol1965; 19: 515–530,
doi: 10.1016/0030-4220(65)90015-0.
26. Krause F, Braun A, Lotz G, Kneist S, Jepsen S, Eberhard J. Evaluation of selective caries removal in deciduous teeth by a fluorescence feedback-controlled Er:YAG laser in vivo.
Clin Oral Invest2008; 12: 209–215, doi:
10.1007/s00784-007-0169-1.
27. Eberhard J, Eisenbeiss AK, Braun A, Hedderich J, Jepsen S. Evaluation of selective caries removal by afluorescence feedback-controlled Er:YAG laserin vitro.Caries Res2005; 39: 496–504, doi: 10.1159/000088186.
28. Wilson M. Photolysis of oral bacteria and its potential use in the treatment of caries and periodontal disease.J Appl Bacteriol
1993; 75: 299–306, doi: 10.1111/j.1365-2672.1993.tb02780.x. 29. Ando Y, Aoki A, Watanabe H, Ishikawa I. Bactericidal effect of Erbium YAG laser on periodontopathic bacteria. Laser Surg Med1996; 19: 190–200, doi: 10.1002/(SICI)1096-9101
(1996)19:2o190::AID-LSM1143.0.CO;2-B.
30. Yamaguchi H, Kobayashi K, Osada R, Sakuraba E, Nomura T, Arai T, et al. Effects of irradiation of an erbium:YAG laser on root surfaces. J Periodontol1997; 68: 1151–1155, doi:
10.1902/jop.1997.68.12.1151.
31. Socrates G (Editor).Infrared and Raman characteristics group frequencies: tables and charts. New York, Wiley; 2001. 32. Valerio RA, Borsatto MC, Serra MC, Polizeli SA, Nemezio
MA, Galo R, et al. Caries removal in deciduous teeth using an Er:YAG laser: a randomized split-mouth clinical trial.Clin Oral Invest2016; 20: 65–73, doi: 10.1007/s00784-015-1470-z.
33. Cappelli DP, Mobley CC. Prevention in clinical oral health care. St. Louise, Mosby Elsevier; 2008.
34. Suzuki N, Yoshida A, Nakano Y. Quantitative analysis of multi-species oral biofilms by TaqMan real-time PCR. Clin Med Res2005; 3: 176–185, doi: 10.3121/cmr.3.3.176. 35. Schwass DR, Leichter JW, Purton DG, Swain MV.
Evaluat-ing the efficiency of caries removal using an Er:YAG laser driven by fluorescence feedback control. Arch Oral Biol