w w w . r b o . o r g . b r
Update
Article
Current
possibilities
for
hip
arthroplasty
夽,夽夽
Giancarlo
Cavalli
Polesello
∗,
Rodrigo
Pereira
Guimarães,
Walter
Ricioli
Júnior,
Nelson
Keiske
Ono,
Emerson
Kiyoshi
Honda,
Marcelo
Cavalheiro
de
Queiroz
FaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received16June2013 Accepted21June2013 Availableonline3April2014
Keywords:
Hipjoint/surgery Arthroscopy Hipinjuries
a
b
s
t
r
a
c
t
Hiparthroscopyhasbeenpopularizedoverthelastdecadeand,withtechnicaladvances regarding imaging diagnostics, understandingof the physiopathology or surgical tech-niques, several applications have been described. Both arthroscopy for intra-articular conditionsandendoscopyforextra-articularprocedurescanbeusedindiagnosingor treat-ingdifferentconditions.Thisupdatedarticlehastheobjectiveofpresentingthevarious currentpossibilitiesforhiparthroscopy.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Possibilidades
atuais
da
artroscopia
do
quadril
Palavras-chave:
Articulac¸ãodoquadril/cirurgia Artroscopia
Lesõesdoquadril
r
e
s
u
m
o
Aartroscopiadequadriltemsidopopularizadanaúltimadécadaecomoavanc¸otécnico, sejanodiagnósticoporimagem,noentendimentodafisiopatologiaounatécnicacirúrgica, diversas aplicac¸õesforamdescritas.Tantoa artroscopia,paraafecc¸õesintra-articulares, comoaendoscopia,paraprocedimentosextra-articulares,podemserusadasno diagnós-ticoounotratamentodediferentesafecc¸ões.Esteartigodeatualizac¸ãotemcomoobjetivo apresentardiversaspossibilidadesatuaisdaartroscopiadequadril.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevierEditora Ltda.Todososdireitosreservados.
Introduction
Hiparthroscopy hasbecomepopularover the past decade and, with technical advances in imaging diagnostics,1 in
understandingthephysiopathologyorinsurgicaltechniques, several applications have been described.2,3 It was first
describedbyBurmanin1931(inByrdetal.4),whoconsidered
夽Pleasecitethisarticleas:PoleselloGC,PereiraGuimarãesR,RicioliJúniorW,KeiskeOnoN,KiyoshiHondaE,CavalheirodeQueiroz
M.Possibilidadesatuaisdaartroscopiadoquadril.RevBrasOrtop.2014;49:103–110.
夽夽WorkperformedintheHipGroup,DepartmentofOrthopedicsandTraumatology,SchoolofMedicalSciences,SantaCasadeSãoPaulo,
SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](G.C.Polesello).
thatthecapacityofthistechniqueforenablingviewingwas extremelylimitedandthatthismethodwaspotentially iatro-genic.Duringthe1980sand1990s,thereweredevelopments in traction techniques that facilitated access to the cen-tralcompartment.5,6Sincethen,betterunderstandingofthe
arthroscopicanatomyoftheperipheralcompartmentanduse ofarthroscopywithouttractionhaveprovidedanenvironment thatisfavorabletowardwide-rangingjointexploration.7Once
2255-4971/$–seefrontmatter©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
theunderstandingofthearthroscopicanatomyofthese com-partmentshadbecomewellestablished,therewasanatural expansionofendoscopicexplorationtoothercompartments aroundthehip,suchastheperitrochanteric,subglutealand medialspacesofthehip.8–10
Thearthroscopicanatomyisalreadywellknown.11
Mul-tipleportalsarepossibleandarewelldefinedwithregardto theirsafety,12 asisthe anatomicaltechniqueinrelationto
preservationofthevascularizationofthefemoralneck.13,14
Indications
Lesionsoftheacetabularlabrum
This is one of the commonest indications.15 The labrum
functionsasajointseal,helpsinproducingandenabling cir-culationofthesynovialfluidandallowscontinuallubrication ofthejoint.16Inadditiontoitsproprioceptivefunction,itadds
stability tothe joint because ofthe vacuum phenomenon, deepensthe hip joint,provides greater uniformityof pres-suredistributionandincreasesthecontactsurfacebetween thefemoralheadandtheacetabulumby22%.17,18
Lesionsoftheacetabularlabrummayoccurduetodirect traumaduringsportsactivities.Infact, theselesions rarely occurintheabsenceofmorphologicalalterationstobones.19
Thus,thearthroscopicresultsfromlabraldebridementalone, without treating the underlying bone dysmorphism, are unsatisfactory.20 In mostcases, femoroacetabular
impinge-ment(FAI)makestheacetabularlabrumthefirststructureto fail.21
Theselesionsmay compromisethe loadabsorptionand stabilizationfunctionoftheacetabularlabrumandmaylead to arthrosis, as also found with meniscal lesions.22 Finite
element studies16,17 have demonstrated that if the sealant
function of the labrum is compromised, the mechanical demandsontheunderlyingcartilageareincreased,alongwith shearingforces,whichmaycontributetowardcausinginjury duetocartilagefatigueandsubsequentarthrosis.23
InadditiontoFAI,labrallesionsmayoccurduetorepetitive microtrauma, of either high or low-energy nature, espe-ciallythroughhiptorsionmechanisms.Repetitiveactivities, whetherinsportsornot,whichforcethehipbeyondthe habit-ualrangeofmotion,especiallyintohyperflexionofthehip, maycauseinjuries.Thesemechanismsmayincludeactivities suchasperforminglegpressexercises,ballet,yoga,spinning exercise,othergymactivities,dancing,workinginasquatting positionandothers.24–28
Theclinicalconditiongenerallyconsistsofanteriorpainin thehip,whichmayirradiatetothegroin,trochantericregion orposteriorregionofthehip.Onefrequentclinicalsignisthe “C”sign,inwhichthepatientpointsoutthelocationofthe paininhishipwithhishandina“C”shape,intransverse ori-entationoverthehipandtrochantericregion,whichdenotes painofintra-articularorigin.29
In the treatment, the major objective is to preserve as muchoftheviabletissueaspossible,withselective debride-ment,reinsertionorlabralreconstruction.Studiescomparing clinical resultsfrom debridement versus labralrepair have demonstrated that the best results are obtained through repair.30,31 Evidence thatlabral reconstruction,using either
autologousorhomologoustissue,maypresentgoodresults in patients withprevious labral resection, ossifiedlabra or hypotrophiclabrahasalsostartedtoappear.32–34
Femoroacetabularimpingement(FAI)
GanzrecognizedthatFAIcouldleadtodevelopmentoflabral lesions and earlyarthrosis innon-dysplastichips.35,36 This
concept is dynamic, based on movement more than axial loadingofthehip.Itmay resultfrommorphological abnor-malities thataffecttheacetabulumand proximalfemur, or it mayoccur inpatientswho subjecttheirhips toextreme andsupraphysiologicalrangesofmotion.Dependingonthe underlyingcause,FAImayresultinlesionsofthelabrumand acetabularcartilage.37Aftertheinjuryhasoccurred,synovial
fluidstarts tocirculatethroughthelesion,inacontinuous valvularmechanism. Ifthelow potentialforhealinginthe intra-articularenvironmentisaddedtothis,these hydrody-namicalterationsandthebonedysmorphismwillperpetuate theacetabularchondrallesionanditsdelaminationofthe sub-chondralbone,untilthecompensatorymechanismsceaseto operate,whichleadstoarthrosis.
