w w w . r b o . o r g . b r
Original
Article
Evaluation
of
treatment
for
camptodactyly:
retrospective
analysis
on
40
fingers
夽,夽夽
Saulo
Fontes
Almeida,
Anderson
Vieira
Monteiro,
Rúbia
Carla
da
Silva
Lanes
∗InstitutoNacionaldeTraumatologiaeOrtopedia,RiodeJaneiro,RJ,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received18October2012 Accepted13May2013 Availableonline15March2014
Keywords:
Handdeformities, congenital/pathology Handdeformities, congenital/therapy Fingers/abnormalities
a
b
s
t
r
a
c
t
Objective:toretrospectivelyassesstheresultsfromcasestreatedinthehandsurgeryservice, startingfromapreestablishedprotocol;andtoconductacriticalanalysisontheresults achieved,withseparationofthecasesintotheirrespectivesubgroups.
Methods:twenty-threepatientsandatotalof40fingerswereevaluatedbetweenJanuary 2004andDecember2011.Wecorrelatedthealteredanatomicalstructuresfoundinthecases thatunderwentthesurgicalprocedureanditsresults,withregardtobothconservativeand surgicaltreatment,emphasizingthemainindications.
Results:theresultswereanalyzedusingtheSiergetmethodoftheMayoClinic.
Conclusion:weobservedthatthecasesofcamptodactylyofthelittlefingeraloneinthe flex-ibleform(>60◦)thatunderwentsurgicaltreatmentuniformlypresentedexcellentresults.
Intherigidforms,ourobservationsindicatedthattherewerebenefitscomprisinggainsof extensionandcorrectionofthedeformity.However,therangeofmotionwithactiveflexion intheproximalinterphalangealjointwasalwayspartial.Withevolutionovertime,some casespresentedsomelossofthegainpreviouslyachieved,whichcorroboratestheneedfor continualvigilanceduringthefollow-up,withsystematicuseofbracesuntilthefinalphase ofskeletalgrowth.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Avaliac¸ão
do
tratamento
da
camptodactilia:
análise
retrospectiva
de
40
dígitos
Palavras-chave:
Deformidadecongênitada mão/patologia
Deformidadecongênitada mão/terapia
Dedos/anormalidades
r
e
s
u
m
o
Objetivos:avaliar,retrospectivamente,osresultadosdoscasostratadosnoservic¸ode Cirur-gia da Mão, a partirde um protocolopreestabelecido; e fazeruma análise crítica dos resultadosalcanc¸ados,comaseparac¸ãodoscasosemseusrespectivossubgrupos.
Métodos:foramavaliados23pacientes,numtotalde40dígitos,dejaneirode2004adezembro de2011.Relacionamosasestruturasanatômicasalteradasencontradasnoscasosqueforam submetidosaprocedimentocirúrgicoeseusresultados,tantonotratamentoconservador comonocirúrgico,eenfatizamossuasprincipaisindicac¸ões.
夽
Pleasecitethisarticleas:AlmeidaSF,MonteiroAV,LanesRCS.Avaliac¸ãodotratamentodacamptodactilia:análiseretrospectivade40 dígitos.RevBrasOrtop.2014;49:134–139.
夽夽
WorkperformedattheHandSurgeryCenter,InstitutoNacionaldeTraumatologiaeOrtopedia,RiodeJaneiro,RJ,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](R.C.d.S.Lanes).
Resultados: osresultadosforamanalisadospelométododeSiergetdaclínicaMayo.