Twodistincttypesoffemoroacetabularimpingementhave been identified,35 andtheyare frequently combined.38 The
firsttypeischaracterizedbylinearimpingementofthe acetab-ularrimagainstthefemoralhead–neckjunction,becauseof localacetabularsupercoverage(e.g.acetabularretroversion) or overallsupercoverage (e.g. deepthighor acetabular pro-trusion),calledapincerorapinchingeffect.Thesecondtype occurswithcompressionofthenon-sphericalextensionofthe femoralheadintotheacetabularcavity,whichiscalledCam. Changes to the femoral and acetabular anatomical for-mat may also result from childhood diseases such as Legg–Calvé–Perthes, epiphysiolysis, changes in inclination andacetabularorfemoralversion.39
Inrelationtotheclinicalcondition,patientscomplainof anteriorandlateralpaininthehip.Intheanterior impinge-menttest,whichisdonewithmaximuminternalrotationand 90◦ of passiveflexion ofthe hip, diminishedinternal
rota-tionofthehipandassociatedpainareobserved.Flexionand adduction ofthe hip lead to conflictbetween the femoral neckandtheacetabularrim.Internalrotationandassociated adduction cause shearing forces in the acetabularlabrum, similartothoseinthemenisci oftheknees,andstimulate thenerveends. Thiscausesacuteinguinalpaininpatients withatornordegeneratedlabrum21(Fig.1).
Thearthroscopictreatmentforfemoroacetabular impinge-ment consists of elimination of the bone conflict and correctionofthedeformities,bothontheacetabularsideand onthe femoralside,along withtreatmentoflesionsofthe chondrolabralcomplexbymeansofosteoplastyofthe proxi-malfemur,osteoplastyoftheacetabularsupercoverageand refixation, reconstruction or labral debridement and treat-mentofthechondrallesions.40,41
Pyoarthritis
Fig.1–Appearanceoftheimpingementtestinthephysical
examinationofthehip,whichisdonewiththehipflexed
at90◦,internalrotationandadduction.
time,betterviewingandeffectiveirrigationofthejoint,the possibilityofimplantingcontinuousirrigationcatheters,the possibility of collecting material for culturing and anato-mopathological examination, and minimal morbidity.42–47
Althoughtherehavebeenfewstudiesonarthroscopic treat-mentofpyoarthritisinadults,goodresultshavebeenobtained providedthattheinterventionwasearly.48,49Amongchildren,
somecomparativestudieshavedemonstratedthesuperiority ofarthroscopic drainage over open drainage. The possibil-ityofdrainage ofacuteinfection alsoexists withtotalhip arthroplasty.50
Arthrosis
Thereissomecontroversyregardinguseofarthroscopyon thehip inthepresenceofosteoarthrosis.Theresultsfrom treatingFAIinthepresenceofadvancedarthrosis,withlossof jointspace,arenotgood.51,52Ontheotherhand,McCarthyand
Lee53describedgoodresultsfromdebridementofosteophytes
anddegeneratedlabraincasesofarthrosisintheinitialstage, i.e.withoutlossofjointspaceonsimpleradiographs(Tönnis classificationtype0and1).54Jointpinchinggreaterthan50%
comparedwiththe contralateralside,orless than2mmof jointspaceremaining,alongwithlimitedrangeofmotion,41
isapoorprognosticfactor.51
Inthelightofpoorresultsandhighratesofconversionto hiparthroplastywithinathree-yearperiod,treatmentforhips witharthrosisshouldhaveveryrestrictedindications.55,56
Freebodies
Hiparthroscopyisanexcellenttoolforremovingfree bod-iesfromthehipjoints,whichcouldbeboneorosteochondral fragmentsresultingfromhipdislocation,firearmprojectiles, synovialchondromatosis, brokenguidewiresor othertypes offoreign bodiesof joints,57–64 thus enabling effective and
completeremovalofthefreebodies,synovectomyandrapid rehabilitation64–69(Fig.2).
Tumorsandotherconditions
Hiparthroscopycanbeusedinselectedcases.Itisalsoan optionfortreatingpigmentedvillonodularsynovitis,synovial chondromatosisandosteoidosteomaofthehip.64,70–73
Impingementofthetendonoftheiliopsoas muscle/internalprominence
Compressionofthetendonoftheiliopsoasmuscleinthe ante-rior capsuleofthe hipand consequentlyin theacetabular labrummaycauselabrallesionsintheanteromedialregion andevenbonedeformityinthefemoralhead,whichisatypical (Fig.3).