Conclusão: observamosqueoscasosdecamptodactiliaisoladadodedomínimonaforma flexível,>60◦,queforamsubmetidosatratamentocirúrgicodemaneirauniforme
apresen-taramresultadosexcelentes.Nasformasrígidas,nossasobservac¸õesindicambenefícios comganhodeextensãoecorrec¸ãodadeformidade.Entretanto,oarcodemovimentocom flexãoativanainterfalângicaproximal(IFP)ésempreparcial.Comotempodeevoluc¸ão, algunscasosapresentaramalgumaperdadoganhopreviamentealcanc¸ado,oquecorrobora apermanentevigilâncianecessárianoacompanhamento,comusosistemáticodeórteses, atéafasefinaldocrescimentoesquelético.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Camptodactylyisacongenitaldeformitycharacterizedbya flexedpostureintheproximalinterphalangealjoint.Itis gen-erallyfoundinthelittlefingerandmayormaynotincludethe otherfingers.Itispainlessandnontraumatic.1–9
Itaffectsapproximately1%ofthepopulation.8,10Itis
bilat-eralinaroundtwothirdsofthepatients,althoughthedegree ofcontractureisusuallynotsymmetrical.8,11,12
Thedeformitygenerally increasesduringgrowthspurts, especiallyduringtheperiodsofrapidgrowthfromonetofour yearsandfrom10to14yearsofage.5,11,13
The primary cause of this deformity is still a matter fordiscussionand thereisnoconsensusinthe worldwide literature.3,4,8,10–13 Although somecases occur sporadically,
thereisoftenanautosomalinheritancepatternpresent.4,7,8,14
The metacarpophalangeal and distal interphalangeal jointsare unaffected,although theymay develop compen-satorydeformities.12
AccordingtoSiergertetal.,7camptodactylycanbedivided
intosimpleandcomplextypesfromaclinicalpointofview. Thesimpletypeconsistsofflexedcontractureoftheproximal interphalangeal joint.In complexcamptodactyly, there are otherassociateddeformitiessuchassyndactylyora combina-tionofclinodactylyandcamptodactyly.7,10Glicensteinetal.15
classifiedcamptodactylyinto:
Primitive:whenitappearsinthefirstyearsoflife.Itaffects bothsexesinthesameproportionsandevolveswith skele-talgrowth. Itmay alsoappearclosetoadolescence, with clearpredominanceinfemales.Itisfrequentlybilateral.It isrestrictedtothelittlefingerandprogressesrapidlyduring thegrowthspurt.
Secondary:associatedwithsyndromesandother malforma-tionsandnormallyinvolvesmorethanonefinger.Themost frequentassociationsare:radialclubhand, oculodentodigi-talsyndrome,Marfansyndromeandarthrogryposis.15,16
In1994,Bensonetal.17classifiedcamptodactylyasfollows:
TypeI:Thisisthecommonestformanditbecomesevident duringchildhood.Itgenerallyaffectsthelittlefingeralone. Itaffectsboysandgirlsequally.
TypeII:Camptodactylyofadolescence,whichoccurs predom-inantlyinfemales.Clinically,itresemblestypeI.Itdevelops betweentheagesofsevenand elevenyears,starting sub-tlyandevolvinggraduallyandprogressively.Itaffectsgirls
morethanboys.Thistypeofcamptodactylygenerallydoes notimprovespontaneouslyandmayevolvetosevereflexed deformity.
Type III: This ispresent from thetime ofbirth. Itusually affectsseveralfingers.Itisconstantlybilateral,with accentu-atedfixedforms.Itisassociatedwithavarietyofsyndromes andothermalformations.8,12,16,17
The degree ofinvolvement between the hands is often asymmetrical.
Inageneralmanner,the classificationshavethe aimof groupingdifferentcasesofcamptodactylyandfromthis,to establishatreatmentprotocol.
Main
problems
and
justifications
Several formsoftreatment forcamptodactyly havealready been proposed. Many published studies have emphasized conservativetreatment,whileothershavedescribedsurgical procedures.
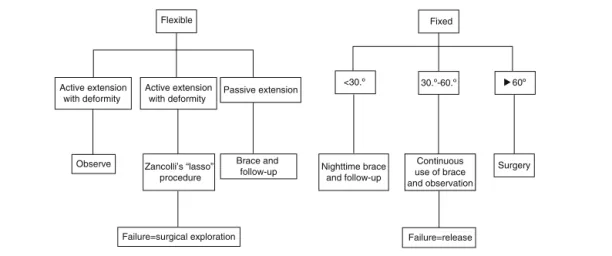
Theproblemwiththisdeformityisthatseveralformsof presentationexist,whichmeansthatthereisnosinglemodel foreffectivetreatment(Fig.1).