Audible and/or palpable internal prominences may be associatedwiththe anteriorregionofthe hip.For selected patients,debridementorlabralrepairtogetherwithtenotomy ofthe psoasmay producegoodresultsinpatients without any improvementthrough conservativetreatment. Internal prominencesarecharacterizedbyprominenceofthetendon oftheiliopsoasovertheiliopectinealeminence.Intheabsence ofimprovementthroughconservativetreatment,tenotomyof thepsoascanbeperformed,eitherasanintracapsular proce-dureoratthelevelofthelessertrochanter,withsatisfactory results.74,75
Dysplasia
Patients with dysplasia generally have hypertrophy of the acetabularlabrumduetoshearingofthefemoralhead,caused by lack ofacetabular coverage.This shearing gives rise to excessive mechanicaldemands atthechondrolabral transi-tionandmyxoiddegenerationoftheacetabularlabrumand/or deinsertionattheacetabularrim.76
Somecareshouldbetakeninindicatingarthroscopyfora dysplastichip.Capsulotomyandlabraldisordermayresultin
progressionofthearthrosis,worseningofthepainandjoint instability.In casesofdysplasiawitha Wibergcenter-edge angle77>20◦,arthroscopycanbeusedforrepairingthelabral
lesion.Incasesofanglessmallerthan20◦,arthroscopyis
con-traindicatedandcanbeusedasacoadjuvantforlabralrepair, duringoraftertreatmentaimedatcorrectingtheacetabular coverage.78
Chondrallesions
Chondrallesionsofthehipmaybeacute,chronicor degenera-tive,withpartialorfulldepth.Theymayresultfromrepetitive trauma,directtrauma,FAI,dysplasiaorosteonecrosisofthe femoralhead.38
There are several options for arthroscopic treatment. Amongthesearemicrofracturing,debridementthrough abra-sion,osteochondralautologoustransplantation(mosaicplasty orosteochondralautologoustransfersystem,OATS), autolo-goustransplantationofchondrocytes,autologous chondroge-nesisinducedbymatrix,freshosteochondraltransplantation andosteochondroplastyofperipherallesionsoftheacetabular rim.79–82Thelong-termresultsandsuperiorityofonemethod
overtheothershavenotyetbeenestablished.83Itisimportant
toemphasizethattheindicationforarthroscopyincasesof osteonecrosismaybetoevaluatechondralandlabrallesions andassistinsurgeryandstaging,andnotasspecifictherapy throughthismethod.Itsindicationshouldbelimited.84,85
Synovectomyandjointbiopsy
Hiparthroscopycanbeusedforsynovectomyand synovial biopsies,anditisfrequentlyindicatedincasesof rheumato-logicalconditionsanddoneonanoutpatientbasis.65,86
Instability
Traumatic
Hipinstabilitymayresultfromlow-energytraumawith sub-luxationofthehip,orcomprisedislocationduetohigh-energy trauma.Removaloffreebodiesisthemainindication,87but
arthroscopycanalsobeusedfortreatingchondralandlabral lesions.88
Non-traumatic
Hipinstabilitymayresultfromcapsule-ligamentlaxityand consequentinjuryofthechondrolabralorosteochondral com-plexofthe acetabulum.Patients who havediseases ofthe connectivetissue,suchasEhlers–Danlosdiseaseoridiopathic capsule-ligamentlaxity,orwhoperformactivitiesthatrequire range of motion greater than what is physiologically nor-mal,suchasballetdancers,may developsymptomatichip instability.89–91
Theclinical picture generally comprises anteriorand/or posteriorhippain,whichmaybeassociatedwithmechanical symptomsandasensationofbeing“outofplace”.Excessive externalrotationofthe hip whenindorsal decubitus,and othersignsofextremelaxitymaybepresent,withorwithout associatedpain.92
Fig.3–Notetheappearanceofthetendonoftheiliopsoas
muscleonmagneticresonanceimagingandthebone
deformationcausedtothefemoralhead,seenon
tomography.
Thearthroscopictreatmentconsistsofrepairingthelesion ofthechondrolabralorosteochondralcomplex.Thereisthe possibilityoftensioningbymeansofsuturesorbyusingradio frequenciesontheanteriorcapsule,withtheaimof diminish-ingtheanteriorinstability.89
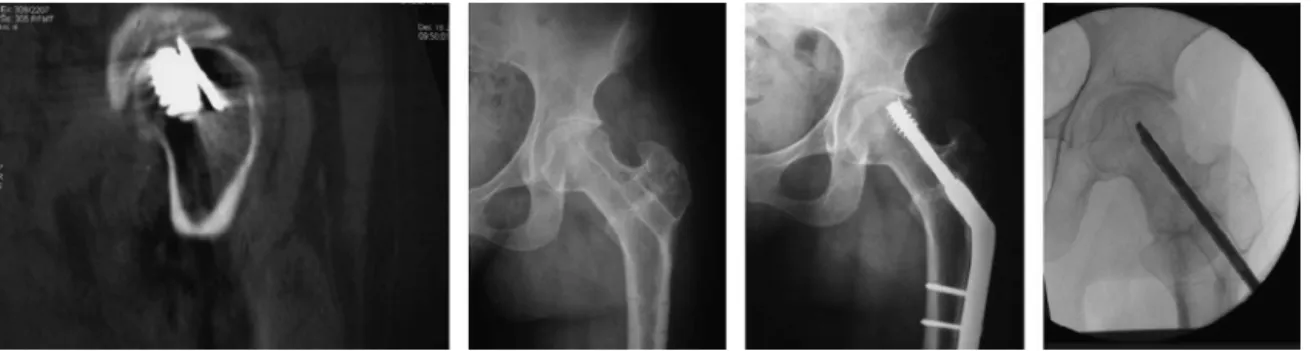
Aidfortreatinghipfractures
Itcanbeusedasanaidforfixingfracturesoftheacetabulum andfemoralhead.93–96 Itisatoolforviewingthereduction,
analyzingscrewpenetrationandremovingfreebodies.
Injuriesoftheroundligament
Theroundligamentisapotentialcauseofhippain.97Itmay
becometornthroughtraumaticcausesorinstability.98
Arthro-scopicdebridementmayleadtopainrelief.99Thepossibility
ofreconstructionusingagraftisdescribedintheliterature,100
butthelong-termresultsareunknown.