Objectives
Theaimofthisstudywastoretrospectivelyevaluatecasesthat hadbeentreatedattheHandSurgeryServiceusinga preestab-lishedprotocol,andtoconductacriticalanalysisontheresults achieved.
Flexible Fixed
<30.º 30.º-60.º Active extension
with deformity
Active extension
with deformity Passive extension
Brace and
follow-up Nighttime brace and follow-up
Continuous use of brace and observation
Surgery
Failure=release Observe Zancolli’s “lasso”
procedure
Failure=surgical exploration
60º
Fig.2–Flowdiagramofthetreatment.
Materials
and
methods
Twenty-three patients(40 fingers)who were treatedatthe HandSurgeryService,InstitutoNacionaldeTraumatologiae Ortopedia,RiodeJaneiro,wereselected.
Allthepatientshadbeentreatedandfollowedupbythe supervisorinchargeofthisprojectandbytheco-supervisor oftheprojectsince2004,inconformitywiththeparameters preestablishedinthetreatmentprotocoldescribedbelow.
Wemadean initialclinicalassessmentand divided the casesintoreducibleforms(flexible)andnon-reducibleforms (fixed), by means of a physical examination. Among the reduciblecases,wedividedthepatientsintotwosubgroups andproposedthefollowingtreatment:
If,throughstabilization ofthemetacarpophalangealjoint, activeextensionofinterphalangealjointwouldbecome pos-sible,weindicatedconservativetreatmentforcasesofless than30◦ ofdeformity;fordeformitiesgreaterthan30◦,we
indicatedZancolli’s“lasso”procedure.
If,aftercorrectionofthedeformity,extensionofthe inter-phalangeal joint would only be possible passively with flexionofthemetacarpophalangealjoint,weinstituted con-servativetreatmentconsisting ofstretching exercisesand useofbraces.Ifconservativetreatmentfailed,wewould indi-catesurgicalexploration,inordertosearchforanomaliesin thesuperficialflexorsand/orlumbricals.
Amongthenon-reduciblecases,i.e.fixedforms,wedivided thepatientsintothreesubgroupsandproposedthefollowing treatment:
Deformitylessthan30◦:thetreatmentwaslimitedto
observa-tion,stretchingexercisesanduseofanighttimebrace.
Deformitybetween30◦and60◦:conservativetreatment,with
continuoususeofabraceandmonitoringoftheevolution ofthedeformity.Incasesoffailure,surgicaltreatmentwas instituted.
Deformitygreaterthan60◦:intheseseverecases,inwhichit
wasimpossibletoadequatelyfitabrace,weindicated surgi-caltreatment,withen-blocreleaseofthestructuresofthe volarfaceofthefinger(Fig.2).
Wesoughttocorrelatethealteredanatomicalstructures foundinthecasesthatunderwentthesurgicalprocedure;and toreporttheresultsfrombothconservativeandconservative treatment.
WeanalyzedtheresultsusingthemethodofSiergetetal.,7
fromtheMayoclinic:
Excellent:Fullcorrectionofextensionwith<15◦lossofflexion
oftheinterphalangealjoint.
Good:Correctionwithlossofupto20◦ofextensionandgain
ofextensionoftheinterphalangealjoint>40◦,withlossof
flexion<30◦.
Fair:Correctionwithlossofextensionofupto40◦andgain
ofextensionoftheinterphalangealjoint>20◦,withlossof
flexion<45◦.
Poor:Correctionwithgainofextensionoftheinterphalangeal joint<20◦,withrangeofmotion<40◦.5,7,8,12
Results
Twenty-threepatientswereevaluated:12females(52.17%)and 11males(47.82%)(Fig.3).
Female 52% Gender
Male 48%
Unilateral
Bilateral
Fig.4–Bilateralversusunilateralimpairment.
Thirteenpatients(56.52%)wereaffectedbilaterally.When patientswere affected unilaterally,this occurred more fre-quentlyontherightside(56.5%)(Fig.4).
Thefingermostaffectedwasthelittlefinger,withatotal of34cases(85%);andtheringfingerwasinsecondplace,in fivecases(14.6%)(Fig.5).
TenpatientswereclassifiedasBensontypeI(42.5%),which wasevidentduringinfancy;eightastypeII(35%),which devel-opedbetweentheagesofsevenandelevenyears;andonlyfour patientsastypeIII(10%),whichhadbeenpresentsincebirth (Fig.6).
Outofthe40fingersevaluated,16werereducible.With sta-bilizationofthemetacarpophalangealjoint,onlyonefinger presentedactiveextensionoftheinterphalangealjoint,with deformity>30◦.Inthis case,weindicatedZancolli’s“lasso”
procedure.Duringtheoperation,weencounteredan abnor-malityinthelumbricals(Fig.7).Theresultwasexcellent,with fullcorrectionofextension.
Theother15 fingersthat werereducible onlypresented extensionofthe interphalangealjoint,withpassiveflexion ofthemetacarpophalangealjoint.In thesecases,we insti-tutedconservativetreatmentusingbraces(Fig.8AandB)and stretchingexercises.
Ineightfingers,weobtainedanexcellentresultandintwo, agodresultwithlossofextensionofnotmorethan20◦and
againofextensionoftheproximalinterphalangealjointof morethan40◦,withlossofflexionoflessthan30◦.
Threepatientsabandonedthetreatmentandtwofingers hadpoorresults,withcorrectionproducingagainofextension
Minimum Anular
35
30
25
20
15
10
15
0
Little finger
Ring finger
Fig.5–Fingermostaffected.
Type I Benson
Type III Type II
Fig.6–DistributionaccordingtoBensonclassification.
oftheproximalinterphalangealjointoflessthan20◦,witha
rangeofmotionoflessthan40◦.Inthesecases,weindicated
surgicalexploration.Inbothcases,weperformedZancolli’s procedure.Inonecase,abnormalinsertionofthelumbricals wasfound.Onefingerpresentedanexcellentresult,withfull correctionofextension,andtheotherevolvedwithscar retrac-tionduringthepostoperativeperiod.
Theother23fingerswereirreducible.Onepresented defor-mity oflessthan 30◦ andanexcellent resultwasobtained
throughconservativetreatment.
Fourteen patients presenteddeformities ofbetween30◦
and60◦.Weinstitutedcontinuoususeofbracesandfollowed
up the cases. Eight casesofdeformity evolvedwith excel-lentresults;twopatientsabandonedthetreatment;andfour evolvedwithapoorresultandsurgicalexplorationwas indi-cated.Amongthese,thevolarreleasetechniquewasusedin threecases,whichproducedexcellentresultsinonecase,with lossofflexion oftheinterphalangeal jointofless than15◦
andfullextension;andgood resultsintwocases,withloss offlexionoftheinterphalangealjointoflessthan30◦.
Fig.8–Brace.
Duringthesurgicalprocedure,wefoundonecaseof abnor-malinsertionofthelumbricalsandonewithahypoplastic superficialflexor.
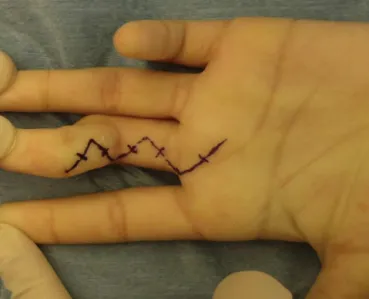
Eightfingerspresenteddeformitiesgreaterthan 60◦ and
en-blocreleaseofthestructuresofthevolarfaceofthefinger wasindicated(Figs.9and10).
Inthreefingers,abnormalinsertionofthelumbricalswas encountered.Weobtainedanexcellentresultinthreecases ofdeformityandagoodresultinonefinger.Threepatients abandonedthetreatment,evenbeforethesurgery,andone abandoneditafterthesurgicalprocedure.
Fig.9–Volaraccess.
Fig.10–Releaseofvolarstructures.
Discussion
Thedegreeofflexionoftheproximalinterphalangeal joint incamptodactylycasesiscorrectlyassessedifthewristand metacarpophalangeal joints are placedinneutral position. Deformities<30◦ donotrequiretreatment,whilethose>60◦
interferewithfunction.