Post-arthroplasty
Casesofpersistentpainsubsequent toarthroplastycanbe investigated and/or treated by means of arthroscopy. The indicationsinclude:tendinitisofthetendonoftheiliopsoas muscle due to impingement at the edge of the acetabu-lar component, acute prosthetic infection, investigation of breakage or loosening of the polyethylene, pseudotumors, corrosion atthe head–neck junction ofthe prosthesis and instability.50,101–107
Peritrochantericspace
Extra-articularendoscopyhasevolvedoverrecentyears, espe-ciallythroughstudiesonconditionsthatcausetrochanteric painsyndromeanddeepglutealpainsyndrome.8
Deepglutealpain
glutealregion.Piriformsyndromecanbeconsideredtobeone ofthecausesofdeepglutealpain.108,109Arthroscopic
neurol-ysisofthesciaticnervehasbeendescribedincasesoffailure ofconservativetreatment,withgoodresults.10,110
Trochantericpainsyndrome
Trochanteric pain syndrome is the term used to describe chronicpaininthelateralregionofthehip.Thereareseveral causalfactors,suchasinjuriesofthetendonofthegluteus mediusandminimusmuscles,trochantericbursitisand exter-nalsnapping.
Injuriesofthegluteusmediusandminimus
Injuriestothegluteusmediusandminimusareanalogousto injuriesoftherotator cuffofthe shoulder,which are both associatedwithadvanced ageand degenerative alterations ofthetendons.111,112Theclinicalconditiongenerallyconsists
oflateralpaininthehipthatdoesnotrespondto conserva-tivetreatmentandmaybeassociatedwithweaknessofthe abductorsandapositiveTrendelenburgsign.Ifconservative treatmentfails,endoscopicrepairofthetendonsaffectedcan beperformed.113,114
Lateral(external)snapping
Externalsnappingisdefinedasanaudibleorpalpable snap-ping sensation in the trochanteric region during flexion andextensionofthehip,commonlyobservedamong long-distancerunners. Itoccurs when the posterior part ofthe iliotibialbandortheanteriorpartofthetendonofthe glu-teusmaximusslidesoverthetrochanterduringhipflexion. Whenthehipisthenextended,thesestructuresmaycollide againstthegreatertrochanterandcauseaudible,palpableand painfulsnapping.Ifconservativetreatmentfails,endoscopic treatmentcanbeperformedwiththeobjectiveofdiminishing thetensionofthesestructuresabovethegreatertrochanter. Ilizaliturrietal.115describedcreationofadefectinthe
iliotib-ialbandabovethegreatertrochanter,with90%resolutionof thesnappingandpain.Poleselloetal.116describedendoscopic
tenotomyofthegluteusmaximus,with88%resolutionofthe snappingandlateralpain.
Bursectomy
Theclinicalpictureoftrochantericbursitiscompriseschronic pain over the lateral regionof the greater trochanter.Pain on palpation is characteristic. In cases that are refractory to conservative treatment, endoscopic bursectomy can be performed.117–120Itisimportanttoemphasizethatthe
diag-nosisoftrochantericbursitisneedstohavespecialattention, given that because of lack of knowledge of the differen-tial diagnoses, other causes of pain in the region may go unnoticed.8,121
Hamstringtendons
Hamstringinjuriesmayrangefrommuscledistensionto com-pleteavulsion.Differentopentechniquesforreinsertionhave beendescribed,althoughthepossibilityofarthroscopic
rein-sertionalsoexists.122,123Ithasbeenreportedthatearlyrepair
has better resultsthan laterepair, especiallyamong high-performanceathletes.124
Adjuvantinfemoralorperiacetabularosteotomyfor dysplasiaandcomplexdeformitiesofthehip
There is a discussion in the literature regarding the indi-cations for hip arthroscopy before or after osteotomy, especially in relation to Ganz’s periacetabular osteotomy. Thosewhoadvocatearthroscopystatethatassociated treat-ment for joint lesions would be beneficial.125,126 On the
other hand,it hasbeenobservedthatalargeproportionof thepatientswhoundergo periacetabularosteotomyremain asymptomaticaftertheoperation,withouttheneedforany newintervention.126,127
Children
Hiparthroscopyforchildrenhasgainedprominentspaceover recentyears.39,128–131Itsindicationsinclude:investigationof
thepediatrichip;biopsy;jointcleaning;septicarthritis43;hip
dysplasia,whichcouldbeforthepurposesofjointcleaning tofacilitatereduction,assistinginpelvicosteotomy, explor-ingjointincongruence,performingdebridementofthelabrum andcartilagefragments,orreleasingfibrosisafterthe opera-tion;Legg–Calvé–Perthesdisease,forremovaloffreebodies, synovectomy, debridement of the round ligament, labrum or cartilage fragments and treatment of femoroacetabular impingement; tenotomy ofthe iliopsoas; epiphysiolysis, to treatFAIoraidinremovingbrokenscrews59;andtrapezoidal
osteotomyofthefemoralneck.132
Conflicts
of
interest
Theauthorsdeclarethattherewerenoconflictsofinterest.
Acknowledgements
TheauthorsthankDr.SheilaIngham,forhelpinrevisingthe text.
r
e
f
e
r
e
n
c
e
s
1.PoleselloGC,NakaoTS,QueirozMCd,DaniachiD,Ricioli JuniorW,GuimarãesRP,etal.Propostadepadronizac¸ãodo estudoradiográficodoquadriledapelve.RevBrasOrtop. 2011;46(6):634–42.
2.LynchTS,TerryMA,BediA,KellyBT.Hiparthroscopic surgery:patientevaluation,currentindications,and outcomes.AmJSportsMed.2013;41(5):1174–89.
3.BediA,KellyBT,KhandujaV.Arthroscopichippreservation surgery:currentconceptsandperspective.BoneJointJ. 2013;95-B(1):10–9.
4.ByrdJW.Hiparthroscopyutilizingthesupineposition. Arthroscopy.1994;10(3):275–80.
6. ByrdJW,ChernKY.Tractionversusdistensionfordistraction ofthejointduringhiparthroscopy.Arthroscopy.
1997;13(3):346–9.
7. DienstM,GöddeS,SeilR,HammerD,KohnD.Hip arthroscopywithouttraction:invivoanatomyofthe peripheralhipjointcavity.Arthroscopy.2001;17(9):924–31.
8. VerhelstL,GuevaraV,DeSchepperJ,VanMelkebeekJ, PattynC,AudenaertEA.Extra-articularhipendoscopy:a reviewoftheliterature.BoneJointRes.2012;1(12):324–32.
9. GriffithsEJ,KhandujaV.Hiparthroscopy:evolution,current practiceandfuturedevelopments.IntOrthop.
2012;36(6):1115–21.