TheradiographicassessmentisdoneintheAPandlateral viewsofthefinger,inordertoexaminetheconfigurationof the proximalinterphalangealjointset.Thealterationsthat can be observed and which are generally associated with severe contracturesare wideningofthebaseofthemiddle phalanxwithanotchonitsjointsurfaceandachiseledcut on thehead oftheproximal phalanxwithflattening ofits surface.8,18,19
Theclinical characteristics thatshouldbe observedand which guidethe treatmentare jointreducibility(flexibility) andthedegreeofdeformity.Theflexedpostureofthe prox-imalinterphalangealjointmaybereducible,i.e.passivelyor activelyflexible,orirreducible,i.e.fixed,whenextensionof thejointaffectedisnotachieved.16Inmostcases,theflexion
movementisnotaffected.
Thiscongenitaldeformityofrelativelysimpleappearance hasseveral typesofpresentationandisextremelydifficult totreat.8,13Thefamilyshouldbeadvisedthatthetreatment
is long and that follow-up throughout the skeletal growth periodisnecessary;moreover,afterpartialortotalcorrection, relapsesmayoccur.5
Manystudieshavedemonstratedsuccessthrough conser-vative treatmentconsistingofuse ofbracesand stretching exercises.3,5,8,13Forsmallerchildren,thebraceshouldinclude
the hand and the wrist. This brace is initially used dur-ing the maximum periodof acceptance,with intervals for stretchingexercisesguidedbytherapists,untilthedeformity hasbeencorrected.13,18Theimportanceoftheparentswith
underestimated,because aggressive stretching could cause painandtissuedamage.5
Ata later stage, to avoid recurrence, the brace isused forshorterperiodsduringtheday.However,nighttimeuseis maintaineduntiltheendoftheskeletalgrowthperiod.8,12,13,16
Surgical treatment is reserved for specificcases and in casesoffailureofconservativetreatment.3,5,7,8,13,16
Boneabnormalitiesarenotacontraindicationforsurgery, buttheresultexpectedwillbegreatlydiminished.12
Thesurgical procedures can bedescribed as those that attempttoidentifyaprimary cause;those thatattempt to rebalancetheinterphalangealjointthroughtransferring flex-ionforcetotheextensorsurface;thosethatprovideen-bloc releaseofall ofthe structuresofthevolarfaceinorder to achieve correction; and bone procedures withdorsal-angle osteotomyoftheneckoftheproximalphalanx.3,16
Ifactiveextensionispossible,withcorrectionofthe defor-mityandplacementofthemetacarpophalangealjointinslight flexion,theproblemisfoundinstabilizingthe metacarpopha-langealjoint,inanalogywithanulnarclaw.Thesecaseswould gain effective benefit from the “lasso” surgical procedure thatwasdescribedbyZancolliapudAdams8andMcFarlane
etal.19
Ifthedeformitycanonlybereducedpassively,with place-mentofthewristormetacarpophalangealjointinflexion,it canbeassumedthatthestructureresponsibleforcontraction crossesthejointsabovetheflexorsurface.Thepossibilitiesare thatthelumbricalmusclehasanabnormaloriginorinsertion, orthatthesuperficialflexorisabnormallyfixed.
Surgerytotreatcamptodactyly,especiallyincasesofsevere contracture,hasseveralcomplication,suchaslesionsof neu-rovascularstructures,scartensionduringextensionandloss offlexion.
Incomplete extension is better tolerated than deficient flexion.Early mobilization should beinstituted in order to promoterestorationofflexion.8,10
Thereturnofthesetofmovementsofthedeepflexorof thefingersandtheproximalinterphalangealjointisslowand maytakesixtotwelvemonthsinpatientswhoaretreated surgically.8
Conclusion
Accordingtoourobservationsfromoutpatientreview consul-tations,weconcludedthatthecasesofcamptodactylyinthe littlefingeralone,intheflexibleform(>60◦),whichunderwent
surgicaltreatmentinauniformmanner,presentedexcellent results.