10.MartinHD,ShearsSA,JohnsonJC,SmathersAM,PalmerIJ. Theendoscopictreatmentofsciaticnerveentrapment/deep glutealsyndrome.Arthroscopy.2011;27(2):172–81.
11.DvorakM,DuncanCP,DayB.Arthroscopicanatomyofthe hip.Arthroscopy.1990;6(4):264–73.
12.RobertsonWJ,KellyBT.Thesafezoneforhiparthroscopy:a cadavericassessmentofcentral,peripheral,andlateral compartmentportalplacement.Arthroscopy.
2008;24(9):1019–26.
13.SussmannPS,RanawatAS,ShehaanM,LorichD,PadgettDE, KellyBT.Vascularpreservationduringarthroscopic osteoplastyofthefemoralhead–neckjunction:acadaveric investigation.Arthroscopy.2007;23(7):738–43.
14.GautierE,GanzK,KrügelN,GillT,GanzR.Anatomyofthe medialfemoralcircumflexarteryanditssurgical
implications.JBoneJointSurgBr.2000;82(5):679–83.
15.KellyBT,WeilandDE,SchenkerML,PhilipponMJ.
Arthroscopiclabralrepairinthehip:surgicaltechniqueand reviewoftheliterature.Arthroscopy.2005;21(12):1496–504.
16.FergusonSJ,BryantJT,GanzR,ItoK.Aninvitro investigationoftheacetabularlabralsealinhipjoint mechanics.JBiomech.2003;36(2):171–8.
17.FergusonSJ,BryantJT,GanzR,ItoK.Theinfluenceofthe acetabularlabrumonhipjointcartilageconsolidation:a poroelasticfiniteelementmodel.JBiomech.
2000;33(8):953–60.
18.KimYT,AzumaH.Thenerveendingsoftheacetabular labrum.ClinOrthopRelatRes.1995;(320):176–81.
19.WengerDE,KendellKR,MinerMR,TrousdaleRT.Acetabular labraltearsrarelyoccurintheabsenceofbony
abnormalities.ClinOrthopRelatRes.2004;(426): 145–50.
20.KimKC,HwangDS,LeeCH,KwonST.Influenceof femoroacetabularimpingementonresultsofhip arthroscopyinpatientswithearlyosteoarthritis.Clin OrthopRelatRes.2007;456:128–32.
21.ItoK,LeunigM,GanzR.Histopathologicfeaturesofthe acetabularlabruminfemoroacetabularimpingement.Clin OrthopRelatRes.2004;(429):262–71.
22.IkedaT,AwayaG,SuzukiS,OkadaY,TadaH.Tornacetabular labruminyoungpatients.Arthroscopicdiagnosisand management.JBoneJointSurgBr.1988;70(1):13–6.
23.McCarthyJC,NoblePC,SchuckMR,WrightJ,LeeJ,TheOtto E,Aufrancaward:theroleoflabrallesionstodevelopmentof earlydegenerativehipdisease.ClinOrthopRelatRes. 2001;(393):25–37.
24.PoleselloGC,CinagawaEHT,CruzPDSS,QueirozMCd, BorgesCJ,RicioliJuniorW,etal.Tratamentocirúrgicopara impactofemoroacetabularemumgrupoquerealiza agachamento.RevBrasOrtop.2012;47(4):488–92.
25.PoleselloGC,OnoNK,BellanDG,HondaEK,GuimarãesRP, RiccioliJuniorW,etal.Artroscopiadoquadrilematletas. RevBrasOrtop.2009;44(1):26–31.
26.PoleselloGC,QueirozMC,OnoNK,HondaEK,GuimarãesRP, RicioliJuniorW.Tratamentoartroscópicodoimpacto femoroacetabular.RevBrasOrtop.2009;44(3):230–8.
27.ByrdJW,JonesKS.Arthroscopicmanagementof femoroacetabularimpingementinathletes.AmJSports Med.2011;39Suppl.:7S–13S.
28.ByrdJW,JonesKS.Hiparthroscopyinathletes:10-year follow-up.AmJSportsMed.2009;37(11):2140–3.
29.DombBG,BrooksAG,ByrdJW.Clinicalexaminationofthe hipjointinathletes.JSportRehabil.2009;18(1):3–23.
30.LarsonCM,GiveansMR.Arthroscopicdebridementversus refixationoftheacetabularlabrumassociatedwith femoroacetabularimpingement.Arthroscopy. 2009;25(4):369–76.
31.LarsonCM,GiveansMR,StoneRM.Arthroscopic debridementversusrefixationoftheacetabularlabrum associatedwithfemoroacetabularimpingement:mean 3.5-yearfollow-up.AmJSportsMed.2012;40(5):1015–21.
32.MatsudaDK,BurchetteRJ.Arthroscopichiplabral reconstructionwithagracilisautograftversuslabral refixation:2-yearminimumoutcomes.AmJSportsMed. 2013;41(5):980–7.
33.SierraRJ,TrousdaleRT.Labralreconstructionusingthe ligamentumterescapitis:reportofanewtechnique.Clin OrthopRelatRes.2009;467(3):753–9.
34.PhilipponMJ,BriggsKK,HayCJ,KuppersmithDA,Dewing CB,HuangMJ.Arthroscopiclabralreconstructioninthehip usingiliotibialbandautograft:techniqueandearly outcomes.Arthroscopy.2010;26(6):750–6.
35.GanzR,ParviziJ,BeckM,LeunigM,NötzliH,SiebenrockKA. Femoroacetabularimpingement:acauseforosteoarthritis ofthehip.ClinOrthopRelatRes.2003;(417):112–20.
36.GanzR,LeunigM,Leunig-GanzK,HarrisWH.Theetiology ofosteoarthritisofthehip:anintegratedmechanical concept.ClinOrthopRelatRes.2008;466(2):264–72.
37.BediA,KellyBT.Femoroacetabularimpingement.JBone JointSurgAm.2013;95(1):82–92.
38.BeckM,KalhorM,LeunigM,GanzR.Hipmorphology influencesthepatternofdamagetotheacetabularcartilage: femoroacetabularimpingementasacauseofearly
osteoarthritisofthehip.JBoneJointSurgBr. 2005;87(7):1012–8.
39.KocherMS,KimYJ,MillisMB,MandigaR,SiparskyP,Micheli LJ,KasserJR.Hiparthroscopyinchildrenandadolescents.J PediatrOrthop.2005;25(5):680–6.
40.PhilipponMJ,SchenkerML.Arthroscopyforthetreatmentof femoroacetabularimpingementintheathlete.ClinSports Med.2006;25(2):299–308.
41.SampsonTG.Arthroscopictreatmentoffemoroacetabular impingement:aproposedtechniquewithclinical experience.InstrCourseLect.2006;55:337–46.
42.El-SayedAM.ResponsetoUriGivonTreatmentofearly septicarthritisofthehipinchildren:comparisonofresults ofopenarthrotomyversusarthroscopicdrainage.JChild Orthop.2008;2(6):497.
43.ChungWK,SlaterGL,BatesEH.Treatmentofsepticarthritis ofthehipbyarthroscopiclavage.JPediatrOrthop.
1993;13(4):444–6.
44.KimSJ,ChoiNH,KoSH,LintonJA,ParkHW.Arthroscopic treatmentofsepticarthritisofthehip.ClinOrthopRelat Res.2003;(407):211–4.
45.NusemI,JaburMK,PlayfordEG.Arthroscopictreatmentof septicarthritisofthehip.Arthroscopy.2006;22(8):902.e1–3.
46.BouldM,EdwardsD,VillarRN.Arthroscopicdiagnosisand treatmentofsepticarthritisofthehipjoint.Arthroscopy. 1993;9(6):707–8.
47.BlitzerCM.Arthroscopicmanagementofsepticarthritisof thehip.Arthroscopy.1993;9(4):414–6.
49.LeeYK,ParkKS,HaYC,KooKH.Arthroscopictreatmentfor acutesepticarthritisofthehipjointinadults.KneeSurg SportsTraumatolArthrosc.2012[Epubaheadofprint].
50.HymanJL,SalvatiEA,LaurencinCT,RogersDE,MaynardM, BrauseDB.Thearthroscopicdrainage,irrigation,and debridementoflate,acutetotalhiparthroplastyinfections: average6-yearfollow-up.JArthroplasty.1999;14(8):903–10.
51.LarsonCM,GiveansMR,TaylorM.DoesarthroscopicFAI correctionimprovefunctionwithradiographicarthritis? ClinOrthopRelatRes.2011;469(6):1667–76.
52.WaltonNP,JahromiI,LewisPL.Chondraldegenerationand therapeutichiparthroscopy.IntOrthop.2004;28(6):354–6.
53.McCarthyJC,LeeJA.Arthroscopicinterventioninearlyhip disease.ClinOrthopRelatRes.2004;(429):157–62.
54.TönnisD,HeineckeA.Acetabularandfemoralanteversion: relationshipwithosteoarthritisofthehip.JBoneJointSurg Am.1999;81(12):1747–70.
55.HorisbergerM,BrunnerA,HerzogRF.Arthroscopic treatmentoffemoroacetabularimpingementofthehip:a newtechniquetoaccessthejoint.ClinOrthopRelatRes. 2010;468(1):182–90.
56.IlizaliturriJrVM.Complicationsofarthroscopic
femoroacetabularimpingementtreatment:areview.Clin OrthopRelatRes.2009;467(3):760–8.
57.TelokenMA,SchmietdI,TomlinsonDP.Hiparthroscopy:a uniqueinferomedialapproachtobulletremoval.
Arthroscopy.2002;18(4):E21.
58.SchindlerA,LechevallierJJ,RaoNS,BowenJR.Diagnostic andtherapeuticarthroscopyofthehipinchildrenand adolescents:evaluationofresults.JPediatrOrthop. 1995;15(3):317–21.
59.IlizaliturriJrVM,Zarate-KalfopulosB,Martinez-Escalante FA,Cuevas-OlivoR,Camacho-GalindoJ.Arthroscopic retrievalofabrokenguidewirefragmentfromthehipjoint aftercannulatedscrewfixationofslippedcapitalfemoral epiphysis.Arthroscopy.2007;23(2):e1–4,227.
60.SozenYV,PolatG,KadiogluB,DikiciF,OzkanK,UnayK. Arthroscopicbulletextractionfromthehipinthelateral decubitusposition.HipInt.2010;20(2):265–8.
61.GuptaRK,AggarwalV.Latearthroscopicretrievalofabullet fromhipjoint.IndianJOrthop.2009;43(4):416–9.
62.LeeGH,VirkusWW,KapotasJS.Arthroscopicallyassisted minimallyinvasiveintraarticularbulletextraction: technique,indications,andresults.JTrauma. 2008;64(2):512–6.
63.SingletonSB,JoshiA,SchwartzMA,CollingeCA. Arthroscopicbulletremovalfromtheacetabulum. Arthroscopy.2005;21(3):360–4.
64.PoleselloGC,OnoNK,HondaEK,GuimarãesRP,RicioliJunior W,SouzaBGS,etal.Tratamentoartroscópicoda
osteocondromatosesinovialnoquadril.RevBrasOrtop. 2009;44(4):320–3.
65.KrebsVE.Theroleofhiparthroscopyinthetreatmentof synovialdisordersandloosebodies.ClinOrthopRelatRes. 2003;(406):48–59.
66.ZiniR,LongoUG,deBenedettoM,LoppiniM,CarraroA, MaffulliN,DenaroV.Arthroscopicmanagementofprimary synovialchondromatosisofthehip.Arthroscopy.
2013;29(3):420–6.
67.LeeJB,KangC,LeeCH,KimPS,HwangDS.Arthroscopic treatmentofsynovialchondromatosisofthehip.AmJ SportsMed.2012;40(6):1412–8.
68.MarchieA,PanuncialmanI,McCarthyJC.Efficacyofhip arthroscopyinthemanagementofsynovial
chondromatosis.AmJSportsMed.2011;39Suppl.: 126S–31S.
69.BoyerT,DorfmannH.Arthroscopyinprimarysynovial chondromatosisofthehip:descriptionandoutcomeof treatment.JBoneJointSurgBr.2008;90(3):314–8.
70.AlvarezMS,MoneoPR,PalaciosJA.Arthroscopicextirpation ofanosteoidosteomaoftheacetabulum.Arthroscopy. 2001;17(7):768–71.