Intherigidforms,ourobservationsindicatedthat there were benefitsrelatingto gains ofextensionand correction ofthe deformity.However,therange ofmotionwithactive flexionoftheproximalinterphalangealjointwasalways par-tial,i.e.eveninthecaseswithexcellentresults,therewasan averagelossofflexionof15◦.
Overtime,somecasesevolvedtopresentsomelossofthe gainthathadpreviouslybeenachieved,whichemphasizesthe needforcontinualfollow-upmonitoring,withsystematicuse ofbraces,untilthe finalphaseofskeletal growthhasbeen reached.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.FoucherG,LoréaP,KhouriRK,MedinaJ,PivatoG. Camptodactylyasaspectrumofcongenitaldeficiencies:a treatmentalgorithmbasedonclinicalexamination.Plast ReconstrSurg.2006;117(6):1897–905.
2.EkblomAG,LaurellT,ArnerM.Epidemiologyofcongenital upperlimbanomaliesin562childrenbornin1997–2007:a totalpopulationstudyfromStockholm,Sweden.JHandSurg Am.2010;35(11):1742–54.
3.MedinaJ,PajardiG.Analgorithmfortreatmentof
camptodactylybasedonareviewof135fingerstreatedin109 patients.JHandSurgBr.1994;28:36.
4.MinamiA,SakaiT.Camptodactylycausedbyabnormal insertionandoriginoflumbricalmuscle.JHandSurgBr. 1993;18(3):310–1.
5.RheeSH,OhWS,LeeHJ,RohYH,LeeJO,BaekGH.Effectof passivestretchingonsimplecamptodactylyinchildren youngerthanthreeyearsofage.JHandSurgAm. 2010;35(11):1768–73.
6.GoldfarbCA.Congenitalhanddifferences.JHandSurgAm. 2009;34(7):1351–6.
7.SiegertJJ,CooneyWP,DobynsJH.Managementofsimple camptodactyly.JHandSurgBr.1990;15(2):181–9.
8.AdamsBD.Congenitalcontracture.In:WolfeSW,Hotchkiss RN,PedersonWC,KozinSH,editors.Green’soperativehand surgery.6thed.Philadelphia:ChurchillLivingstone/Elsevier; 2011.p.1443–51.
9.ReichertB,BrennerP,BergerA.Considerationsonetiology, correctionandtreatmentofcamptodactyly.JHandSurgBr. 1994;19:9.
10.SmithPJ,GrobbelaarAO.Camptodactyly:aunifyingtheory andapproachtosurgicaltreatment.JHandSurgAm. 1998;23(1):14–9.
11.GuptaA,BurkeFD.Correctionofcamptodactyly.Preliminary resultsofextensorindicistransfer.JHandSurgBr.
1990;15(2):168–70.
12.ScottBD.Camptodactylyandclinodactylyinhandsurgery.In: BergerRA,WeissAP,editors.Handsurgery.Philadelphia: LippincottWilliams&Wilkins;2004.p.1478–91.
13.OginoT,KatoH.Operativefindingsincamptodactylyofthe littlefinger.JHandSurgBr.1992;17(6):661–4.
14.ObergKC,FeenstraJM,ManskePR,TonkinMA. Developmentalbiologyandclassificationofcongenital anomaliesofthehandandupperextremity.JHandSurgAm. 2010;35(12):2066–76.
15.MonteiroAV,AlmeidaSF.Deformidadescongênitasdo membrosuperior.In:PardiniAG,FreitasA,editors.Cirurgia damão:lesõesnãotraumáticas.2a.ed.RiodeJaneiro: Medbook;2008.p.206–8.
16.GlicensteinJ,HaddadR,GueroS.Surgicaltreatmentof camptodactyly.AnnChirMainMembSuper.
1995;14(6):264–71.
17.BensonLS,WatersPM,KamilNI,SimmonsBP,Upton3rdJ. Camptodactyly:classificationandresultsofnonoperative treatment.JPediatrOrthop.1994;14(6):814–9.
18.MiuraT,NakamuraR,TamuraY.Long-standingextended dynamicsplintageandreleaseofanabnormalrestraining structureincamptodactyly.JHandSurgBr.1992;17(6):665–72.