71.ChangBK,HaYC,LeeYK,HwangDS,KooKH.Arthroscopic excisionofosteoidosteomaintheposteroinferiorportionof theacetabulum.KneeSurgSportsTraumatolArthrosc. 2010;18(12):1685–7.
72.KhapchikV,O’DonnellRJ,GlickJM.Arthroscopicallyassisted excisionofosteoidosteomainvolvingthehip.Arthroscopy. 2001;17(1):56–61.
73.SchrödereSouzaBG,DaniWS,HondaEK,RicioliW, GuimarãesRP,OnoNK,etal.Enblocarthroscopicresection ofosteoidosteomainthehip:areportoffourpatientsand literaturereview.CurrOrthopPract.2010;21(3):320–6.
74.IlizaliturriJrVM,VillalobosJrFE,ChaidezPA,ValeroFS, AguileraJM.Internalsnappinghipsyndrome:treatmentby endoscopicreleaseoftheiliopsoastendon.Arthroscopy. 2005;21(11):1375–80.
75.ContrerasME,DaniWS,EndgesWK,DeAraujoLC,BerralFJ. Arthroscopictreatmentofthesnappingiliopsoastendon throughthecentralcompartmentofthehip:apilotstudy.J BoneJointSurgBr.2010;92(6):777–80.
76.LeunigM,PodeszwaD,BeckM,WerlenS,GanzR.Magnetic resonancearthrographyoflabraldisordersinhipswith dysplasiaandimpingement.ClinOrthopRelatRes. 2004;(418):74–80.
77.WibergG.Studiesondysplasticacetabulaandcongenital subluxationofthehipjoint.ActaOrthopScandSuppl. 1939;83(58):5–135.
78.ByrdJW,JonesKS.Hiparthroscopyinthepresenceof dysplasia.Arthroscopy.2003;19(10):1055–60.
79.YenYM,KocherMS.Chondrallesionsofthehip:
microfractureandchondroplasty.SportsMedArthroscRev. 2010;18(2):83–9.
80.FontanaA.Anoveltechniquefortreatingcartilagedefects inthehip:afullyarthroscopicapproachtousingautologous matrix-inducedchondrogenesis.ArthroscTechn.
2012;1(1):e63–8.
81.AkimauP,BhosaleA,HarrisonPE,RobertsS,McCallIW, RichardsonJB,etal.Autologouschondrocyteimplantation withbonegraftingforosteochondraldefectdueto posttraumaticosteonecrosisofthehip–acasereport.Acta Orthop.2006;77(2):333–6.
82.EllenderP,MinasT.Autologouschondrocyteimplantationin thehip:casereportandtechnique.OperTechnSportsMed. 2008;16(4):201–6.
83.FontanaA,BistolfiA,CrovaM,RossoF,MassazzaG. Arthroscopictreatmentofhipchondraldefects:autologous chondrocytetransplantationversussimpledebridement–a pilotstudy.Arthroscopy.2012;28(3):322–9.
84.RuchDS,SekiyaJ,DicksonSchaeferW,KomanLA,PopeTL, PoehlingGG.Theroleofhiparthroscopyintheevaluationof avascularnecrosis.Orthopedics.2001;24(4):339–43.
85.EllenriederM,TischerT,KreuzPC,FrohlichS,FritscheA, MittelmeierW.Arthroscopicallyassistedtherapyof avascularnecrosisofthefemoralhead.OperOrthop Traumatol.2013;25(1):85–94.
86.DorfmannH,BoyerT.Arthroscopyofthehip:12yearsof experience.Arthroscopy.1999;15(1):67–72.
87.MullisBH,DahnersLE.Hiparthroscopytoremoveloose bodiesaftertraumaticdislocation.JOrthopTrauma. 2006;20(1):22–6.
88.PhilipponMJ,KuppersmithDA,WolffAB,BriggsKK. Arthroscopicfindingsfollowingtraumatichipdislocationin 14professionalathletes.Arthroscopy.2009;25(2):169–74.
90.ShuB,SafranMR.Hipinstability:anatomicandclinical considerationsoftraumaticandatraumaticinstability.Clin SportsMed.2011;30(2):349–67.
91.DuthonVB,CharbonnierC,KoloFC,Magnenat-ThalmannN, BeckerCD,BouvetC,etal.Correlationofclinicaland magneticresonanceimagingfindingsinhipsofelitefemale balletdancers.Arthroscopy.2013;29(3):411–9.
92.ShindleMK,RanawatAS,KellyBT.Diagnosisand
managementoftraumaticandatraumatichipinstabilityin theathleticpatient.ClinSportsMed.2006;25(2):309–26.
93.MatsudaDK,rarefractureA.anevenrarertreatment:the arthroscopicreductionandinternalfixationofanisolated femoralheadfracture.Arthroscopy.2009;25(4):408–12.
94.YamamotoY,IdeT,OnoT,HamadaY.Usefulnessof arthroscopicsurgeryinhiptraumacases.Arthroscopy. 2003;19(3):269–73.
95.LansfordT,MunnsSW.ArthroscopictreatmentofPipkin typeIfemoralheadfractures:areportof2cases.JOrthop Trauma.2012;26(7):e94–6.
96.GotzLP,SchulzR.Arthroscopicallycontrolledscrew placementforosteosynthesisofacetabularfractures. Unfallchirurg.2013;116(11):1033–5.
97.WettsteinM,GarofaloR,BorensO,MouhsineE.Traumatic ruptureoftheligamentumteresasasourceofhippain. Arthroscopy.2005;21(3):382.
98.KusmaM,JungJ,DienstM,GoeddeS,KohnD,SeilR. Arthroscopictreatmentofanavulsionfractureofthe ligamentumteresofthehipinan18-year-oldhorserider. Arthroscopy.2004;20Suppl.2:64–6.
99.HavivB,O’DonnellJ.Arthroscopicdebridementofthe isolatedLigamentumTeresrupture.KneeSurgSports TraumatArthrosc.2011;19(9):1510–3.
100.PhilipponMJ,PennockA,GaskillTR.Arthroscopic
reconstructionoftheligamentumteres:techniqueandearly outcomes.JBoneJointSurgBr.2012;94(11):1494–8.
101.FontanaA,ZeccaM,SalaC.Arthroscopicassessmentof totalhipreplacementandpolyethylenewear:acasereport. KneeSurgSportsTraumatArthrosc.2000;8(4):244–5.
102.KhandujaV,VillarRN.Theroleofarthroscopyinresurfacing arthroplastyofthehip.Arthroscopy.2008;24(1),122e1–3.
103.McCarthyJC,JibodhSR,LeeJA.Theroleofarthroscopyin evaluationofpainfulhiparthroplasty.ClinOrthopRelatRes. 2009;467(1):174–80.
104.CuellarR,AguinagaI,CorcueraI,PonteJ,UsabiagaJ. Arthroscopictreatmentofunstabletotalhipreplacement. Arthroscopy.2010;26(6):861–5.
105.VanRietA,DeSchepperJ,DelportHP.Arthroscopicpsoas releaseforiliopsoasimpingementaftertotalhip replacement.ActaOrthopaBelg.2011;77(1):41–6.
106.PattynC,VerdonkR,AudenaertE.Hiparthroscopyin patientswithpainfulhipfollowingresurfacingarthroplasty. KneeSurgSportsTraumatArthrosc.2011;19(9):1514–20.
107.BajwaAS,VillarRN.Arthroscopyofthehipinpatients followingjointreplacement.JBoneJointSurgBr. 2011;93(7):890–6.
108.HwangDS,KangC,LeeJB,ChaSM,YeonKW.Arthroscopic treatmentofpiriformissyndromebyperineuralcystonthe sciaticnerve:acasereport.KneeSurgSportsTraumat Arthrosc.2010;18(5):681–4.
109.DezawaA,KusanoS,MikiH.Arthroscopicreleaseofthe piriformismuscleunderlocalanesthesiaforpiriformis syndrome.Arthroscopy.2003;19(5):554–7.
110.PoleselloGC,QueirozMC,LinharesJPT,AmaralDT,OnoNK. Variac¸ãoanatômicadomúsculopiriformecomocausade dorglúteaprofunda:diagnósticoporneurografiaRMeseu tratamento.RevBrasOrtop.2013;48(1):114–7.
111.BunkerTD,EslerCN,LeachWJ.Rotator-cufftearofthehip.J BoneJointSurgBr.1997;79(4):618–20.
112.KaganA.Rotatorcufftearsofthehip.ClinOrthopRelatRes. 1999;(368):135–40.
113.VoosJE,ShindleMK,PruettA,AsnisPD,KellyBT.Endoscopic repairofgluteusmediustendontearsofthehip.AmJSports Med.2009;37(4):743–7.
114.LachiewiczPF.Abductortendontearsofthehip:evaluation andmanagement.JAmAcadOrthopSurg.2011;19(7):385–91.
115.IlizaliturriJrVM,Martinez-EscalanteFA,ChaidezPA, Camacho-GalindoJ.Endoscopiciliotibialbandreleasefor externalsnappinghipsyndrome.Arthroscopy.
2006;22(5):505–10.
116.PoleselloGC,QueirozMC,DombBG,OnoNK,HondaEK. Surgicaltechnique:endoscopicgluteusmaximustendon releaseforexternalsnappinghipsyndrome.ClinlOrthop RelatRes.2013;471(8):2471–6.
117.FoxJL.Theroleofarthroscopicbursectomyinthetreatment oftrochantericbursitis.Arthroscopy.2002;18(7):E34.
118.WieseM,RubenthalerF,WillburgerRE,FennesS,HaakerR. Earlyresultsofendoscopictrochanterbursectomy.Int Orthop.2004;28(4):218–21.
119.BakerJrCL,MassieRV,HurtWG,SavoryCG.Arthroscopic bursectomyforrecalcitranttrochantericbursitis. Arthroscopy.2007;23(8):827–32.
120.FarrD,SelesnickH,JaneckiC,CordasD.Arthroscopic bursectomywithconcomitantiliotibialbandreleaseforthe treatmentofrecalcitranttrochantericbursitis.Arthroscopy. 2007;23(8):e1–5,905.
121.HoGW,HowardTM.Greatertrochantericpainsyndrome: morethanbursitisandiliotibialtractfriction.CurrSports MedRep.2012;11(5):232–8.
122.SallayPI,BallardG,HamerslyS,SchraderM.Subjectiveand functionaloutcomesfollowingsurgicalrepairofcomplete rupturesoftheproximalhamstringcomplex.Orthopedics. 2008;31(11):1092.
123.DierckmanBD,GuancheCA.Endoscopicproximal hamstringrepairandischialbursectomy.ArthroscTechn. 2012;1(2):e201–7.
124.SarimoJ,LempainenL,MattilaK,OravaS.Complete proximalhamstringavulsions:aseriesof41patientswith operativetreatment.AmJSportsMed.2008;36(6):1110–5.
125.RossJR,ZaltzI,NeppleJJ,SchoeneckerPL,ClohisyJC. Arthroscopicdiseaseclassificationandinterventionsasan adjunctinthetreatmentofacetabulardysplasia.AmJ SportsMed.2011;39Suppl.:72S–8S.
126.KimKI,ChoYJ,RamtekeAA,YooMC.Peri-acetabular rotationalosteotomywithconcomitanthiparthroscopyfor treatmentofhipdysplasia.JBoneJointSurgBr.
2011;93(6):732–7.
127.FujiiM,NakashimaY,NoguchiY,YamamotoT,MawatariT, MotomuraG,etal.Effectofintra-articularlesionsonthe outcomeofperiacetabularosteotomyinpatientswith symptomatichipdysplasia.JBoneJointSurgBr. 2011;93(11):1449–56.
128.DeAngelisNA,BusconiBD.Hiparthroscopyinthepediatric population.ClinOrthopRelatRes.2003;(406):60–3.
129.JayakumarP,RamachandranM,YoumT,AchanP. Arthroscopyofthehipforpaediatricandadolescent disorders:currentconcepts.JBoneJointSurgBr. 2012;94(3):290–6.
130.RoyDR.Arthroscopyofthehipinchildrenandadolescents.J ChildOrthop.2009;3(2):89–100.
131.BerendKR,VailTP.Hiparthroscopyintheadolescentand pediatricathlete.ClinSportsMed.2001;20(4):
763–78.